
KEYWORDS
Purpura fulminans, toxic epidermal necrolysis, disseminated intravascular coagulation, sepsis
INTRODUCTION
Acute purpura fulminans is a rare and life-threatening disorder, frequently associated with acute disseminated intravascular coagulation secondary to sepsis. The features of purpura fulminans include tissue necrosis and small vessel thrombosis.1 Toxic epidermal necrolysis (TEN) is characterised by extensive apoptosis and detachment of the epithelium of the skin and mucous membranes and is mostly attributable to adverse drug reactions.2,3 Both diseases have a high morbidity with mortality rates up to 50%.3,4 Early recognition as well as identification and treatment of the aetiology may halt disease progression and prevent further complications. We present a case of severe sepsis-induced purpura fulminans resulting in severe epidermolysis, mimicking TEN.
CASE REPORT
A 56-year-old woman presented to the emergency department as self-referring patient with acute fever, chills and severe pain in both legs. Her medical history revealed depression, breast augmentation and alcohol abuse. Her current medication consisted of ibuprofen, citric acid and sodium chlorite 25%. The last two are for dermal application only, but the patient used these orally, unaware of the details of the prescription. Apart from hay fever, she had no known allergies. On physical examination she was confused and severely ill, with tachypnoea and a pulse oxygen saturation of 98% without supplemental oxygen. Capillary refill time was delayed with cold, white extremities and cutis marmorata, a pulse of 90 beats/minute, and blood pressure 130/95 mmHg. Her body temperature was 36.8° Celsius and neurological, pulmonary, cardiac and abdominal examination showed no abnormalities. Because of suspected aortic thrombosis, CT abdomen was performed which showed no vascular or other abnormalities. Urine samples and chest X-ray showed no signs of infection. The presumed diagnosis of septic shock with unknown focus was made and blood cultures were drawn after the first bolus of antibiotics was administered. She was treated with cefuroxime, clindamycin and tobramycin.
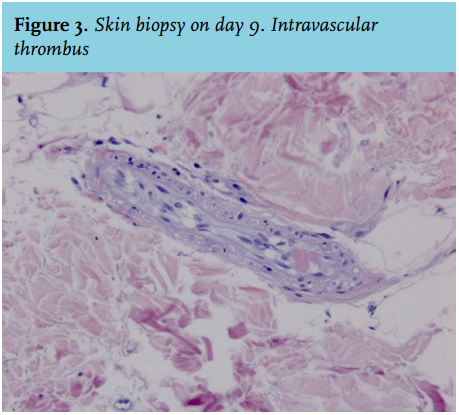
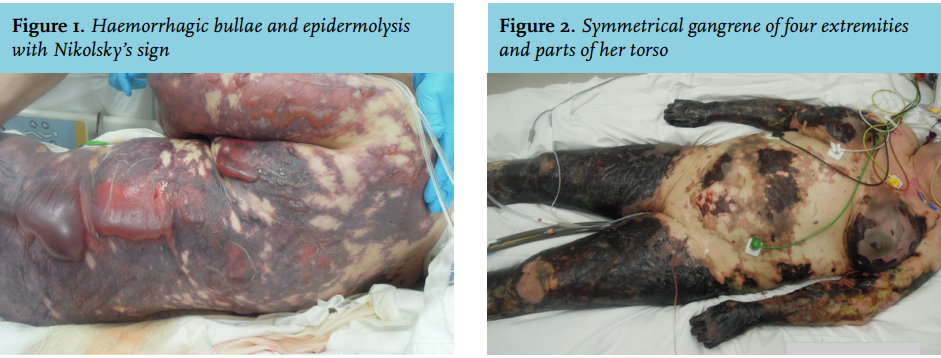
Despite volume resuscitation, vasopressor therapy and initiation of mechanical ventilation in the ICU, her clinical condition deteriorated into multiple organ failure (ARDS, acute renal failure and disseminated intravasal coagulation, see table 1). Furthermore, she rapidly developed a sharply demarcated retiform purpuric skin rash with a positive Nikolsky’s sign, resulting in haemorrhagic bullae and epidermolysis in the next two days (figure 1). Eventually, this resulted in bilateral symmetrical gangrene of four extremities, parts of her torso and face, without involvement of the mucosa (figure 2). Skin biopsies on day 9 and 10 showed a largely necrotic epidermis with subepidermal blistering, intravascular thrombi and extravasation of erythrocytes (figure 3). Although blood cultures remained negative, blood samples drawn in the emergency department eventually showed a sequence 100% identical to the 16S rRNA gene sequence of Streptococcus pneumoniae.
