KEYWORDS
Ganciclovir, encephalopathy, side effect, ataxia
INTRODUCTION
Ganciclovir is often prescribed for both prophylactic and therapeutic purposes. The use of ganciclovir for a primary cytomegalovirus (CMV) infection is debatable; moreover, ganciclovir can also be associated with severe side effects. We present a case history of a patient with a rare side effect of ganciclovir.
CASE REPORT
We describe the case of a 60-year-old woman with Crohn’s disease, which is in remission with azathioprine 200 mg once a day; she is not on any other medication. She was admitted to another hospital because of a daily spiking fever up to 40 °C and severe fatigue which had developed over the last few weeks. A CMV infection was diagnosed with haemolytic anaemia (haemoglobin 5.7 mmol/l; haptoglobin 0.08 g/l) with cold agglutinins, thrombocytopenia (119 x 109/l) and leucopenia (2.6 x 109/l) and lymphopenia (0.4 x 109/l). Because of the symptomatic CMV infection in an immunocompromised patient, she was treated with intravenous ganciclovir. The azathioprine was discontinued.
Ganciclovir was started at 5 mg twice a day whereupon she was afebrile within a few days. A few days after ganciclovir was started, our patient developed back pain and an unsteady gait which progressed and after a few days she was unable to walk independently. She also developed bradyphrenia with anxiety and a disorder in word retrieval and memorisation. Our patient had never experienced these symptoms before. MRI of her head showed no abnormalities. Her creatinine level remained stable during her hospitalisation (52 µmol/l). Because of the unexplained deterioration, the patient was transferred to our hospital. Encephalitis was ruled out after clinical evaluation by the neurologist and normal cerebral spinal fluid. The EEG showed slow activity which is indicative of encephalopathy. We diagnosed a ganciclovir-induced ataxia and encephalopathy whereupon we discontinued the ganciclovir. Her neurological symptoms disappeared within a few weeks. This confirmed our diagnosis of ganciclovir-induced ataxia and encephalopathy as an explanation for her symptoms.
DISCUSSION
Based on literature it is unclear if a primo CMV infection in immunocompromised patients should be treated with antiviral agents.1 Literature suggests discontinuing or reducing immunosuppressive agents without administering antiviral drugs in a therapeutic dosage.2 However, if you do choose to start treatment with antiviral drugs the effectiveness of oral compared with intravenous treatment remains a subject of discussion.3 As described above, our patient was treated with ganciclovir intravenously because of the severe symptoms. It is recommended to start with 5 mg/kg twice a day which is reduced to once daily after seven days.
Ganciclovir is an antiviral agent that inhibits DNA polymerase and prevents replication of the virus. More than 90% of ganciclovir is eliminated through glomerular filtration and crosses the blood-brain barrier.4-6
Known side effects of ganciclovir are bone marrow depression, gastrointestinal complaints and less frequently psychiatric symptoms consisting of depression, fear and confusion. These last symptoms were observed in our patient; however, this did not explain all of her problems. Ataxia and encephalopathy due to ganciclovir is not officially registered as a side effect. At the Dutch registration for side effects (Lareb), 20 cases of encephalopathy and 12 cases of ataxia were known to have been reported internationally.4,7
Five unique cases are described in literature of ganciclovirinduced ataxia and encephalopathy.5,6 These cases describe the occurrence of neurological symptoms in patients receiving ganciclovir. Neurological symptoms consisted of an unsteady gait, dysarthria, disturbed consciousness or visual hallucinations. In four of these cases a high ganciclovir concentration in the blood was found. Only three out of five cases mentioned decreased kidney function. In one case ganciclovir toxicity was treated with haemodialysis after which the blood concentration of ganciclovir decreased.
In our patient, it is striking that the nature and course of the symptoms appear to be identical. The mean time to onset of symptoms is approximately one week. In all published cases, as well as our case, the ataxia and encephalopathy appears to be reversible. Renal impairment might cause an increased risk for developing ataxia and encephalopathy since the drug is predominantly excreted through the urine.8
However, a therapeutic ganciclovir level does not exclude the possibility of developing side effects, even with a normal kidney function (Naranjo score 7/13, probable adverse drug event; table 1).9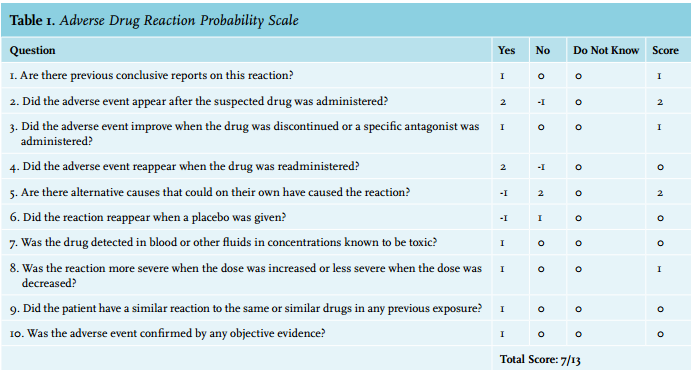
CONCLUSION
Treatment of a primary CMV infection with ganciclovir in immunocompromised patients is debatable. If a patient treated with ganciclovir develops neurological symptoms one should be aware of the possibility of a reversible ganciclovir induced ataxia and encephalopathy.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES