KEYWORDS
Dyspnoea, internist, lung ultrasound, medical training
INTRODUCTION
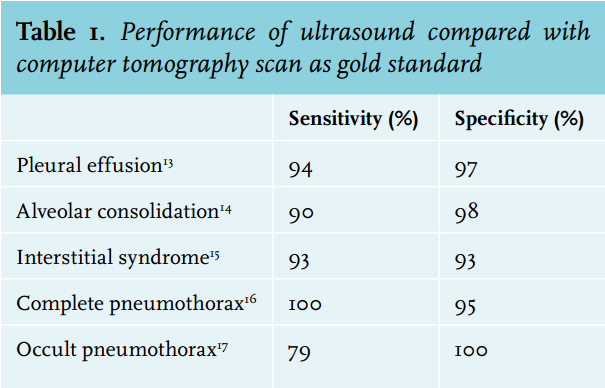
The lungs can provide a wealth of diagnostic information, as they represent the crossroads of respiration and circulation. However, physical examination of the lungs remains a significant challenge. This is largely due to the poor acoustical performance of the stethoscope. Even seasoned physicians may fail to become experts at this 19th century technique.1 For example, for detecting congestive heart failure or pneumonia, auscultation has a low sensitivity.2 Clinical decision-making entered another era when the chest X-ray was introduced, followed by computed tomography (CT). Due to its superior sensitivity, the CT scan is now the gold standard in the diagnosis of community acquired pneumonia.3,4 But CT scanning requires transportation of a potentially critically ill patient, which is not without risk.5,6 In addition CT scanning is associated with significant costs, radiation and contrast burden, which should not be taken lightly.6,7 Lung ultrasonography (LUS) is the answer to these limitations. LUS enables physicians to differentiate between causes of acute dyspnoea within minutes at the bedside, and as such is particularly helpful in the emergency department and on the ward.8,9 LUS is not only superior to the physical examination and chest X-ray, but even comparable to CT for many diagnoses.10-12 Pneumonia, pulmonary oedema, pulmonary embolism, asthma, chronic obstructive pulmonary disease and pneumothorax can be assessed with sensitivity and specificity ranging from 90 to 100% (table 1).
LUS yields important diagnostic information within minutes and is able to answer important binary questions.18 The examination can easily be repeated to evaluate the progress of the disease or the effect of initiated therapy. And importantly, LUS avoids radiation, transport and excessive cost. We have extensive experience with LUS, as it is an essential component of our intensive care ultrasound (ICARUS) curriculum and protocol. It is against this background that we see great potential for LUS in the daily practice of internists. In this narrative review, we therefore aim to provide guidance for internists wishing to adopt LUS.
DEVELOPMENT OF LUS
In medicine, ultrasound frequencies between 1 and 15 MHz are used, to allow for non-invasive visualisation of tissue structures. Ultrasound physics have been extensively reviewed elsewhere.19,20 In short, ultrasound beams travel through tissues until they are reflected when acoustic impedance of the adjacent tissue is different. Ultrasound cannot penetrate bone and is fully reflected by air. Therefore, the lung was considered unsuitable for ultrasound in the past.21,22 However, LUS creates artefacts through the interplay of air, lung tissue, pleurae, fluid and bone. Through reflection, scatter and absorption of ultrasound beams, physiological and pathological processes generate distinctive combinations of artefacts and these speak a language of their own. This was studied in detail by Lichtenstein and colleges who named many of these artefacts and showed their reproducibility.23 In fact, virtually all acute life-threatening respiratory disorders abut the pleural line, generating artefacts that unveil the great potential of LUS.
MACHINE AND PROBE SELECTION
For LUS, virtually any ultrasound machine will do, even legacy equipment. Handy features include a supporting trolley, fast start-up time and a small width, allowing bedside use. Most importantly, as LUS relies on artefacts, it should be possible to suppress all software artefact reduction, such as harmonics, filters and other image optimisation. Higher beam frequency yields higher resolution, but less maximum depth. In practice, linear vascular probes, cardiac phased array probes, or even abdominal probes may be used.
SYSTEMATIC SCANNING
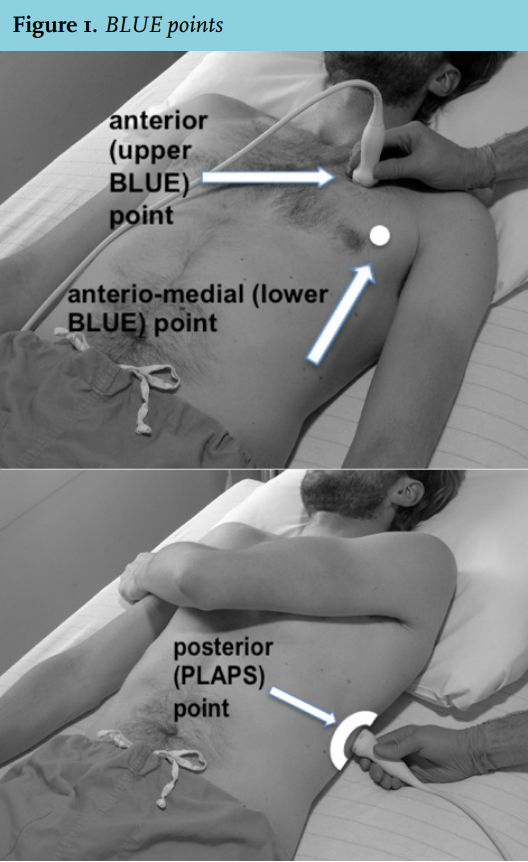
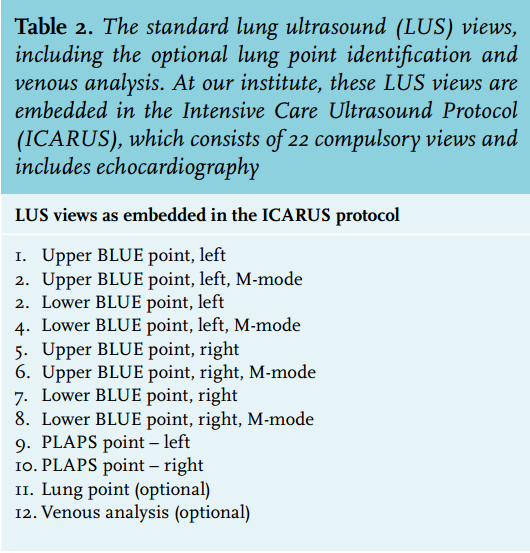
LUS is a trade-off between diagnostic speed and extensive scanning. A reasonable approach is to scan at least three different zones of the lung: anterior, anteromedial and posterior. We recommend the approach suggested by Lichtenstein in his BLUE protocol.8 Figure 1 shows how to find these points. The anterior points are called upper BLUE points and the anteromedial points lower BLUE points, after the protocol. The posterior points are called the ‘posterolateral alveolar and/or pleural syndrome point’, or PLAPS point. In addition, the protocol includes optional identification of the ‘lung point’ and scanning for lower extremity venous thrombosis to aid diagnosis. Table 2 shows the proposed compulsory and optional views for LUS. As discussed in detail below, these views enable discrimination between acute causes of dyspnoea. LUS does not require any cardiac ultrasound imaging, as a cardiac cause of dyspnoea can be diagnosed from lung imaging only.
LUS ARTEFACTS
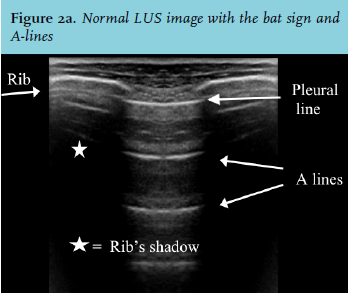
There are many LUS artefacts, but for daily practice only a few of these need to be remembered. It is essential to first identify the pleural line, as most pathology abuts it. To do so, the probe should be positioned perpendicular to the ribs. A rib is easily recognised as a shadow, caused by absorption of ultrasound by bone tissue. The pleural line is horizontal and hyperechoic, situated slightly beneath the two ribs. This yields a characteristic image called the ‘bat sign’ (figure 2a). Under normal circumstances, the parietal pleura and visceral pleura are seen as one line.
Lung sliding
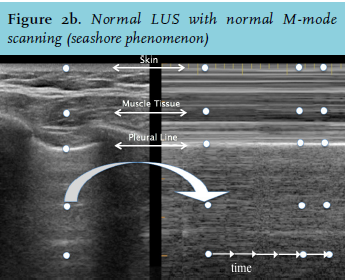
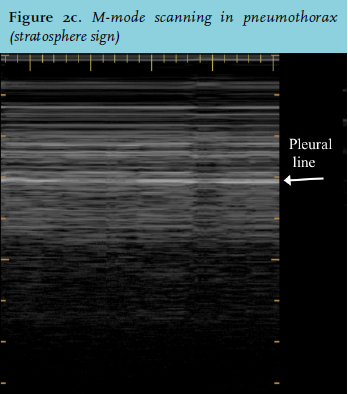
Although visualised as one, respiration causes visceral pleura to slide relative to the parietal pleura. This causes a subtle sparkling to-and-fro movement artefact called lung sliding. Lung sliding indicates that both pleura are adjacent, ruling out pneumothorax at that point.24 Lung sliding is so characteristic that it takes only a few seconds to recognise. Lung sliding can be confirmed using the M-mode. This setting essentially repeats one line of the screen over time. In the presence of lung sliding, the ‘seashore phenomenon’ occurs (figure 2b). If lung sliding is absent, the ‘stratosphere sign’ appears (figure 2c). Of note, abolished lung sliding is far from specific: pneumothorax is the classic example, but a motionless pleural line can also be caused by inflammatory or chronic adherences, fibrosis and atelectasis.
A-lines
An A-line is the main horizontal artefact and a repetition of the pleural line. If ultrasound beams encounter a tissue-air interface, they are reflected back to the probe. However, the probe itself reflects them once again. This causes the beams to travel through the soft tissue a second time. This is called reverberation and causes the visualisation of A-lines (figure 2a). The depth at which an A-line is displayed is always equal to the distance of the pleural line to the probe and can be used to differentiate A-lines from other artefacts. It follows that A-lines represent the presence of air at the pleural line. This can be alveolar air and therefore normal lungs yield A-lines. However, it can also be air outside the alveoli, such as the air between the visceral and parietal pleura in pneumothorax.
B-lines
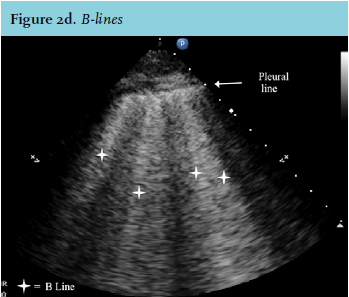
B-lines are the main vertical artefacts and are reminiscent of helicopter search spotlights. They are sometimes referred to as lung rockets or comet tail artefacts. However, strictly speaking, B-lines are a specific subtype of these. Interstitial oedema first appears in the subpleural interlobular septa which are surrounded by alveolar gas. Ultrasound beams entering this small pleural line-fluid-air system are reflected again and again, essentially being trapped. This results in many to-and-fro moments, generating a long vertical hyperechoic artefact, the B-line. Thus, by definition, B-lines arise from the pleural line. They erase A-lines and immediately rule out pneumothorax. B-lines are hyperechoic and narrow, span across the whole ultrasound image without fading and move with lung sliding. More than two anterior B-lines are pathological and indicate interstitial syndrome.15 Although semantically unrelated, B-lines correlate with Kerley B-lines on chest X-ray (figure 2d). Any disease affecting the pulmonary interstitium can cause an interstitial syndrome. The commonest cause is pulmonary oedema. The number of B-lines per screen or the distance between B-lines allows assessment of severity. It has been suggested that very dense B-lines, i.e. more than 10 per screen or only 3 mm apart, favour the diagnosis of ARDS.8,23
C-lines, air bronchogram, shred sign and pleural effusions
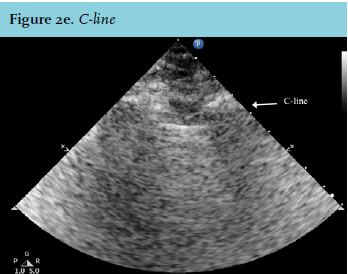
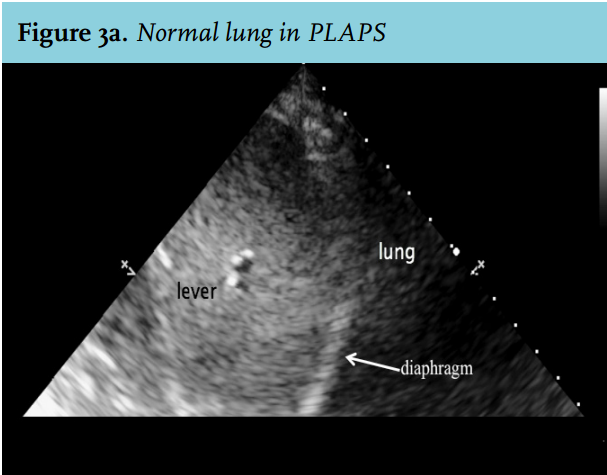
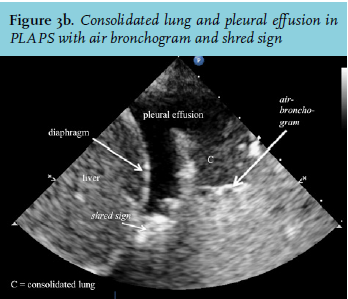
Alveolar consolidation causes typical ultrasound patterns at the different scanning points. At the anterior points, this yields C-lines, identified by a curvilinear aspect of the pleural line (figure 2e). This is caused by adjacent consolidated tissue.23 Pulmonary consolidations are fluid disorders. The non-aerated lung tissue is therefore easily traversed by ultrasound beams and creates an image comparable with that of liver tissue (figure 3a and b). Virtually all consolidations touch the pleural line. However, because of gravity, consolidation usually appears first at the PLAPS point.14 For similar reasons, pleural effusions also first appear at the PLAPS point (figure 3b). They can be hypoechoic or hyperechoic with particles. Hyperechoic effusions are associated with exsudate, but accuracy is not perfect.25 Hyperechoic effusions in combination with consolidated lung tissue at the PLAPS point are associated with the diagnosis of pneumonia. Consolidations can be further analysed by looking for air bronchograms or the shred sign (figure 3b). An air bronchogram is caused by reflection of ultrasound beams in the air-filled bronchi surrounded by consolidated tissue. The shred sign appears when the border of aerated lung and consolidated lung is not sharp. Both are suggestive of pneumonia. Furthermore LUS will identify the presence, size, and nature of an effusion and can be used to guide thoracocentesis (figure 3b).
THE DECISION TREE
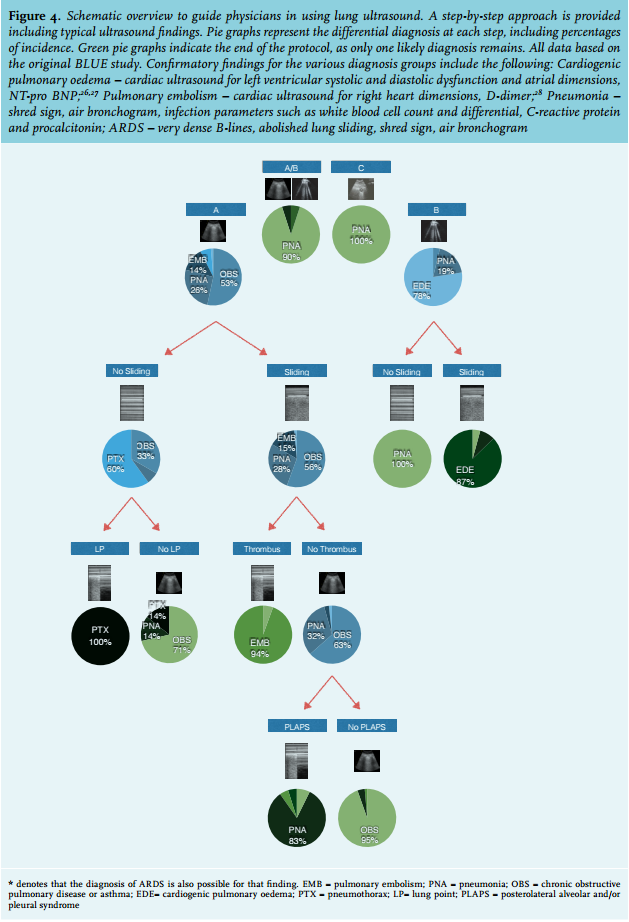
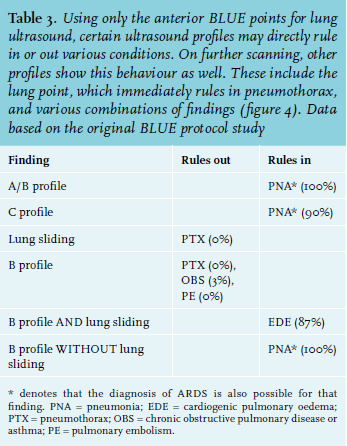
We propose a decision tree for a structured approach of the dyspnoeic patient using LUS. This is based on the original data from the BLUE study.8 This landmark investigation related combinations of ultrasound signs to final diagnosis in acutely dyspnoeic patients presenting at the emergency department. Our decision tree consists of binary questions. Answering these rapidly narrows the differential diagnosis with impressive accuracy (figure 4). In addition, table 3 gives a number of combinations of findings that either directly point to a certain diagnosis or directly exclude it. This may be useful in hyperacute settings. The protocol starts by scanning the anterior BLUE points. The first step in our decision tree is to identify line artefacts. These determine the BLUE profile, depending on the predominance of anterior artefacts. Thus, A and B profiles are distinguished. If one lung shows A-predominance and the other B-predominance, this is called the A/B profile. If any anterior C-line is noted, the C-profile is said to be present, regardless of other artefacts. In case of A or B profiles, the decision tree calls for further analysis based on combinations of lung sliding, findings at the PLAPS point, identification of a lung point and/or venous analysis.
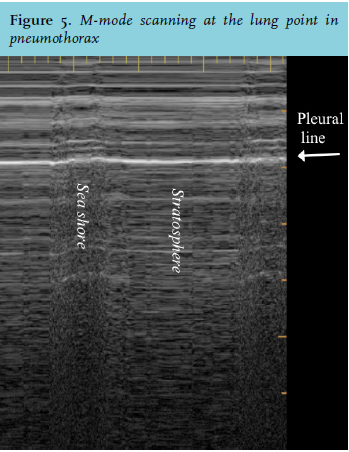
Imaging both PLAPS points again aims to answer a binary question. PLAPS is said to be positive if any sign of alveolar consolidation is seen or if any pleural effusion is seen. If not, PLAPS is said to be negative. Of course, more information can be deducted from the exact findings, but for application of the decision tree, this simple yes or no will suffice. Identification of the lung point to confirm the presence of pneumothorax becomes necessary if an A-profile is present without lung sliding. Starting at the BLUE point where lung sliding was found to be absent, the operator moves the probe down the chest, while staying at the same intercostal space to search for the lung point. This is the point on the thorax where the visceral pleura is sliding in and out of the ultrasound image, due to respiratory movement (figure 5). This implies that M-mode imaging at the lung point will yield a pattern that alternates between the seashore sign and the stratosphere sign. Interestingly, LUS was shown to be superior to bedside chest radiographs for the detection pneumothorax.12 In addition, the size of the pneumothorax may be estimated from the distance between the lung point and the sternum, as the pneumothorax extends anteriorly from this point.
Venous analysis is not performed routinely for LUS, but can be of great help in the setting of A-lines with lung sliding. Presence of thrombus in the large veins of the lower extremity strongly suggests pulmonary embolism as the final diagnosis in this situation. Subtle compression manoeuvres starting from the femoral vein can distinguish thrombus from patent veins. Veins can usually be followed up to the popliteal fossa with relative ease. However, venous analysis is not an absolute requirement to narrow down the differential diagnosis. Using the diagnostic tree is fairly straightforward. For example: the presence of lung sliding, bilateral A-lines but without evidence of PLAPS leads to the diagnosis of COPD/asthma.
BECOME AN EARLY ADAPTER
There are limited data on the efficiency of LUS education. Lichtenstein suggests that short sessions, with a total duration of 90 minutes, focusing on lung sliding (yes/ no) and searching for B-lines (yes/no), yield an average accuracy of 95%.23 Medical students using ultrasound identified abnormalities more accurately than certified specialists who performed physical examination.29 This stresses that it is not difficult to learn point-of-care LUS. Recently, an international expert group recommended at least 30 studies to achieve global competency in basic critical care echocardiography and we think the same holds true for LUS.30 Recently, it was suggested to incorporate ultrasound training in standard undergraduate training.31 Ultrasound can also be used for other parts of the body, for example the abdomen, but this is beyond the scope of this review.
OUR EXPERIENCE
At VU University Medical Center (VUmc), we have developed the Intensive Care Ultrasound (ICARUS) protocol and curriculum. The protocol consists of 22 compulsory views (table 2). Eight views are devoted to LUS. The other views are dedicated to echocardiography. This can provide further evidence for the BLUE diagnosis, for example in pulmonary embolism (enlarged right heart) or cardiogenic pulmonary oedema (decreased ventricular function). The program is open to fellows in intensive care medicine and anaesthesiology residents. Intensivists, anaesthesiologists, internists and emergency medicine physicians from the Netherlands and abroad can also take part. Following a two day hands-on introductory course, candidates perform the ICARUS protocol on 50 patients in their own hospital. After 5-10 patients, external candidates return to VUmc for hand-on refinement of their technique on VUmc patients. Following a practical and theoretical exam, candidates become ICARUS certified and are able to perform LUS for clinical purposes. Endorsement of the ICARUS certification program by the Netherlands Society for Intensive Care Medicine and other ultrasound courses may facilitate widespread dissemination of ultrasound knowledge amongst physicians, including those specialising in internal medicine, in all hospitals in the Netherlands.
LIMITATIONS
Performing a LUS examination and interpreting the acquired images correctly requires formal training. The reliability of LUS is therefore dependant on the experience of the ultrasonographer. It is important to note that point-of-care ultrasound does not replace specialised ultrasound examinations by comprehensively trained physicians, such as an echocardiography by a cardiologist. Also patient-dependent factors such as obesity, the presence of subcutaneous emphysema and wound dressings alters the transmission of ultrasound beams and makes ultrasound a challenge in some patients. Most of the studies validated ultrasound for acute dyspnoeic patients in the emergency department and ultrasound has yet to be validated for other indications.8 Acquired images should be uploaded to a hospital server so they can be reviewed by more experienced ultrasonographers, discussed with colleagues and used to compare with newer images to evaluate the effect of initiated therapy or progress of the disease over time.
CONCLUSION
LUS is a rapid diagnostic bedside tool that is easily accessible for internists and should therefore be considered an extension of physical examination and used in combination with laboratory tests and when needed other imaging techniques. Answering clinical questions with LUS enables immediate therapy for potentially lethal conditions. LUS will give the internist an advantage in clinical care in the near future.
DISCLOSURES
The authors declare no conflicts of interest. Institutional funding only.
REFERENCES