KEYWORDS
Intraperitoneal, ovarian cancer, survival, toxicity, treatment
INTRODUCTION
In the Netherlands, 1,300 women are diagnosed with epithelial ovarian cancer (OC) annually.1,2 Most patients are diagnosed with advanced, FIGO stage III disease. Standard therapy consists of either primary debulking surgery (PDS) followed by chemotherapy or neo-adjuvant chemotherapy followed by interval debulking surgery (IDS) and adjuvant chemotherapy. Cytoreductive surgery is centralised and performed in one of the eight Dutch gynaecologic oncology centres specialised in treatment of ovarian cancer. Intravenous (iv) chemotherapy consists of carboplatin and paclitaxel with or without bevacizumab. Median recurrence-free survival (RFS) in advanced stage OC is 12 months and median overall survival (OS) is 24-50 months.3-5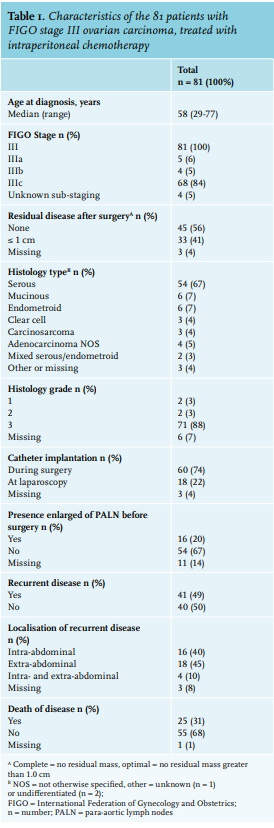
Since 1996, several randomised studies have confirmed the superiority of intraperitoneal (ip) plus iv chemotherapy (iv/ip) over iv chemotherapy alone.5-14 Armstrong et al. showed an improvement in median overall survival from 50 to 66 months for patients receiving iv/ip chemotherapy compared to iv chemotherapy.5,15 This led to a clinical announcement by the United States National Cancer Institute in 2006 recommending iv/ip chemotherapy as treatment of choice for patients with OC with optimal (no residual mass larger than 1.0 cm in diameter) or complete (no visual residual mass) PDS.5,10 Recently, another unpublished randomised trial using a lower dose of ip cisplatin combined with bevacizumab did not find a significant difference in RFS compared to iv carboplatin with weekly paclitaxel and bevacizumab.16 Since OS data are not available and results have not yet been peer reviewed, it is unclear how this study should be valued. Nine randomised trials and three large meta-analyses on ip chemotherapy showed the superiority of ip chemotherapy over iv chemotherapy.6,8,14,17 However, iv/ip administration of chemotherapy is still not common practice.5,10 In the Netherlands, only a few centres treat patients with iv/ip chemotherapy after primary debulking surgery. In particular, the more severe toxicity cases, due to high dose of cisplatin (predominantly renal-, oto- and neurotoxicity), combined with paclitaxel (neurotoxicity), as well as abdominal pain and catheter complications are arguments against iv/ip chemotherapy.5,10 Although iv/ip chemotherapy results in an impaired quality of life during treatment, quality of life recover after termination of iv/ip chemotherapy.5,15
Currently, the most effective evidence-based schedule for iv/ip chemotherapy is the schedule used by Armstrong et al.5 Since 2007, four hospitals from three Dutch gynaecologic oncology centres offer this iv/ip chemotherapy schedule. The aim of this study is to evaluate both toxicity and survival outcomes of iv/ip chemotherapy in daily practice in the Netherlands.
METHODS
Setting and Participants
This observational study was performed in women diagnosed with FIGO stage III OC who had at least an optimal PDS (tumour rests 1 cm or less) and were treated with iv/ip chemotherapy in the Netherlands between January 2007 and May 2016 (n = 81). The in- and exclusion criteria were according to the Armstrong protocol.5 In addition, the decision to give iv/ip chemotherapy was based on clinical condition and co-morbidity.
Procedures
All procedures (chemotherapy, dosage, reductions, discontinuation) have been performed according to the publication of Armstrong et al. (day 1 paclitaxel 135 mg/ m2 in 24 hours iv; day 2: cisplatin 100 mg/m2 ip; and day 8: paclitaxel 60mg/m2 ip, to be repeated every 3 weeks for 6 courses).5 Premedication and anti-emetics were given according to local standard treatment.5 For iv/ip therapy, a peritoneal catheter (9.6 Fr single lumen Bardport) was implanted either during PDS or afterwards by laparoscopic procedure. Ip catheters were removed after completion of treatment.
During consultation with the gynaecologic oncologists and medical oncologist, all eligible patients were informed on procedures of iv/ip chemotherapy, including survival benefit and treatment- related toxicity, after which, in a shared decision process, a choice was made for either iv or iv/ip adjuvant chemotherapy. After surgery, the patients received additional information from the medical oncologist and definitive informed consent was obtained.
Data collection
Retrospective data collection took place in May 2016. Patients have been prospectively registered between January 2007 and May 2016. The following clinical and patient information was obtained from the medical records: age at time of diagnosis, date of diagnosis, histological type of the tumour, surgical outcome after surgery, timing of implanting the abdominal catheter in relation to PDS, duration of follow-up (defined as time period between PDS and database lock), ip catheterrelated morbidity (infection, obstruction, leakage), and chemotherapy related toxicity; nausea/vomiting, abdominal pain, haematological toxicity, electrolyte disturbance, impaired renal function, and neurotoxicity). RFS (defined as time period between PDS and first radiological proof of recurrence) and OS (defined as time period between PDS and death of any cause; this last variable was obtained from the Dutch Population Register). All toxicity was reported and graded according to common terminology criteria for adverse events (CTCAE) v4.0. In accordance with ethical standards, no ethical approval was needed.
Statistical analysis
Descriptive statistics of participants were performed for patient characteristics (table 1); course of iv/ip treatment and related morbidity and toxicity (table 2); and reasons for not completing six courses of chemotherapy (table 3). Cumulative survival analyses were performed from date of surgery with the Kaplan-Meier method (tables 4 and 5) and were compared with previously defined prognostic variables, surgical outcome (complete vs. optimal debulking), number of completed ip courses (1-3 vs. 4-6), age at diagnosis (≤ 60 vs. > 60 yrs), localisation of recurrent disease (intra- vs. extra-peritoneally), presence of enlarged para-aortic lymph nodules (PALN) before surgery (yes vs. no), presence of dose reduction (no vs. yes), and start of chemotherapy (≤ 28 days vs. > 28 days).5,10 Life expectancies were computed for the same groups by using the mortality rates to construct a life table (table 4). All statistical analyses were conducted using IBM SPSS Statistics version 22 (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient characteristics
Of the 89 OC patients who consented to iv/ip treatment, 81 were eligible for analysis. Eight patients were excluded from further analyses: 1 patient because of incomplete data, and 7 (8%) patients did not receive iv/ip chemotherapy. In the three cancer centres, 41, 27 and 13 patients (total n = 81) have been treated, respectively. Reasons not to start this treatment were: diagnosis of FIGO stage IV disease in 2 patients, pre-existent hearing loss in 2 patients precluding cisplatin treatment, post-operative perforation of gastrointestinal tract in 1 patient, post-operative infection in 1 patient, and progression of disease prior to start chemotherapy in 1 patient.
Patient characteristics are summarised in table 1. Median age at the time of diagnosis was 58 (range 29-77) years. All patients were diagnosed with FIGO stage III OC. All women underwent PDS; 45 (56%) had a complete PDS; 33 (41%) had an optimal PDS, of which, 3 (4%), patient information on residual disease after debulking surgery is lacking. The majority of patients were diagnosed with a high-grade serous carcinoma.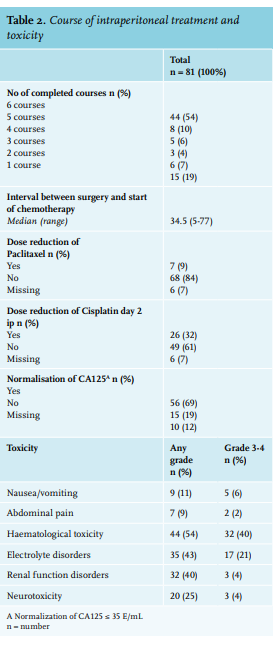
Abdominal catheter: implantation and complications
In 60 patients (74%,) the ip catheter was implanted during PDS, and 18 patients (22%) received the ip catheter during a laparoscopy, of which, patient information for 3 (4%) on catheter implantation is lacking. Seven patients (9%), had ip catheter complications, of whom, 3 (4%) continued iv/ip therapy after replacement of the catheter and 4 (5%) continued with iv therapy only.
Toxicity and morbidity
Toxicity and morbidity due to administration of iv/ip cisplatin and paclitaxel is summarised in table 2. Grade 3-4 toxicity was predominantly haematological (40%) or biochemical (21%). Although renal and neural toxicity was common, it was grade 3-4 in a minority of patients (both 4%). In 50 (62%) patients, no subjective toxicity was documented. Median time between surgery and start of adjuvant treatment was 34 days (range 5-77 days). Forty-four patients (54%) completed all six cycles of chemotherapy. Forty-six percent of the patients (37/81, table 2) discontinued the planned treatment. Reasons for discontinuation of iv/ip chemotherapy are summarised in table 3. Main reasons were impaired renal function, PAC dysfunction, or neurotoxicity. Dose reductions mainly occurred due to the toxicity of cisplatin. Thirty-seven (46%) patients needed at least one dose reduction (7 patients needed a dose reduction of paclitaxel, 26 patients needed a dose reduction of cisplatin ip. For six patients, dose reductions were registered, not specifying which drug. Of all 44 patients who completed the scheduled six cycles of chemotherapy, 19 (43%) needed a dose reduction, most frequently due to toxicity of cisplatin on the second day of treatment (4/16 = 25%, n = 3 missing).
Overall survival and recurrence-free survival
After completion of treatment, 56 (69%) patients had CA-125 normalisation. Median duration of follow-up was 40.0 months (range 4-115 months). One patient was lost to follow-up for survival analyses. During the follow-up period, 41 patients (49%) had recurrent disease and eventually, 25 (31%) patients died. The median RFS and OS were 24 (range 0-108) and 80 (range 4-115) months, respectively. Results of OS are listed in table 4. Those who completed 4 to 6 courses of iv/ip chemotherapy (p = 0.041, figure 1.) and those who had ip localisation of recurrent disease (p = 0.024) had significantly better OS than those who received 3 or fewer courses of iv/ip chemotherapy and those with extra-peritoneal recurrence of OC. All other characteristics were not significant. Those who underwent a complete debulking had significant improvement of RFS compared to those who had an optimal but not complete debulking (p = 0.045). There was no significant association between other factors and outcome variables.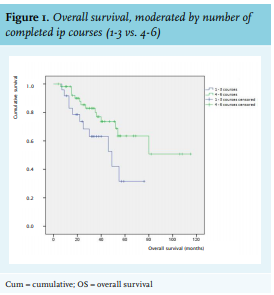
DISCUSSION
In this study, we investigated the use of iv/ip chemotherapy for OC in the Netherlands between January 2007 and May 2016. Four hospitals from three gynaecological cancer centres prescribed ip/iv chemotherapy for a minority of their patients. With the strict selection criteria described by Amstrong et al., results in daily practice were more or less comparable with the study results concerning toxicity and RFS. The reasons for toxicity with iv/ip chemotherapy are two-fold: the dose of ip in the cavity is higher than can be administered iv, and the slow uptake of cisplatin from peritoneal surfaces, results in prolonged systemic exposure.10
Fifty-four percent of the patients diagnosed with FIGO stage III OC who received iv/ip treatment were able to complete six cycles according to the Armstrong regimen. This is not worse than the 42% in the original report of Armstrong et al.,5,10 or the 12.7% reported by Wright et al. It is slightly lower than Schlappe et al., who reported 62% completion,11,12 but they used a different regimen with a lower dose of cisplatin (75 mg/m2 ) and administered carboplatin instead of cisplatin.11 Due to the retrospective character of our study, toxicity data were not always complete. Abdominal pain as a cause for discontinuation of treatment occurred in 9% of the patients, which is similar to other studies.11,18 Other adverse effects were similar to those previously reported.
Catheter complications occurred in 9% of the patients, while Schlappe et al and Walker et al. reported port problems in 9% and 34% of their patients, respectively.11,18 We hypothesise that the better completion rate over time may be due to improved experience with placing and using ip catheters and the centralised care.19 The selection of patients in order to increase completion rate (such as younger age and better performance status) may also have had a substantial role.
Dose reductions in our study were mostly used to decrease the toxicity of cisplatin. Recent studies by Mackay et al. and Hasegawa et al. with ip treatment using carboplatin, showed comparable data for survival and ip port-related toxicity, but less systemic toxicity.20-23 Carboplatin instead of cisplatin in ip treatment for epithelial ovarian cancer may thus be a better alternative in terms of toxicity, but efficacy is unproven. Preclinical studies have shown that the tumour penetration of cisplatin is better than carboplatin, suggesting a pharmacokinetic advantage of cisplatin over carboplatin in achieving local high concentrations such as in ip administration.24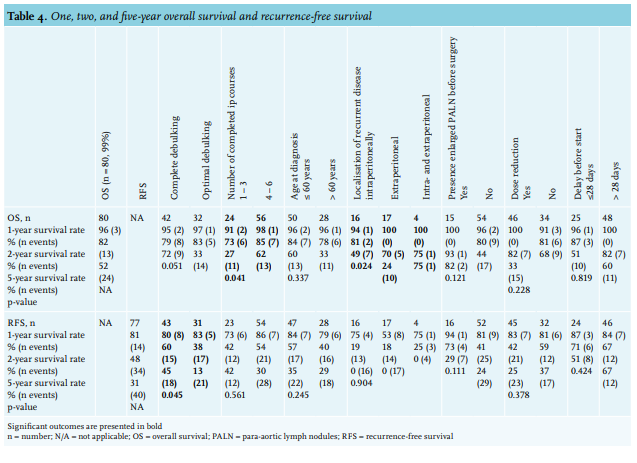
A recent study of Walker et al.25 revealed no advantage to the use of the modified ip cisplatin regimen compared with the more conventional iv drug administration. It is noteworthy that in this study, cisplatin was administered in a dose of 75 mg/m2 instead of 100 mg/m2 and was also combined with bevacizumab. Moreover, recent studies revealed that addition of bevacizumab (VEGF-inhibitor) to the standard three weekly carboplatin paclitaxel has similar survival rates but with less toxicity (less sensory neuropathy).25,26 New treatment strategies with, for example, maintenance parp inhibitors combined with other targeted agents may improve the prognosis of OC in the near future, hopefully leading to less (long-term) toxicity.
The presence of PALN during debulking surgery and information on catheter implantation are important prognostic and therapeutic criteria to select patients eligible for ip treatment. PALN might be a sanctuary side for the ip chemotherapy27 and during second look catheter implantations, presence adhesions could be an indication of potential treatment failure.28,29 It is to be expected that in the near future a personalised treatment plan, predicted by tumour and personal characteristics, will further improve the cure and care of these patients. The use of iv/ip treatment should then be reassessed.
Unfortunately, we did not record information on patient experience. The study of Walker et al. reported that patients who received ip treatment experienced significantly worse symptoms, especially abdominal discomfort.18 IP treatment results in an impaired quality of life during treatment; however, this recovers after termination of therapy. It would have been interesting to evaluate this in daily practice.
As toxicity is the main drawback of iv/ip chemotherapy, research to mitigate this is important. Prior research showed that co-administration of epinephrine and cisplatin might lead to a decrease of toxicity. IP administration of epinephrine increases the penetration of platinum derivatives into tumours.30 However this does not seem common practice in iv/ip chemotherapy. Another way to decrease toxicity might be the use of thiosulphate. Within minutes after administration of cisplatin, the highly toxic monoaqua hydrolysis complex (MHC) is formed.31 Thiosulphate modulates the metabolism of cisplatin in plasma by rapidly reacting with the MHC to form platinum-sulfur complexes.31 By using thiosulphate as a possible chemoprotective agent in animal studies, toxicity of cisplatin was reduced, often without appreciably affecting its anticancer efficiency.31,32 Thiosulphate was also used in the recent published HIPEC trial of van Driel et al.33,34 Prospective studies with epinephrine and thiosulphate in iv/ip are warranted in order to investigate possible decrease of toxicity of iv/ip treatment in OC.
HIPEC with cisplatin after primary debulking may be another strategy to improve outcome after primary debulking surgery in the light of the recently published positive results of HIPEC after interval debulking. A study protocol for this is under development.20,21,35 We did not find evidence of a difference in RFS and OS for older patients, although drug metabolism and renal function may be impaired in the elderly (even in the presence of creatinine levels within the normal range).36 This seems to justify treatment with this regimen on the basis of functional status rather than age alone. Many patients considered candidates for iv/ip chemotherapy (based on disease characteristics) in the Netherlands do not receive this treatment.
In order to estimate the potential population which could be candidate for iv/ip chemotherapy, we assessed the number of patients with FIGO stage III and optimal or complete debulking registered in the Netherlands Cancer Registry (NCR) in the comprehensive cancer centres of the hospitals providing iv/ip chemotherapy in the same period. After linking the eligibility criteria of our study to the NCR data, n = 1447 women with FIGO stage III disease were registered who had at least an optimal PDS, and were living close to the hospitals using iv/ip chemotherapy. Only 6% of the patients were actually treated with iv/ip therapy in the region of the hospitals offering iv/ip chemotherapy in the past eight years. Even allowing for insufficient functional status and/or patient preference, this number seems low. A lack of familiarity with ip administration procedures, perceived toxicity, or financial incentives leading to inadequate referral to ip/iv centres may be part of this gap between eligibility and actual treatment.5,10,12 In the US, a recent report of Medicare beneficiaries found that only 3.5% of women with OC received iv/ip chemotherapy.12 Moreover, if we would reflect on all eight Dutch centres that treat OC, the percentage of Dutch patients receiving iv/ip chemotherapy would be even lower.
One way to improve patient referral for iv/ip chemotherapy is developing uniform patient information leaflets and shared decision-making tools which are available in the centres that apply iv/ip chemotherapy, should be available for all patients in the Netherlands. Currently, a project addressing this issue is in progress. In addition, optimal referral with discussion in expert multidisciplinary teams (leading to survival gain), before and after primary surgery, with optimisation of patient selection and patient counselling, education of referring physicians, and overcoming logistical hurdles, including financial incentives, will be key.5,10-12,37-40 Further research after adjustment of therapy regimen and co-administered medication is also needed to decrease or palliate toxicity. This study has several limitations. First, the sample size is small. Second, toxicity was not reported with the rigor of a randomised controlled trial. For this reason, some data on morbidity and toxicity are lacking and may have led to underreported results. Third, we lack detailed information about the performance status of patients during iv/ip treatment and were unable to correlate results with this factor. Despite these limitations, the current study contributes new findings based on nationwide, multicentre data. We succeeded in collecting data on all patients who have been treated with ip chemotherapy since 2006 until 2015, from all institutes in the Netherlands that apply this treatment modality.
CONCLUSION
Toxicity, RFS, and OS of ip chemotherapy administered in daily practice in the Netherlands, for patients with advanced, at least optimally debulked OC, leads to similar results as those reported by Amstrong et al. in a randomised controlled trial.
DISCLOSURE
The authors have declared no conflicts of interest.
ACKNOWLEDGEMENTS
The authors would like to thank all participants for participation in our study. Furthermore, we thank the Department of Biostatistics, Radboud University Medical Center and the Netherlands Cancer Registry for their support.
REFERENCES