KEYWORDS
Engerix®, Fendrix®, hepatitis B, HIV, non-responder, vaccination
INTRODUCTION
The higher risk of hepatitis B infection in HIV-infected patients, often with an immune compromised status and a known diminished rate of response to hepatitis B virus (HBV) vaccination,1-4 affords a tailored vaccination strategy such as double-dosing the HBV vaccination5,6 or doubling the number of hepatitis B vaccine injections over time.7,8 For management of vaccine non-responders, there are no exact guidelines. Most studies in literature have found a variable response rate of 74-83% to a second series of vaccinations among non-responders.9,10 Revaccination of HIV-infected individuals with double doses of commercially available hepatitis B vaccines in non-responders to primary single-dose vaccination also has been successful in 50% of these individuals.11 The introduction of Fendrix® provides an efficient well-tolerated alternative with superior immunogenicity. Fendrix® contains the adjuvant aluminium phosphate and 3-O-desacyl-4’-monophosphoryl lipid A (a Toll-like Receptor 4 agonist). The immunogenicity of Fendrix® was assessed in several clinical trials in healthy volunteers as well as in pre-haemodialysis and haemodialysis patients.12-16 Overall, due to the improved adjuvant system, Fendrix® demonstrated higher seroprotection rates and higher antibody concentrations in all studies. Decline of antibody concentration in haemodialysis patients followed the same course as that shown for other plasma- and yeast-derived HBV vaccines, with a faster decline the first 12 months and a slower decline thereafter. The aim of our study was to investigate the effects of Fendrix® versus Engerix® vaccinations in previously non-responsive HIV-infected subjects in a randomised controlled trial.
PATIENTS AND METHODS
Patients and study design
The study was designed as a two-arm, randomised, open-label pilot study in human immunodeficiency virus (HIV)-infected, hepatitis B virus (HBV)-uninfected subjects, naïve to Fendrix® vaccination. We selected a subset of non-responding patients in the Erasmus Medical Center (MC). These patients came from two cohorts. First, we used a previous multi-centre study initiated by our hospital where a total of 811 patients were vaccinated according to an accelerated schedule (t = 0, 1, 3 weeks) or a standard schedule (t = 0, 4, 24 weeks). About 50% of these patients responded.1 A total of 144 non-responding patients who were in care at the Erasmus MC subsequently received a double-dose HBV revaccination (t = 0, 4, 8 weeks) with a 51% response.11 The second cohort comprised of non-responders, not included in previous studies, who received a first single-dose HBV vaccination as part of their standard of care schedule; because of non-response, they were also revaccinated with a double-dose HBV schedule. Patients were vaccinated with 10 mcg HBvaxPro® vaccine or 20 mcg Engerix® vaccine in the primary schedules and 20 mcg HBvaxPro® vaccine in the double-dose schedule. These two vaccines are interchangeable.17 A total of 48 patients in the non-responding cohort via these two routes were included in this study. Eligible patients were aged ≥ 18 years, had a CD4+ cell count > 200/mm3 , a negative hepatitis B surface antigen (HBsAg), no antibody to hepatitis B core antigen (anti-HBc), and no antibody to hepatitis B surface antigen (anti-HBs) titres. Exclusion criteria were hepatitis C co-infection, pregnancy, radiation therapy, cytotoxic agents, or any immune modulator treatment. Subjects who fulfilled eligibility requirements were randomised 1:1 to receive Fendrix® (t = 0, 4, 8, 24 weeks, according to the manufacturer) or double-dose Engerix® (t = 0, 4, 24 weeks, standard time schedule) vaccinations intramuscularly in the deltoid region. Blood samples were taken at the 28-week time point for quantitative anti-HBs testing (Abbott ARCHITECT® system). The primary efficacy endpoint was the proportion of responders, defined as the number of patients with anti-HBs titres ≥ 10 IU/l at week 28. Secondary endpoint was a difference in antiHBs titre response between Fendrix® and Engerix®.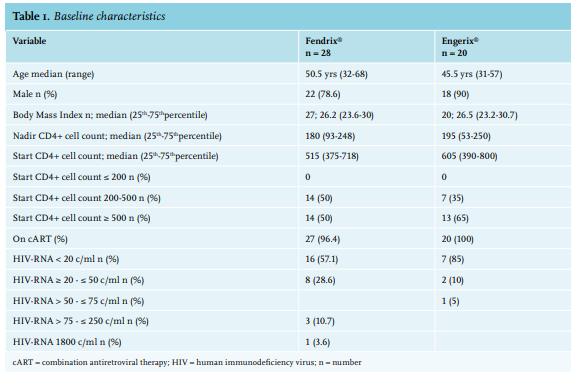
Statistics
A logistic regression analysis was performed to analyse the primary endpoint. We included vaccine type (reference level was Engerix®) in the model because we wanted to investigate the differences in the outcome between the two arms of the study. In this model, we corrected for other baseline covariates including the HIV-RNA load and CD4 count at study inclusion, nadir CD4, age, and sex. The difference between anti-HBs titre was assessed by Wilcoxon rank sum test. Approval was obtained from the Medical Ethics Committee of the Erasmus Medical Center (MEC-2010-390) and informed consent was obtained from each patient.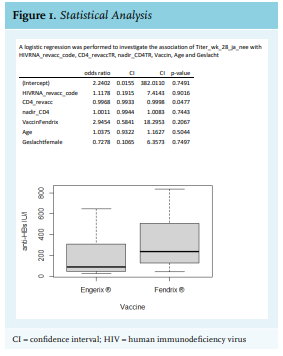
RESULTS
Forty-eight HIV-infected patients were included in the study. During the course of the study (March 2011 – June 2013), the guidelines on primary HBV vaccination in HIV-infected patients in the Netherlands were changed (December 2012) to a double dose. Therefore, enrolment in the study was prematurely terminated as subsequent patients did not fulfil the inclusion criteria of the study anymore.
Twenty patients received Engerix® and twenty-eight received Fendrix®. All Engerix® patients received three double dosages of the vaccination; all Fendrix® patients received four vaccine doses according to the manufacturer’s instructions. Patient characteristics in both groups were similar at baseline. Table 1 reports the distribution of age, gender, body mass index, start CD4+ cell count, nadir CD4+ cell count, usage of combination antiretroviral therapy (cART), and HIV-RNA at start of vaccination. Both groups consisted of mostly males, with similar and current CD4+ cell counts in the normal range and nearly all patients were on cART with a reasonable to excellent viral suppression.
The response rates, defined as anti-HBs ≥ 10 IU/l, at week 28 in the Fendrix® arm and the Engerix® arm were 85.7% and 65.0%, respectively (p = 0.09). A mean 75% responded to either vaccination. As is shown in figure 1, there was no significant difference in the proportion of patients with anti-HBs ≥ 10 between the two used vaccine types if we correct for HIV-RNA at vaccination, CD4+ cell count at vaccination, nadir CD4+ cell count, type of vaccine, age, and gender. In addition, we found no significant difference between anti-HBs titres after vaccination by either vaccine strategy. All included patients received the complete vaccination series. Compliance to the vaccination schedule in the Fendrix® group between the first and fourth vaccine (t = 0 and 24 weeks) was 64.2% (18/28 patients). Of the remaining 10 patients, 2 were vaccinated at week 23, 4 at week 25, 2 at week 26, 1 at week 27, and 1 at week 34. In the Engerix® group, compliance between the first and third vaccine (t = 0 and 24 weeks) was 60% (12/20 patients). Of the remaining 8 patients, 1 was vaccinated at week 22, 1 at week 23, 4 at week 25, 1 at week 26, and 1 at week 50.
DISCUSSION
In our observational study of the effect of Engerix® and Fendrix® revaccination in a previously non-responder group to HBV primary and booster vaccination, we found a response rate of 65.0% and 85.7%, respectively. No superiority of one of the investigated hepatitis B vaccines was shown in this cohort because the number of patients needed for this analysis were not achieved. HBV vaccination in HIV-infected patients is a challenging opportunity for several reasons. First, the prevalence of HBV infection among men having sex with men (MSM) is high and unprotected sex imposes an increased risk of contracting the disease. Second, adherence to the standard HBV vaccination schedule is a matter of concern and has to be proven difficult in daily practice for both doctor and patient,18-21 and third, HIV-infected patients have an impaired response and show a wide diversity of seroconversion to HBV vaccination as summarised in the review of Mena et al.22 With the use of Tenofovir (TDF) as part of a first-line cART regimen in HIV-infected patients, the viral load in treated patients decreases, which also decreases the risk of HBV transmission. However, considering the latest developments in HIV treatment where non-TDF-containing cART regimens as part of dual treatment or single tablet regimens are prescribed (for example, Dolutegravir/Abacavir/lamivudine, Dolutegravir/ Rilpivirine, Dolutegravir/lamivudine) the necessity of effective immunity against HBV is still ongoing.
To our knowledge, only two studies have published data on the effect of Fendrix® as a revaccination strategy in HIV-infected patients. In the study of de Silva et al., 22 patients who had previously not responded to at least one course of standard vaccines showed an overall response rate of 95%.23 Machiels et al. showed, in a retrospective analysis of 100 patients with HIV and nonresponding to prior HBV vaccination, a seroconversion rate of 81% irrespective of the Fendrix® scheme used or the amount of vaccines given.24
In our previous studies, we achieved an overall response rate to HBV vaccination of 75% among HIV-infected patients (around 50% responded on primary single-dose HBV vaccinations and 51% additional success rate was achieved after a double-dose booster HBV vaccination scheme).11 In this study, a total of 75% patients responded to the Fendrix® or Engerix® vaccinations. This means that an additional 19% of HIV-infected patients responded and thus, all together (primary, booster, and re-booster HBV vaccination), an ultimate overall response to HBV vaccination in HIV-infected patients of around 94% can be achieved. These results suggest that continuing HBV vaccination in non-responders is worth the effort.
Although there was a trend of higher anti-HBs levels in the Fendrix® group responders, there was no significant difference in overall response between the two groups with the data we have collected. We realise that applying a regression model on such a small number of subjects should be done with caution and that no strong conclusions can be made.25 However, the results can be used for a future study. The number of included HIV-infected patients needed to achieve reliable answers were not achieved due to interruption of the study. Since 2012, Dutch guidelines advise the initiation of a primary vaccination scheme with double-dose HBV vaccination at t = 0, 4, 24 weeks in HIV-infected patients when CD4 count ≥ 350 cells/mm3 , followed by double-dose revaccination at t = 0, 4, 8 weeks in non-responders. Although the effect of the modification of the guideline is not yet studied, we assume that the number of non-responders is decreasing. The changed guidelines made it impossible to include more patients in our Fendrix® versus Engerix® study. As there may be a difference between double-dose HBV vaccination and Fendrix®, it could be interesting to compare these two vaccines as a first vaccination schedule in a randomised controlled trial. While HIV patients on cART in the Netherlands do have repeated visits and are generally compliant, the approach of continuing HBV vaccination until adequate response is less favourable. Primary immunisation series with a more effective vaccine is of great relevance since it would require fewer injections and appointments, thereby reducing the overall cost.
In addition, it is important to realise that our patients belong to a group of non-responders to initial and revaccination schedules. Starting with a strong vaccine in the first schedule and being able to avoid re-vaccination seems reasonable and could be cost saving. Alternatively, our study signals that a third round of HBV vaccination is worth the effort in previous non-responders.
DISCLOSURES
The authors declare that there are no conflicts of interest. The data from the Fendrix® patients were used in a retrospective multicentre study published in AIDS. 2019 Mar 1;33(3):503-507. doi: 10.1097/ QAD.0000000000002085. For this study, free Engerix® and Fendrix® vaccines were received from GlaxoSmithKline.
REFERENCES