Because of the severe epidermolysis with 67% of the body surface area involved, she was transferred to the ICU of a burn centre when her condition had stabilised two weeks after admission. There, she underwent an amputation of the right lower limb and necrotectomy of her left leg, abdomen and right mamma. Despite maximal intensive care support, the patient deteriorated progressively due to nosocomial infection, with positive cultures with Candida albicans, Enterococcus faecium and Aspergillus fumigatus. For reasons of futility, taking into account this patient’s goals and her extensive mutilation and persisting multi-organ failure, treatment was discontinued and she died on day 29.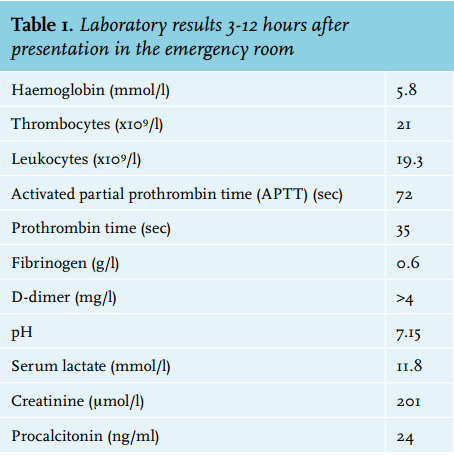
DISCUSSION
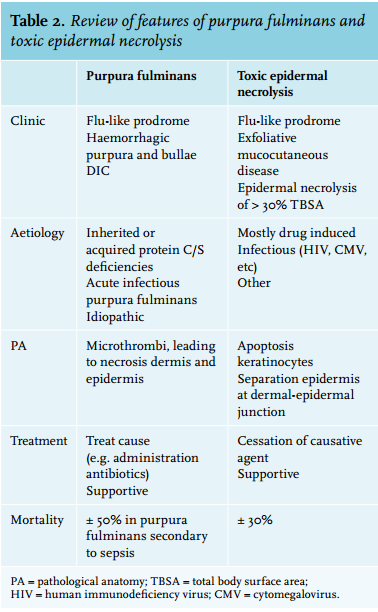
Both purpura fulminans and TEN are rare and life-threatening disorders with a high mortality (up to 50% and 30% respectively).5 Epidermal necrolysis secondary to the thrombotic and haemorrhagic cutaneous infarction in purpura fulminans during sepsis might be hard to differentiate from other life-threatening skin disorders, such as TEN (see table 2 for a review of features of purpura fulminans and toxic epidermal necrolysis). Moreover, both syndromes can be present simultaneously or successively, as has previously been described.3 Early recognition and treatment of the underlying cause of both diseases is vital to prevent further disease progression and reduce the incidence of complications.
Purpura fulminans is a rapidly progressive disorder, accompanied by vascular collapse and disseminated intravascular coagulation,6 which is characterised by the formation of microthrombi through activation of the inflammatory cascade and consumption of protein C, S, and antithrombin III, leading to widespread intravascular thrombosis.4 The consumption of coagulation factors and platelets in turn led to bleeding and haemorrhagic infarction of the skin.7 Multiple organ failure is common, since the haemorrhagic infarction is not limited to the skin, but also affects lungs, kidneys, central nervous system and adrenal glands.8 Acute infectious purpura fulminans usually presents during severe sepsis, particularly following exposure to endotoxin producing bacteria.1 Although it is common in meningococcal infection, Streptococcus pneumoniae is also a well-known cause.8 Previous literature shows that 6% of patients with pneumococcal sepsis developed tissue necrosis resulting in symmetrical peripheral gangrene.9 Treatment is supportive and includes treatment of the underlying cause, most importantly the administration of a broad-spectrum antimicrobial agent.3,8 Complications of purpura fulminans are scarring, secondary infection, digital or limb necrosis and amputation.
