KEYWORDS
ANCA-associated vasculitis, pauci-immune glomerulonephritis, recommendations
INTRODUCTION
Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a rare systemic autoimmune disease affecting small vessels and includes three different entities: granulomatosis with polyangiitis (Wegener) (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (eGPA).1 Untreated AAV is associated with high morbidity and mortality2 and therefore early diagnosis and treatment is essential to reduce fatal outcome and prevent chronic damage. Simultaneously, the wide variety of presenting symptoms related to AAV, together with its low prevalence make timely diagnosis challenging to clinicians. Many randomised diagnostic and therapeutic studies in the past half century have transformed AAV from a fatal disease to a chronic (relapsing) disease.3 Survival rates below 20% in untreated GPA patients, before the introduction of corticosteroids and cyclophosphamide (CYC) in the 1960s,2 have now improved to one-year survival rates in 81-95% of GPA patients, with 73-83% of patients surviving after 5 years and 55-75% after 10 years.4 Improved survival coincides with an increased risk of side-effects from intensive immunosuppression in the long-term, such as infections and malignancies. Therefore, current studies aim to improve and define the optimal balance between over- and under-immunosuppression during remission-induction and maintenance therapy. AAV patients encompass a heterogeneous group that requires an individualised and often multidisciplinary approach to treatment. The clinical diagnosis, the severity of the disease, and patient characteristics are important for tailoring an optimal treatment strategy for each AAV patient.5-8 However, the rarity of the disease results in reduced routine of treating physicians which can be illustrated by a high level of clinical practice variation. The rarity of diseases, such as AAV, is also a barrier for large, high-quality studies to establish high grade evidence to support clinical practice,9,10 despite joint international efforts to conduct large randomised controlled trials.11-19 To overcome this, physicians are supported by the development of clinical practice guidelines (CPGs), which are a common way to improve health care quality and safety through standardisation.20 Indeed, CPGs are ‘systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances’.21 CPGs are known to improve clinical outcomes, promote consistency of care and reduce unwanted variation in health care as well as health care costs.22-25 Developing CPGs for a rare disease like AAV is difficult because clinical evidence is based on only a few large, controlled clinical trials supplemented by mostly uncontrolled trials with smaller sample sizes, increased heterogeneity and limited generalisability.9,24 Altogether, these limitations to the development of CPGs permit, and sometimes even encourage, practice variation within the care for a rare and complex disease like AAV. In order to improve the implementation of currently available CPGs on AAV in the Netherlands, a national initiative was launched to assemble and summarise expert opinion recommendations from a broad number of clinicians experienced in diagnosing and treating AAV patients. The present study describes the results of a national initiative in the Netherlands that considered the challenges clinicians face when caring for their patients with AAV. Based on a longstanding, national collaboration in the field of AAV that previously resulted in a Dutch guideline on the diagnostics of small-vessel vasculitis,26 we now developed consensus-based recommendations on the implementation of (inter)national guideline recommendations concerning diagnosis, terminology, and treatment (algorithms) for patients with AAV.
METHODS
ARCH foundation
In 2017, the Arthritis Research and Collaboration Hub (ARCH) foundation was initiated with the goal to improve healthcare for patients with rare systemic autoimmune diseases including AAV, by spreading expertise and by sharing medical information easily among physicians. With the support of ARCH, we initiated a national initiative to achieve consensus on diagnosing and treating AAV patients. The national initiative encompassed different methods and platforms to discuss and measure consensus guided by recommendations from current (inter)national guidelines. A national working party for AAV was organised, which included experts in multiple disciplines as well as representatives from the Dutch Vasculitis Foundation and national professional associations including internal medicine, nephrology, rheumatology, clinical immunology, pathology, dermatology, otorhinolaryngology, and ophthalmology. The working group was led by core members: three medical specialists, a nephrologist (YKOT), rheumatologist (SWT), clinical immunologist (AR); the chairman of the Dutch Vasculitis Foundation (PMJV); and one physician-scientist (ED). Core members were responsible for organisation of meetings, leading discussions, and composition of the implementation document.
Implementation document
Between February and August 2018, an implementation document was composed by the multidisciplinary working group AAV. This document describes the basic approach to the diagnosis and management of AAV based on recently published management guidelines and clinical trials over the last two decades. Sixty-five recommendations from the following guidelines were used as basis for the implementation document: The Canadian Vasculitis research network (CanVasc) recommendations for the Management of Antineutrophil Cytoplasm Antibody-associated Vasculitides; the British Society of Rheumatology (BSR) and British Health Professionals in Rheumatology (BHPR) guideline for the management of adults with ANCA-associated vasculitis; and the European League Against Rheumatism/European Renal Association—European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of ANCA-associated vasculitis.6-8 A recently developed Dutch guideline for ANCA-associated vasculitis with renal involvement was also consulted during this process because it encompassed the clinicians’ preferences within the Dutch nephrology community.6-8,27 All clinical trials and studies relevant to this implementation document were referenced in the implementation document. The document is made available as supplementary material.
Invitational consensus conference
An invitational consensus conference was organised where AAV patients, clinicians with experience on the treatment of AAV patients, paramedics, and physician-scientists in the field of AAV were invited through above-mentioned professional associations. Professional associations were responsible for the national distribution via their respective websites, scientific committees/representatives, or mailings. The Dutch Vasculitis Foundation was also invited. Additionally, members of the Dutch national working party on systemic autoimmune diseases (Systemische Autoimmuunziekten Nederland, SANL) were invited and the conference was advertised via the ARCH website. Recommendations from the implementation document were distributed in a timely manner to participants before the conference and discussed plenary. There was a focus on domains in the diagnosis and treatment of AAV where no clear consensus could be deducted from current (inter)national guidelines, or domains which were perceived as deviating from Dutch clinical practice or with a high clinical practice variation.
Online survey
An online survey was distributed nationally to all members of the two most represented professional organisations during the invitational conference: the Dutch Federation for Nephrology (NfN – 424 physicians) as part of the Dutch Society of Internal Medicine and Dutch Society for Rheumatology (NVR – 395 physicians). The online survey requested the opinion on statements covering all the domains of diagnosing and treating AAV.
Analysis To achieve consensus on a national level, the Delphi method was used as basis for consecutive meetings and surveys as described. At any stage during the procedure, statements that were discussed and presented were voted upon by physicians on a binary scale (1: Agree [A] and 2: disagree [D]). Cut-off for consensus was set at 70% (dis)agreement. Descriptive statistics was used to summarise characteristics of the participants in different platforms and the degree of consensus per statement and domain. All analyses were performed with IBM SPSS Statistics version 23.
RESULTS
A total of 98 Dutch physicians participated in a Delphi procedure to discuss and find consensus during conference or online survey. Among these physicians were 75 nephrologists, 16 rheumatologists, 5 clinical immunologists, 1 pulmonologist, and 1 pathologist. The criterium for consensus was met for 37 of 50 statements (74%). All statements with their level of agreement are documented in the implementation document (Supplementary material), including the contribution of a maximum of 10 patients. For the sake of clarity and conciseness, a summary on the statements deemed most relevant to Dutch clinical practice in the domains of diagnostics, terminology, and (concomitant) treatment (table 1) are described in this manuscript.
Implementation domain: Diagnosis of AAV
Statement 1: High-quality antigen-specific immunoassay tests are recommended for ANCA testing
The previous consensus statement recommended that positive ANCA tests (generally performed through antigenspecific immunofluorescence) should be confirmed in a second independent test.28 Implementation of this recommendation is traditionally left to the discretion of local practices and it is unclear whether the confirmation test should be performed and reported sequentially or simultaneously. Recently, a consensus statement by clinical immunologists was published on the basis of novel research recommending a high-quality antigen-specific immunoassay as the first test and confirmation by a second high-quality immunoassay (preferably by a second antigenspecific immunoassay test or an immunofluorescence test using neutrophils as substrates). Consequences of the implementation of this diagnostic strategy was extensively reviewed.29 Consensus was unanimous (A: 100%, D: 0%) that high-quality antigen-specific immunoassay tests should be used instead of immunofluorescence for the assessment of patients with clinical suspicion of AAV. This was predominantly due to the superior sensitivity and specificity of antigen-specific immunoassays over immunofluorescence tests using neutrophils as substrates.29,30
ANCA testing should only be performed when there is clinical suspicion for AAV. The following key symptoms were commonly considered as supportive of clinical suspicion for AAV: bloody crusts in the nose (93%), lung nodules (90%), (epi)scleritis/retro-periorbital inflammation (89%), arthritis/arthralgia (87%), renal insufficiency, (microscopic) haematuria and/or proteinuria (84%), fever of unknown origin (81%), skin manifestations (80%), and neuropathy (80%). When AAV is suspected, initial diagnostic evaluation should include: urinary sediment (100%), ANCA serology (98%), renal function (98%), chest X-ray (94%), inflammation markers (92%), and complete blood count (87%). There was no consensus on the added value of electrolytes (49%) and liver enzymes (48%). Histopathological evidence (30%) was not required during initial evaluation of patients, as further discussed in Statement 2.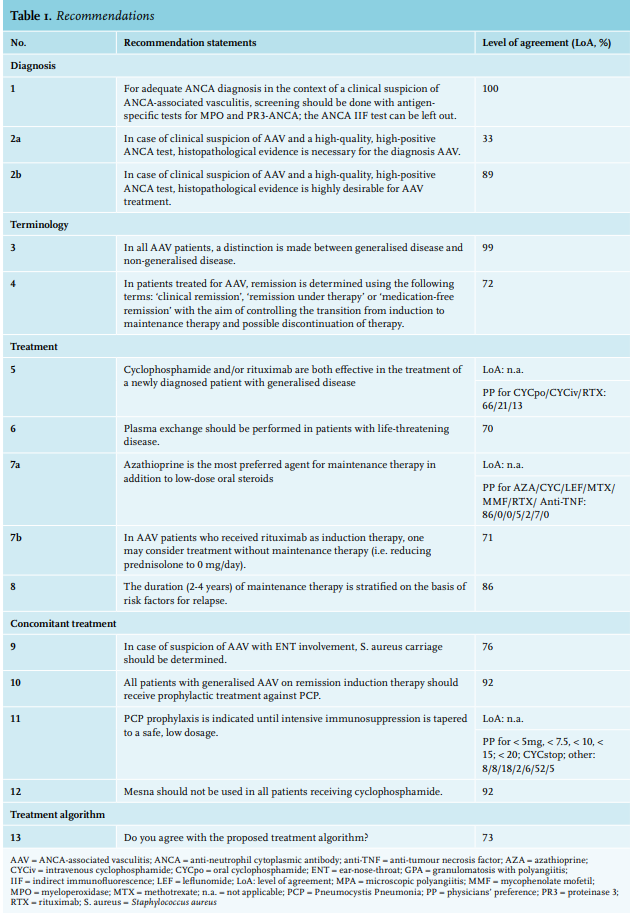
Statements 2a and b: Histopathological evidence of small-vessel vasculitis is highly desirable, but lack thereof should not interfere with the initiation of adequate treatment
There is a long-standing debate as to whether a kidney biopsy, involving a high-risk procedure, is indicated when there is already strong clinical suspicion of AAV with renal insufficiency, an active urine sediment with dysmorphic erythrocyturia, proteinuria, and a positive ANCA test. It has been shown that in such cases the chance for a kidney biopsy to confirm ANCA-associated glomerulonephritis lesions is probably well above 90%.31 A recent study summarising the outcomes of histopathological examinations of non-renal biopsies in GPA patients demonstrated typical vasculitis findings in only 39% of the biopsies, while 55% of the biopsies showed non-specific lesions.32 Consequently, the absence of specific histopathological lesions in such cases requires serious reconsideration of the clinical diagnosis of AAV.
Consensus was reached on the importance of obtaining histopathological evidence for vasculitis from an affected organ (e.g., kidney, lung, nose, skin) in particular, to support treatment choices in those cases that require initiation of intensive remission induction therapy. There was no majority found to make a distinction for myeloperoxidase (MPO) and proteinase-3 (PR3)-positive patients within this particular discussion on obtaining histopathological evidence of vasculitis. Because the recent study by Bossuyt et al. showed only small differences in sensitivity of PR3 (94%) vs. MPO (87%) and specificity of PR3 (90%) vs. MPO (83%), it would not affect the wording ‘highly desirable’ within this statement.29 In general, any diagnostic procedure should be performed when it has added value for diagnosis or consequences for treatment decisions and/or prognosis in AAV patients. Especially in AAV patients with renal involvement, a kidney biopsy will often provide answers that are important for diagnosis, treatment intensity, and prognosis of AAV disease and therefore the rationale to perform a renal biopsy stands. However, as for any invasive diagnostic test, the risks of a kidney biopsy should be considered (i.e., 3.5% bleeding of which 0.9% need transfusion and 0.6% need angiographic intervention; up to 14% AV-fistulas; ≤ 0.01% nephrectomy).33,34
Histopathological validation of the diagnosis AAV is of particular importance when adequate clinical response is unexpectedly lacking after initiation of treatment. In patients without renal symptoms, the potential clinical value of a kidney biopsy to confirm AAV remains unknown.
