KEYWORDS
Cushing’s syndrome, ectopic ACTH production, large cell neuroendocrine carcinoma, prostate cancer
INTRODUCTION
Adenocarcinoma of the prostate is the most frequent malignancy diagnosed in men. In metastatic disease, blocking androgen synthesis and/or the androgen receptor is the cornerstone treatment modality. Ultimately, all patients with metastatic prostate cancer (PC) will develop resistance with a fatal outcome. In late-stage metastatic prostate cancer, typically in the setting of aggressive visceral metastases, clinical manifestations attributed to neuroendocrine tumour dedifferentiation can become apparent.
CASE REPORT
A 75-year-old man with a two-year history of metastatic prostate cancer was admitted to the hospital due to macroscopic haematuria. He had indistinct complaints of muscle weakness and emotional lability. His hormonesensitive prostate cancer (HSPC) had been treated with upfront docetaxel in combination with a luteinising hormone releasing hormone agonist, but after one year, the disease was considered castrate-resistant prostate cancer (CRPC) and treated with enzalutamide. Physical examination revealed a blood pressure of 183/83 mmHg, a mild dorsocervical fat pad, and bilateral pitting oedema. There was no hyperpigmentation, moon facies, or abdominal striae. Initial laboratory examination revealed a hypokalaemia of 2.7 mmol/l (3.5-5.0 mmol/l), a metabolic alkalosis, a prostatespecific antigen (PSA) of 90ug/l (< 4.0 µg/l), and lactate dehydrogenase (LDH) 909 U/l (< 248 U/l). Additional tests showed a midnight cortisol in saliva (340 nmol/l; N < 4 nmol/l), 24-hour urinary free cortisol (UFC) 16,000 nmol/24 h (15-130 nmol/24 h), serum cortisol 1.750 nmol/l (130-540 nmol/l), and ACTH 40.4 pmol/l (1.60-13.9 pmol/l). Cortisol was not suppressed (1.553 nmol/l) after a low dose of dexamethasone (1 mg) overnight. Abdominal CT scan demonstrated stable para-aortal lymphadenopathy and bone metastases, but a progressive tumour of the prostate and bilateral enlarged adrenal glands. An MRI scan of the pituitary did not reveal any abnormalities. Pathology of the prostate biopsies showed a large cell neuroendocrine carcinoma (LCNEC) of the prostate (figure 1). Immunohistochemical staining of the prostate biopsy showed tumour cells positive for CD56, chromogranin, and synaptophysin, but staining for ACTH was negative. An additional PET scan with Ga-68-Edotreotide (DOTATOC) showed increased expression of somatostatin receptors in a subset of the bone metastases and part of the prostate. 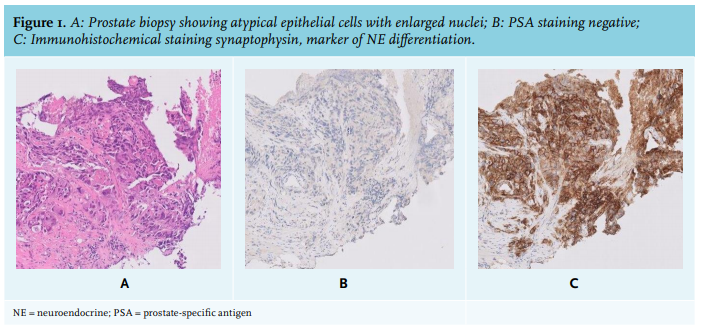
The diagnosis of Cushing’s syndrome was made, most probably due to ectopic production of ACTH by a metastatic LCNEC of the prostate. The patient was treated symptomatically with potassium chloride and potassiumsparing diuretics (spironolactone), in combination with ketoconazole, a cortisol synthesis blocking agent. Urinary cortisol excretion was monitored to evaluate the efficacy of this treatment. After five days of ketoconazole 400 mg twice daily, 24-hour urinary free cortisol excretion declined to 3.500 nmol/24 h. We decided not to perform additional invasive testing, bilateral adrenal extirpation, or to initiate palliative chemotherapy as the medical condition of the patient deteriorated. The patient died within several weeks after diagnosis.
DICUSSION AND CONCLUSION
ACTH-dependent Cushing’s syndrome is caused by ectopic ACTH secretion in approximately 10-15% of cases. It has been associated with a wide variety of tumours, usually carcinomas. Ectopic secretion is most frequent diagnosed in pulmonary small cell cancer but also occurs in other, often malignant neuroendocrine tumours.1-2 A small cell neuroendocrine tumour of the prostate has been reported in 1-3% of cases as the cause for Cushing’s syndrome.3 To the best of our knowledge, Cushing’s syndrome caused by ectopic ACTH secretion by a LCNEC of the prostate has not been reported in the literature to date.
The lack of abnormalities on an MRI scan of the pituitary decrease the likelihood that an ACTH-producing pituitary microadenoma was the source of the ACTH hypersecretion, although it is important to note that a negative pituitary MRI in itself cannot exclude Cushing’s disease. The timeline of the clinical symptomatology of Cushing’s syndrome in our patient is also suggestive of a relationship with the patient’s prostate cancer since symptoms only recently occurred and coincided with the clinical progression of the metastatic disease. Furthermore, the negative immunohistochemical ACTH staining does not exclude an ectopic ACTH-secreting tumour as it has been reported that tumour immunostaining for ACTH can be negative in up to 30% of ACTH-secreting tumors.2 Neuroendocrine cells, which lack androgen receptors, are a part of the normal prostate tissue, where they play a regulatory role in proliferation and secretion of the prostate epithelium.4-5 In vitro experiments have shown that during androgen deprivation treatment (ADT), prostate adenocarcinoma cells have the capacity to transdifferentiate to a more neuroendocrine (NE) phenotype, a process called NE transdifferentiation. Restoring the androgens can suppress this process.6-7 Clinically, a substantial proportion of pre-treated end-stage prostate cancer patients show salient features of de novo small neuroendocrine cell carcinomas, mostly with an aggressive behaviour, and often with visceral metastases. Although most patients are not routinely biopsied in end-stage disease, it has been estimated that at least 25% of the patients with advanced prostate cancer will develop neuroendocrine prostate cancer.8
LCNEC of the prostate is extremely rare as indicated by a recent systematic review and pooled analysis of 20 patients.9 In most patients, the LCNEC of the prostate occurred after long-standing androgen deprivation in the setting of prostate cancer. The clinical manifestations were aspecific and most cases, like our patient, were diagnosed at the time of palliative transurethral resection of the prostate for urinary symptoms. Ectopic hormonal production was not reported. Prognosis is poor, and although systemic chemotherapy may have some benefit, most patients die within a few months.9
The symptomatic treatment of ectopic Cushing’s syndrome includes potassium suppletion, potassium sparing diuretics, cortisol synthesis blocking agents (e.g., ketoconazole, metyropone, etomidate), and bilateral adrenal extirpation. As is illustrated by our case, ketoconazole monotherapy is unlikely to suffice and addition of other cortisol blocking agents or even bilateral adrenalectomy should be considered. After a full biochemical control, palliative chemotherapy can be considered in order to achieve tumour shrinkage and thereby decrease ectopic ACTH production.
LCNEC of the prostate is extremely rare and mostly occurs after long-term hormonal therapy of prostatic adenocarcinoma. NE differentiation during ADT should be suspected in all prostate cancer patients with rapid clinical deterioration.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES