KEYWORDS
Antibiotics, bloodstream infections, blood cultures, laboratory staffing, microbiology, delayed treatment, after office hours
INTRODUCTION
Timely adequate treatment of bloodstream infections is important to reduce mortality and morbidity,1-5 so in most suspected cases patients immediately receive empirical broad-spectrum antibiotics. Nevertheless, because these empirical antibiotic regimens can still be inadequate, delayed reporting of blood culture results is associated with increased infection-related mortality.6,7 Delayed culture reporting may also impede important antimicrobial stewardship goals such as streamlining and de-escalating of antimicrobial therapy.8,9 It is therefore important to identify unnecessary delays in the process, from blood culture collection to administration of a culture-based antimicrobial agent.
Previous studies have shown that patient care delivered during hospital office hours is associated with a shorter length of stay and lower mortality in comparison to care delivered after hospital office hours.10-13 In the United Kingdom, this has even led to a call for equal standards of performing care, seven days a week.14 With regard to blood culture processing, a study by Morton et al. demonstrated that culture yield can be lower during the weekend,15 possibly due to lower staff presence or delayed incubation or processing.16 Immediately incubating collected blood samples has been shown to reduce these delays.17 However, most microbiological laboratories do not process blood cultures after office hours, leaving room for potential delays. Furthermore, there is an increasing number of onsite hospital microbiological laboratories being moved offsite to save costs and to increase performance.18,19 As culture specimen transport is generally only performed during office hours, cultures identified as positive after the last transport of the day are not processed until the next morning. Having the laboratory and clinical ward at different sites has been shown to increase time between culture collection and start of incubation.16,20 Unfortunately, it is unknown whether the time to administration of an adequate antibiotic regimen is influenced by what time of day a culture is flagged as positive. We performed a retrospective study to determine the duration of each step of the process, from culture positivity to antimicrobial administration, in a hospital with an offsite microbiological laboratory. We compared the duration of each step during and outside of laboratory office hours.
MATERIALS AND METHODS
Setting: the hospital
The retrospective study was performed in a 550-bed general teaching hospital in Amsterdam, the Netherlands. It has no onsite microbiological laboratory, except for a small facility where blood culture bottles can be immediately incubated, using the BacT/ALERT incubation system (BioMérieux, Marcyl’Etoile, France). Three times a day, clinical samples including blood culture bottles that were flagged positive were transported to the offsite microbiological laboratory by transport van, with a travel time of 15-25 minutes, depending on traffic. Van departure times were 9:30 hrs, 12:00 hrs, and 16:00 hrs on weekdays. Departure time during the weekend was at 10:00 hrs; for cases with positive blood cultures, an additional transport occurred in the afternoon, and cultures were then always processed at the offsite laboratory that same day. There were no transports at other times. At least one of the two regular microbiologists were present in the hospital for consultation and communication of results during office hours (08:00-17.30) on weekdays but not during the weekend. Outside of these hours, microbiological consultation was performed by telephone by one of nine microbiologists who were affiliated with the hospital and the offsite laboratory. When present on weekdays, the microbiologist telephoned results of all positive blood cultures to the treating physician. During the weekend, only relevant positive cultures (as determined by the microbiologist) were reported to the physician. Microbiological results and therapeutic advice were also communicated to clinicians via the electronic health record system Epic (Epic Systems Corporation, USA). Microbiologists based their advice on the hospital’s local antibiotic guidelines.
Setting: the offsite laboratory
Gram stains were performed on every positive blood culture. Determination of blood culture pathogen and susceptibility testing were performed using MALDI-TOF (VITEK®MS; bioMérieux, Marcyl’Etoile, France) and disk diffusion testing was conducted according to EUCAST methodology. Laboratory opening hours were from 08:00-19.30 on weekdays and varied depending on work demands during the weekend. Gram stains and pathogen determination were not performed outside of these hours. At least one microbiologist was present at this site during these hours. Both the laboratory and the hospital used the GLIMS Microbiology Laboratory System (CliniSys Group, UK) to document all logistics steps and therapeutic recommendations. Microbiologists were immediately notified of any culture positivity via this system. Data collection We performed retrospective case reviews of hospital inpatients with positive blood cultures during two pre-selected non-consecutive weeks per month between 1 December 2011 and 31 October 2012. There was one culture with multiple pathogens; it was treated as a single culture. Subsequently drawn cultures were only included as a new case if separated by eight or more days. The microbiologist on duty excluded cultures with pathogens determined as contaminants after complete pathogen determination and in consultation with the treating physician. We retrieved all information on blood cultures, starting time of each logistics step, and antimicrobial advice from the GLIMS laboratory system. Time of culture collection could not be retrieved from this system. We lacked data to separate culture transportation from the Gram staining process so this was analysed as a single step. For each case, we assembled information on the empirical antimicrobial regimen and all changes in this regimen until 48 hours after the final pathogen determination report became available. Time of prescribing and nurse-reported time of administration were retrieved from the electronic pharmacy system Pharma (‘Apotheek Informatie Systeem Pharma’, VCD Healthcare, the Netherlands). The responsible medical ethical board approved the study. Office hours variables We created a dichotomous variable called ‘regular office hours’ if a culture was flagged positive by the incubator between the hours of 08:00-17:00 in order to differentiate it from blood culture positivity that occurred between 17:00-08:00. Because the variable depended on the moment of culture positivity in the hospital and not on time of arrival at the offsite laboratory, we used the 17:00 time point rather than the actual laboratory closing time of 19.30 to demarcate the end of regular office hours. To further analyse the effect of laboratory closing times in our data, we constructed a second variable called ‘optimal office hours’ that divided the 24-hour day into most optimal (between 02:00-14:00) and least optimal (14:00-02:00) periods with regard to timely culture processing.
Primary and secondary outcomes
Primary outcome for the study was the duration of each culture-processing step between incubation completion and administration of the first dose of the adjusted antimicrobial regimen. We assessed the influence of time of day of culture positivity on culture transport, Gram stain duration, and all subsequent culture processing steps using the two office hours variables introduced above. To check whether severity of the infection affected culture-processing time, we also focused specifically on the processing of patients with a Staphylococcus aureus bloodstream infection admitted to the intensive care unit (ICU).21
Additionally, an infectious disease specialist from a neighbouring hospital determined if each administered antimicrobial regimen provided adequate coverage of the microorganisms in the blood culture. Adequate coverage after Gram staining was defined as therapy with high expectation of clinical activity against the pathogen. Adequate coverage after full determination of the pathogen was defined as therapy for which the pathogen was susceptible in vitro. Naturally, treatments with antimicrobial drugs with insufficient pharmacokinetic characteristics were always determined inadequate, e.g. nitrofurantoin for Escherichia coli bacteraemia. Our definition of adequate therapy is independent of certain circumstances such as guideline adherence. For example, treating amoxicillin-susceptible Escherichia coli with ceftriaxone constitutes adequate coverage, despite the fact that the lack of streamlining may be seen as inappropriate from the viewpoint of antimicrobial stewardship.22
Decisions by this specific infectious disease specialist on the related concept of appropriateness of antimicrobial therapy have been shown valid and reliable when compared to colleagues.23 Finally, we also report data on treatment advice adherence.
Statistical analysis
Linear regression was used to compare the duration of culture processing steps between office hours. All time variables were logistically transformed prior to the analysis. Additionally, a variable denoting antimicrobial coverage of the cultured microorganism(s) was added to each crude model to assess potential confounding. Confounding was considered relevant if the regression coefficient from the univariable analysis differed from the coefficient in the multivariable model (containing the potential confounder) by more than 10%. We compared antimicrobial coverage percentages of the cultured microorganism(s) between the empirical phase, after Gram stain completion, and after final determination/susceptibility using logistic generalised estimating equations to adjust for clustering within patient cases. All analyses were performed using Stata 13 (StataCorp, USA). P < 0.05 was considered significant for all analyses.
RESULTS
Patients and cultures
We included positive blood cultures drawn from 136 patients. Culture results from 37 patients were determined to be a result of contamination and were excluded. Five patients were excluded because they were discharged or died before complete microorganism determination. See table 1 for baseline characteristics.
Impact of time of day of incubation completion
Median durations of each post-incubation cultureprocessing step during or outside of office hours are shown in figure 1. The difference in processing times between culture positivity during and outside of office hours was largest for the transport and Gram stain step, which also resulted in significant differences when all post-incubation steps were added together. Figure 2 demonstrates how duration of transport and Gram stain step varied for time of day of culture positivity. Cultures positive for Staphylococcus aureus were highlighted to illustrate that processing times for cultures with this specific pathogen, which indicate a serious infection with high mortality,21 were similar to those of cultures with other microorganisms. The same applied to patients admitted to the ICU. Based on the pattern of figure 2, we constructed an optimal office hours variable denoting 02:00-14:00 as the optimal period for speedy culture processing, results of which are also shown in figure 1. Adding a variable denoting adequacy of empirical treatment to the model did not change the above findings substantially. 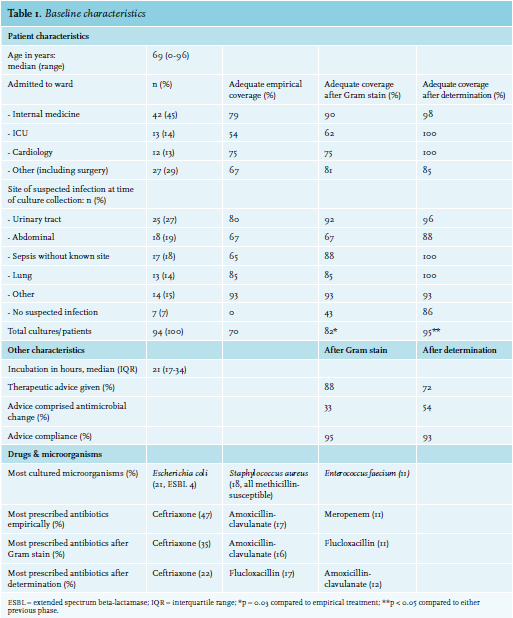
DISCUSSION
Our findings suggest that blood culture-processing time is influenced by the time of day a culture is flagged positive, in a medium-sized teaching hospital with an offsite microbiological laboratory. We showed that median time from incubation completion to Gram stain completion increased from four to 12 hours or even 16 hours, depending on the definition of office hours, irrespective of the adequacy of the empirical antimicrobial regimen. This translated to a similar increase in the cumulative time from culture positivity to administration of the adjusted antibiotic regimen. Previous studies showed that the offsite location of the laboratory is associated with increased time to start of culture incubation,16,20 but the influence of offsite location and time of day of culture positivity on the whole culture process from culture positivity to antibiotic administration has not been reported. Interestingly, our data demonstrated that the delay already showed for cultures completing incubation as early as 14:00, long before the end of the working day. In the context of literature supporting early adequate treatment of bloodstream infections to reduce mortality,1-7 this delay potentially undermines optimal clinical outcomes. 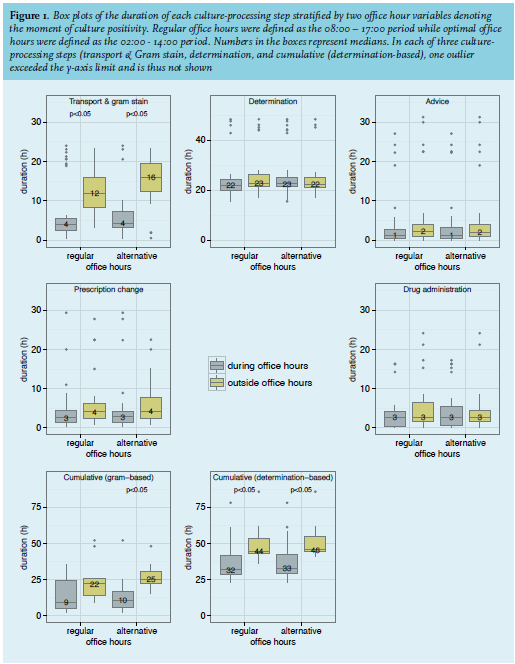
It could be argued that microbiologists might speed up culture processing if they knew that a certain patient was suspected of having a serious infection (e.g. sepsis, endocarditis). To check whether our results also applied to patients with severe infections like those admitted to the ICU or with Staphylococcus aureus bloodstream infections, we presented culture processing for these patients separately. We assumed that ICU patient culture transport and processing may have been fast-tracked. Similarly, although clinicians and microbiologists would not yet have known the responsible pathogen for the Staphylococcus aureus patients at this stage, we hypothesised that these patients may have presented with more severe or typical symptoms leading to quicker processing as well.21 However as figure 2 shows, cultures for these two groups of patients followed the same delay pattern, suggesting that this was not the case.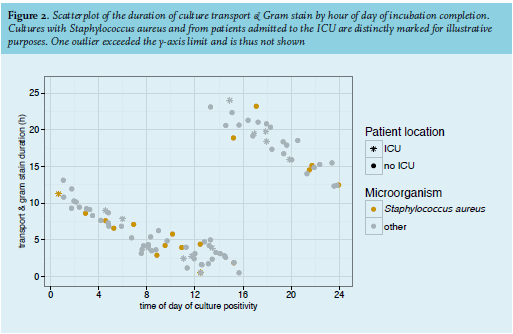
An obvious solution would be to extend transportation and laboratory activity into the evening and night, or to use a transport and stain on-demand solution. We expect that hospitals with similar characteristics to the hospital in our study would process a monthly average of 6.3 positive, new, non-contaminated blood cultures that would complete incubation between 14:00-02:00. Of these cultures, 1.9 (30%) would belong to patients who would thus not receive adequate antimicrobial coverage for the cultured microorganism. Complete culture determination in our study decreased this non-coverage to 9% so the number of patients who would potentially benefit would be 1.3, every month. Assuming that this solution would completely solve the problem of the after-hours delay, it would allow a monthly average of 1.3 patients to receive adequate antimicrobial coverage 13 hours (median value) earlier than in the current situation. In other words, although the delay is substantial, it occurs relatively infrequently and also depends on hospital size and local epidemiology.
Another potential solution can be deduced from our finding that cultures completing incubation as early as 14:00 could be deferred to the next day. This suggests that increased efforts and coordination to ensure that cultures flagged positive between 14:00 and 16:00 are included in the final transport to the laboratory where a Gram stain can be performed before closing time, may prevent unnecessary consequences.
Our results suggest there was no influence of time of day of incubation completion on the speed of culture processing after Gram staining. This is not unexpected because delays in the transport and Gram stain step meant that this step was often completed during office hours, which allowed the subsequent steps to take place during office hours as well. It must be noted that timing of treatment advice from the microbiologist is not the only determinant of the duration of prescription change and drug administration. Other factors may have played a role, such as physician-specific advice adherence rate, or sufficient or insufficient appreciation of the urgency of timely adequate treatment.
Our study has limitations. It contains a relatively small number of cultures, so a comparison of clinical patient outcomes was not feasible. Due to time constraints, we could not collect every culture available in the inclusion period, so selection bias cannot be ruled out. However, the included cultures were from all parts of the calendar year to prevent influence of specific seasons. Moreover, the specific inclusion periods were chosen before data collection took place to prevent outcome bias. The single-centre design and availability of data made it impossible to perform an isolated estimation of the effect of the offsite location of the laboratory. Still, our findings suggest that work completed during or outside office hours results in an unequal standard of care for patients with bacteraemia. This inequality is infrequent, can be substantial, and may be preventable. As outcomes and cost-effectiveness considerations are subject to local circumstances and epidemiology, we advise hospitals with similar offsite laboratories to investigate the extent of the problem in their centre in order to be able to act accordingly.
ACKNOWLEDGMENTS
We wish to thank Dr. Rogier R. Jansen for his helpful comments on the manuscript.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
R E F E R E N C E S