Implementation domain: Terminology
Statements 3 and 4: Homogenous terminology of disease severity and disease states support therapeutic decision-making
Guidelines have used different terminology to define disease severity of AAV requiring less or more intensive immunosuppressive treatment. Definitions of disease stages formulated by the EUVAS group (European Vasculitis Study Group) and the WGET research group (Wegener’s Granulomatosis Etanercept Trial Research Group) are being used frequently to classify AAV in clinical trials and guidelines.35,36 EUVAS defines four different disease stages: localised, early systemic, generalised, and severe AAV. Localised AAV is characterised by ear-nose-throat (ENT) and lung involvement with mild renal impairment (serum creatinine < 120 umol/l). In cases of other non-upper respiratory tract organ involvement on top of localised disease, it is called early systemic disease. The generalised form is defined as organ-threatening disease in organs outside the ENT and lungs with a serum creatinine of < 500 umol/l. When the serum creatinine level is > 500 umol/l, it is called severe disease. WGET makes a distinction between limited and severe disease. Limited disease is defined as sinus, skin, joints, and mild renal manifestations. Lifeor organ-threatening manifestations, such as rapidly progressive glomerulonephritis, pulmonary haemorrhage and vasculitis neuropathy is defined as severe AAV. On the basis of these disease stages, different treatment regimens are recommended (more severe stages require more intensive immunosuppressive medication).
It is clear that for implementation of guideline recommendations, consensus is needed on terminology. As such, consensus was reached on differentiating generalised disease from life-threatening and non-generalised disease (A: 99%, D: 1%). Generalised disease is defined as organ-threatening disease/involvement of organs such as kidneys, lungs, heart, and peripheral or central nervous system, whereas life-threatening disease includes rapidly progressive glomerulonephritis leading to end-stage renal disease, severe pulmonary haemorrhage, and/or dual anti-glomerular basement membrane (GBM) and ANCA positivity. Non-generalised disease is when none of the above-mentioned symptoms are present. Intensity of immunosuppression and treatment approach was coupled to this terminology.37
Also, consensus was reached on two definitions of clinical remission (‘remission on therapy’ and ‘medication-free remission’) (A: 72%, D: 28%), which also was coupled to treatment decision regarding maintenance therapy. ‘Remission on therapy’ is the state of clinical remission ≥ 6 months at a prednisolone dose ≤ 10 mg/day and medication-free remission is clinical remission without any immunosuppressive medication. From these disease states, it also becomes obvious that ‘clinical response’ to treatment is a clinical state where an improvement of disease activity is observed but ‘clinical remission’ is not yet achieved.
Implementation domain: Treatment of AAV
Statement 5: Cyclophosphamide and/or rituximab are both effective in the treatment of a newly diagnosed patient with generalised disease
Several guidelines recommend glucocorticoids in combination with cyclophosphamide (CYC) or rituximab (RTX) as remission induction therapy for generalised and life-threatening disease.6-8 Oral CYC was introduced in the 1960s as a treatment for AAV and significantly changed the disease course. Unfortunately, CYC treatment is accompanied by serious side effects and (long-term) toxicities in association to its life-long, cumulative dose. Significant progression has been made by studies investigating lower dosing of CYC without loss of efficacy: the CYCLOPS study showed that pulsed intravenous CYC was non-inferior to daily oral CYC to achieve remission, long-term survival, preservation of renal function, and prevention of end-stage renal failure. Equivalence on these hard endpoints were observed despite an increased relapse rate in patients treated with intravenous CYC. At the same time, intravenous CYC was associated with fewer side effects.11 Of note, several studies11,38-40 have shown that the risk for relapse is inversely associated with the cumulative CYC dose received during the induction phase. In 2010, the RAVE study compared RTX to oral CYC demonstrating that RTX was non-inferior to CYC in achieving remission in newly diagnosed AAV patients with generalised disease; of note, RTX was superior to CYC in relapsing AAV patients.18
Overall, CPGs have remained careful in their recommendations on a preferable agent for remission induction therapy and recommend either CYC or RTX in AAV patients with generalised disease, and azathioprine (AZA), methotrexate (MTX), or mycophenolate mofetil (MMF) in AAV patients with non-generalised disease unless contraindicated (i.e., impaired renal function). In the present initiative, we surveyed physicians’ preference and found that in the Netherlands, 66% of physicians prescribe oral CYC, 21% intravenous CYC, and 13% RTX as induction treatment for AAV patients with generalised disease. Thus, we are aligned with the CPGs’ recommendations, and have stated in the implementation document that CYC and RTX are equivalent therapy choices as induction treatment. Clinicians should consider the (dis)advantages of CYC and RTX for each individual patient who requires remission induction therapy.
Statement 6: Plasma exchange therapy should be performed in patients with life-threatening disease
In addition to immunosuppressive agents, the EULAR recommendations and BSR/BHPR guideline suggest to add plasma exchange (PLEX) therapy in patients with a serum creatinine level > 500 umol/l and/or pulmonary haemorrhage.6,8 The CanVasc recommends PLEX only in patients who remain refractory with immunosuppressive therapy because of controversial long-term outcomes on renal survival and mortality.7 Preliminary data of the PEXIVAS study, which was presented at the EULAR/ ERA-EDTA congress, has shown that additional PLEX had no favourable long-term outcomes in comparison to regular immunosuppressive therapy, but these were not published at the time of this inventory. Until the results of this trial are published and/or confirmed, we recommend to perform PLEX in patients with life-threatening disease. Consensus was achieved on adding PLEX if the patient suffers from rapidly progressive glomerulonephritis and/ or alveolar haemorrhage (A: 70%, D: 30%).
Statement 7a: Azathioprine is the most preferred agent for maintenance therapy.
Statement 7b: After an RTX-based remission induction therapy, the physician may consider treatment without maintenance therapy (i.e., reducing prednisolone to 0 mg/day).
When remission is achieved after remission induction therapy, maintenance therapy is required to prevent relapses. Previous studies have shown that relapses occur in 30-50% of patients after reducing or discontinuing therapy.41-44 In the last decade, pioneering clinical trials studying maintenance therapy drugs and duration have been conducted.12,16,45 The CYCAZAREM study investigated the replacement of CYC by AZA after achieving remission in comparison to prolonged CYC treatment as maintenance therapy. No difference was observed in relapse rates between these groups, concluding that AZA is a safe alternative for maintenance therapy.14 Hereafter, AZA has been considered the most effective treatment for maintaining clinical remission compared to MTX (WEGENT), MMF (IMPROVE), leflunomide (LEM), belimumab (BREVAS), or anti-TNF (WGET).13,17,36,46,47 Most recently, the MAINRITSAN studies12,45,48 demonstrated the superiority of RTX maintenance treatment over AZA, in which case fixed re-treatment every six months or tailored RTX infusions on the basis of CD19+ cells and ANCA levels had comparable efficacy on maintaining clinical remission. However, these data were not publicly available at the time of the survey.
In CPGs, after remission induction therapy, the CanVasc group and the BSR/BHPR guideline recommend to use either AZA, MTX, or RTX as maintenance therapy and if not tolerated, MMF or leflunomide.6,7 According to the EULAR recommendations, the aforementioned agents AZA, RTX, MTX, and MMF can be used as maintenance therapy.8 Besides the RAVE study, there is a lack of data on maintenance treatment after remission induction therapy with RTX. This study confirmed that no maintenance treatment after RTX was equivalent to AZA maintenance after CYC.18,49 Consequently, recommendations on optimal maintenance therapy remained unclear.
In the present study, we surveyed physicians’ preference and found that AZA is the most preferred maintenance therapy in addition to low-dose oral steroids (86%) in the Netherlands. RTX maintenance was only given by 7% of physicians. Upon RTX given as remission induction therapy, 71% of physicians would consider continuing without any maintenance therapy (similar to the RAVE study).18,49 It needs to be mentioned that at the time of the survey, the long-term results of the MAINRITSAN-1 and MAINRITSAN-2 studies were not publicly available yet and might have influenced the formulation of this statement which was built upon physicians’ preferences.
Statement 8: The duration of maintenance therapy should be based on risk factors for future relapse
There is no clear consensus on the optimal duration of maintenance therapy. In 2017, the EUVAS working group analysed in 380 new AAV patients whether duration of AZA maintenance influenced relapse rates at five years. Interestingly, discontinuing AZA maintenance ≤ 12 months results in significant more relapses, whereas this phenomenon disappeared in patients with AZA maintenance for 18 months or more.50 Guidelines also recommend to continue maintenance therapy for 18-24 months after diagnosis.6-8 A Dutch study demonstrated no additional value of extending maintenance therapy (4 years vs. 1 year) in AAV patients, however unfortunately, the study was prematurely stopped due to slow patient recruitment.51 More recently, a large randomised, controlled trial (REMAIN study) demonstrated a significant reduction of relapse risk when maintenance therapy with low-dose steroids and AZA was maintained for four years compared to two years.16 Despite these conflicting results and well-established risk factors for relapse derived from several large RCTs, as detailed in the implementation document, table 6 (Supplementary material),44,52-54 consensus was reached on the recommendation that risk factors for relapse should be taken into account at the time of discontinuing maintenance therapy after at least two years (A: 86%, D: 14%).