TEN is defined as extensive skin sloughing with the involvement of mucosa, with epidermal necrolysis in > 30% of the body surface area.3,10 Most cases of TEN are drug induced (80-95%) and immune mediated, combined with a genetic susceptibility for drug hypersensitivity. Several immune mediators, including the key mediator granulysin, a cytotoxic protein produced by natural killer cells and cytotoxic T lymphocytes, are suggested to be responsible for extensive apoptosis in keratinocytes.11
Multiple organs may be involved, including the respiratory, renal and hepatic system. Its primary treatment is instant withdrawal/cessation of the causative agent.10 Further treatment is supportive with special care for the skin lesions and prevention of secondary infections.
In the case we present here, we suspected a sepsis on day 1, rapidly evolving into sepsis-induced purpura fulminans and this diagnosis was eventually histologically supported by the presence of fibrin thrombi on skin biopsy. However, because of the impressive epidermolysis on day 2-4, the positive Nikolsky’s sign of the skin and absence of bacterial growth in blood cultures, we questioned this diagnosis. We considered these skin lesions to be TEN provoked by the use of ibuprofen, with secondary disseminated intravascular coagulation. Initial biopsy showed an epidermal necrosis and low epidermal or subepidermal detachment of the skin, both indicative of TEN, but not specific for this disease. However, the second skin biopsy showed necrosis due to embolism with microthrombi, extravasation of erythrocytes and detachment of the epidermis. Retrospectively, the first skin biopsy was also compatible with purpura fulminans with thrombosis of a larger vessel more proximal to the biopsy site. Epidermolysis is a well-known phenomenon in purpura fulminans. Furthermore, in this stage, the presence of 16S rRNA gene sequence of S. pneumoniae was confirmed which contributed to the diagnosis of purpura fulminans.
Sequence analysis of the 16S rRNA gene is useful for bacterial detection and identification and remains the standard approach in investigating microbial diversity.12,13 Its main advantage is the processing time to detect and identify bacteria, which is significantly shorter than a culture-based approach.14 Also, it is not dependent on the presence of replicating organisms and can be detected from intact dead or living bacteria. In the clinical setting, using 16S RNA sequencing accurately detects bacteria in over 90% of all cases of culture-confirmed blood stream infections and can detect up to 71% additional blood stream infections compared with blood culture alone.14,15 16S rRNA gene PCR for detection of bacterial DNA applied directly to peripheral whole blood of patients suspected of bacteraemia has been documented to have a sensitivity and specificity of 66.7-77.8% and 94.4-99.3% respectively, excluding contaminants.14,16
In the case presented here, we sequenced the variable regions 1, 2 and 3 using standard BLAST for the comparison. The sequence showed 446 base pairs identical to Streptococcus pneumoniae forward and reverse and resulted in a 100% query cover and 100% match with exclusively S. pneumoniae (23 strains). As for the reliability of species identification, it is important to discriminate between S. pneumoniae and other closely related species such as S. oralis and S. mitis, which can have overlapping 16S RNA sequences. If results show less than 100% homology, additional testing with a S. pneumoniae specific PCR, such as the lytA gene, is recommended to confirm the 16S sequence diagnosis.17 In the case presented here, additional testing was not performed as 100% homology was found. However, the possibility of a contamination of the blood sample should be taken into account.
In conclusion, we present a case with a suspected rapidly progressive, severe pneumococcal sepsis induced purpura fulminans complicated by multiple organ failure, severe epidermolysis and cutaneous necrosis. We show the diagnostic challenge to differentiate between purpura fulminans and TEN, as the extensive epidermolysis in purpura fulminans may mimic TEN. Through additional diagnostic testing with repeated skin biopsies and 16S rRNA gene sequencing, diagnosis of purpura fulminans was eventually thought most suitable.
DISCLOSURES
The authors declare no conflicts of interest.
REFERENCES