Implementation domain: Concomitant treatment
Statement 9: Nasal carriage of Staphylococcus aureus should be determined in AAV patients with ear-nose-throat involvement
Previous studies have shown that chronic carriage of nasal Staphylococcus aureus (≥ 75% of the cultures were positive) in patients with nasal disease is associated with higher relapse rates and treatment with trimethoprim/ sulfamethoxazole 960 mg given twice daily for two years is able to reduce relapse rates.55,56 In the AAV guidelines, no statement or recommendation is made on testing nasal carriage of S. aureus, but only on treating this condition. Although in the general population approximately one-third has intermittent and one-third has chronic carriage of S. aureus, 60-70% of GPA patients are carriers of S. aureus. 57 We reached consensus on the need for determining nasal carriage of S. aureus in patients with (a clinical suspicion of) AAV and ENT involvement (A: 76%, D: 24%). In carriers, treatment with oral trimethoprim/ sulfamethoxazole can be considered.
Statement 10: All AAV patients on remission induction therapy should be treated with pneumocystis pneumonia (PCP) prophylaxis.
Statement 11: PCP is indicated until intensive immunosuppression is tapered to a safe, low dosage.
Patients suffering from autoimmune diseases and receiving immunosuppressive treatment are at increased risk of developing pneumocystis pneumonia (PCP).58-60 Several papers describe an important role for corticosteroids in the development of PCP, whether or not in combination with other cytotoxic agents.58,61-63 The use of PCP prophylaxis is advised in patients with corticosteroids ≥ 20 mg/day for at least one month and is especially recommended in the presence of additional T-cell defects or cytotoxic agents such as CYC.64
Guidelines have stated that PCP prophylaxis should be given to patients on remission induction therapy, if not contraindicated. The EULAR/ERA-EDTA recommends prophylaxis against PCP only in patients receiving CYC; there is no recommendation for patients receiving RTX.8 The BSR/BHPR guideline briefly mentions that PCP prophylaxis should be considered for AAV patients on immunosuppressive therapy6 and the CanVasc group recommends prophylaxis against PCP in patients receiving either CYC or RTX. In patients receiving CYC, prophylaxis should be continued for at least three months after cessation of CYC, because of the occurrence of PCP infections in several case reports after withdrawal of remission induction therapy.61 There is no statement on the optimal duration of PCP prophylaxis after remission induction treatment with RTX.7 Based on two different studies, PCP prophylaxis seems to be indicated in RTX-treated AAV patients because of severe infections.65,66
We surveyed physicians’ preference regarding PCP prophylaxis and found that in the Netherlands, 92% of clinicians will prescribe PCP prophylaxis during remission induction therapy; 52% would stop prophylactic treatment for PCP simultaneously with tapering or termination of CYC; 18% would discontinue PCP prophylaxis at the time of reaching a prednisolone dose of ≤ 10 mg/day, 6% when reaching ≤ 20 mg/day, 2% at reaching ≤ 15mg/day, 8% when reaching ≤ 7.5 mg/day, and 8% when reaching ≤ 5 mg/day.
Statement 12: Mesna should not be used in all patients receiving cyclophosphamide
High-dose intravenous CYC or long-term oral CYC (> 3 months) is associated with haemorrhagic cystitis and bladder cancer due to the interaction between the acrolein metabolite of CYC and the bladder wall.67,68 Mesna (2-mercaptoethane sulfonate) is able to inactivate acrolein and prevent these side effects.69 These results are based on CYC use in patients with cancer receiving higher doses of CYC in comparison to patients with rheumatic diseases. Because of the lack of evidence in patients with rheumatic diseases, there are no strong recommendations for mesna use in guidelines for AAV. A national position statement by Dutch rheumatologists has advised that mesna should only be considered in patients with long-term CYC use and at high risk for bladder toxicity (e.g., disturbed bladder emptying, urinary retention, or recurrent cystitis).6-8,67,70 Structural examination of the urine sediment helps to detect bladder toxicity.27,67,70 Indeed, consensus was reached that mesna should not be prescribed in all CYC-treated AAV patients (A: 91%, D: 9%).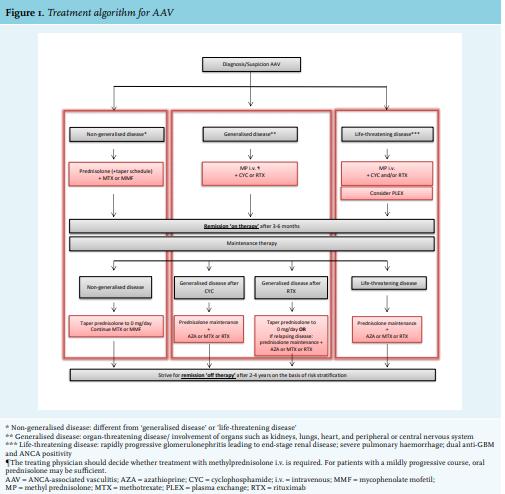
Statement 13: Treatment algorithm – figure 1
Based on several statements discussed above and detailed in the implementation document (Supplementary material) consensus was reached on a treatment algorithm (A: 73%, D: 27%) for AAV patients (figure 1).
Categorisation of AAV patients upon clinical presentation
Delay in diagnosing or initiating adequate therapy in patients with severe AAV may have harmful consequences. Therefore, the treatment algorithm first necessitates at an early stage, the categorisation of patients by consensus-based definitions, i.e., ‘life-threatening disease’, ‘generalised disease’ or ‘non-generalised disease’.
Associated with disease categories is the choice of remission induction therapy
If there is a life-threatening disease, consensus was that PLEX therapy should be considered in addition to treatment with intravenous methylprednisolone pulse therapy and cyclophosphamide whether or not combined with RTX.15,71 Of note, agreement on the use of methylprednisolone pulses was found on the background that PLEX therapy is not readily available in all Dutch hospitals. As mentioned before, publication of the results from the PEXIVAS study will undoubtedly improve the selection criteria for which AAV patients PLEX therapy can be indicated. In patients with generalised disease, either intravenous methylprednisolone or oral prednisolone can be chosen in combination with CYC or RTX during the remission induction phase. In specific cases (e.g., patients with a mildly progressive course), oral prednisolone combined with an immunosuppressive agent may be sufficient. Patients with non-generalised disease should start with high doses of prednisolone combined with an immunosuppressive agent such as MTX or MMF during the remission induction phase.
Categorisation of AAV patients when responding to treatment
Usually, patients achieve clinical remission, defined as absence of disease activity (BVAS score of 0), between 3-6 months after initiation of remission induction therapy. At this state, patients are ‘in remission on therapy’. At that time, maintenance therapy should be initiated to prevent disease relapses and is interdependent to the chosen remission-induction treatment. As such, patients with life-threatening disease should continue with maintenance therapy in the form of low-dose oral prednisolone combined with AZA, RTX, or MTX. The choice for a specific agent depends on the tolerance of a patient and the preference of the treating physician. Patients with generalised disease treated with CYC as remissioninduction will continue prednisolone combined with AZA, RTX, or MTX. Patients with generalised disease treated with RTX as remission-induction will taper prednisolone to 0 mg/day and stop maintenance therapy, unless the patient suffers from relapsing disease. In that case, maintenance therapy should be continued with low-dose oral prednisolone combined with AZA, RTX, or MTX. Patients with non-generalised disease should continue treatment with low-dose oral prednisolone in combination with MTX or MMF.
The ultimate aim is to achieve ‘medication-free remission’. This goal can be realised within two to four years after starting AAV treatment, where the duration of maintenance treatment should be guided by the individual patient’s risk classification for a relapse.
DISCUSSION
AAV is a complex, systemic autoimmune disease with a low disease prevalence and therefore intrinsically difficult to diagnose and treat, which is eventually reflected in clinical practice variation. Due to the rarity of the disease, it is challenging to obtain high-quality clinical evidence to underpin firm and coherent recommendations in guidelines for clinicians allowing, intended or not, for considerable differences in clinical AAV management between physicians. In this setting, the present study described the development of a national, multidisciplinary, consensus-based implementation document. By means of a nation-wide consensus the implementation of guideline recommendations can be improved because clear and practical guidance is given for treating physicians, including for those issues that cannot be addressed by guidelines due to lack of data or adequate, comparative studies. Moreover, a consensus-based implementation document can address practice variation and thereby improve physicians collective experience with a uniform management of patients with a rare and severe disease like AAV. Ultimately, harmonisation of the management will improve standardised evaluation of care for AAV patients which is a prerequisite for improving care in the future.
We described a Dutch national implementation document on the basis of previously published guidelines and consensus (of ≥ 70%) among nation-wide healthcare professionals experienced in treating AAV patients. This implementation document is complementary to current evidence-based guidelines because it enabled us to provide recommendations on practical issues where evidence is not readily available. Exemplary are the recommendations on terminology annotating disease subsets, disease states, and disease extent in direct relation to treatment choices; the methods of ANCA testing and confirmation; the minimal requirements for the organisation of care around AAV patients; and the use of PLEX in AAV patients with life-threatening disease. For the latter, it is important to note that the level of agreement on the indications for PLEX can be influenced in the near future by the publication of the PEXIVAS study results and the results of a meta-analysis of all studies on PLEX in AAV collectively. As such, this implementation document with high rates of consensus facilitates the harmonisation of local treatment protocols for AAV and reduce practice variation with the intent to improve care for AAV patients nationwide.
Not unexpectedly, we encountered several noteworthy findings during this study. First, based on the characteristics of responders on our nation-wide invitation through professional associations, the majority of the participants were nephrologists and to a lesser extent, rheumatologists. It is therefore important to note that due to a higher representation of nephrologists, one can argue that this document is based on a consensus between nephrologists rather than the broad concept of any treating physician involved in the treatment of AAV. However, although speculative at this time, participation to our study indicates that AAV patients in the Netherlands are in general, treated by nephrologists and/or rheumatologists. To confirm this observation, a more in-depth study at the individual patient-level is needed. Second, a remarkable observation was the high frequency (66%) of participants employing oral CYC as the preferable first-line therapy, while several trials and guidelines, including Dutch guidelines, recommend intravenous CYC or RTX because of reduced toxicity.6-8,11,18 One can only speculate on the rationale of individual physicians however, possible explanations can be found in the suggestion of reduced relapse rates in the pivotal CYCLOPS study, the convenience of oral CYC administration without the need of hospital admissions for intravenous treatments (i.e., CYC iv or RTX), and its lower costs. Third, the preference for AZA as maintenance therapy in the majority of the physicians is noteworthy. At the time of this study, the long-term results of the MAINRITSAN-1 and MAINRITSAN-2 studies were not widely available.
Altogether, we present an implementation document for the diagnosis and treatment of AAV that is complementary to a previously published Dutch multidisciplinary guideline on the diagnosis of small-vessel vasculitis26 and the Dutch guideline for treatment of renal vasculitis.27 The described implementation strategy can be exemplary for other countries to translate international guideline recommendations into common clinical practice. In addition, during our study, several clinically-relevant issues were identified for the AAV research agenda, such as the value of risk-stratification in deciding whether to stop treatment and the position of rituximab as maintenance treatment tailored by immunological parameters (i.e., ANCA and B-cell levels). Future studies will be directed at evaluating whether this consensus-based, implementation strategy reduces clinical practice variation in the Netherlands and improves healthcare for AAV patients. To do so, a nation-wide study has been started to evaluate the care provided to AAV patients in the past 10 years. This study will provide important insights into current practice variation in the Netherlands with regard to diagnosis (including in-hospital time-to-diagnosis and patient characteristics), treatment regimens (including immunosuppressants used for induction and maintenance therapy and duration of treatment), and disease outcomes (including mortality, infections, and malignancies); at the same time, indicators for the quality of care can be defined. Also, in order to contain practice variation, strategies will be developed to improve access to expert advice and/ or consultation. Ultimately, these efforts will lead to the improvement of care and disease amelioration for AAV patients.
ACKNOWLEDGMENTS
The work of E. Dirikgil., Y.K.O. Teng, S.W. Tas, P.M.J. Verhoeven, A. Rutgers, J.M. van Laar, and H.J. Bernelot-Moens is financially supported by Arthritis Research and Collaboration Hub (ARCH). Y.K.O. Teng is funded by the Dutch Kidney Foundation (KJPB12.028), Clinical Fellowship from the Netherlands Organization for Scientific Research (90713460).
We thank all patients and professional healthcare providers who participated in the consensus meeting and online survey for their effort and time. The final implementation document is published in Dutch at the website of ARCH: https://www.arch.nl/wp-content/ uploads/2018/10/ConsensusdocAAV-1.pdf
SUPPLEMENTARY MATERIAL
For the implementation document in Dutch, please request via email: y.k.o.teng@lumc.nl or info@arch.nl
REFERENCES