KEYWORDS
Choosing Wisely, quality improvement, unnecessary procedures
INTRODUCTION 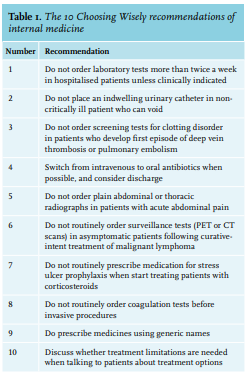
To improve quality of care and reduce healthcare costs, reducing low-value care is a key element. Low-value care is care that is unlikely to benefit the patient given the cost, available alternatives, and preferences of patients.1 In addition, this includes overuse of unnecessary medical care and this may cause harm to patients. Earlier research showed that approximately a quarter of all medical care is. unnecessary.2 The Choosing Wisely campaign, a physician-driven campaign to create conversations between physicians and patients about unnecessary tests, treatments, and procedures, was launched by the American Board of Internal Medicine (ABIM) Foundation in 2012 to address low-value care.3 At this moment, Choosing Wisely has spread to more than 20 countries worldwide. The ‘Choosing Wisely Netherlands Campaign’ started in 2014.4 A main part of this campaign was the creation of Choosing Wisely recommendations by scientific societies, which are evidence-based lists of recommendations or ‘Things Providers and Patients Should Question’ to address commonly used low-value care. The Netherlands Association of Internal Medicine (NIV) developed a list of recommendations of 10 wise choices. The development of the list was by a bottom-up approach, through a survey via e-mail to all NIV members asking for any item to be proposed. Three criteria for a Choosing Wisely recommendation were: (1) evidence based, (2) room for improvement in quality of care and/or costs, and (3) broad consensus. During an invitational conference all subspecialty societies discussed which 10 choices were the best. This leaded to a list of 10 recommendations in Dutch (Supplementary Appendix)*. A translated version is found in table 1.
In the United States, early trends of seven Choosing Wisely recommendations showed only minimal benefits.5 The next step in the Choosing Wisely campaign is a shift from recommendation development towards implementation,6 because raising awareness of evidence about low-value care is generally insufficient to change clinical practice.7,8 In 2014, these Choosing Wisely recommendations of internal medicine were published and communicated explicitly by the NIV. In the present survey, we explored the current implementation of the Choosing Wisely recommendations of internal medicine. We aimed that minimal 80% of the physicians self-reported that the recommendation was implemented, then we presume the recommendation was part of regular care.
MATERIALS AND METHODS
We actively surveyed physicians and residents to determine the implementation of the Choosing Wisely recommendations in the departments of internal medicine in 2018. The survey was performed during a presentation about the Choosing Wisely Netherlands campaign by a PhD student of internal medicine (BJL). In addition to the survey, the goal of the presentations was to inform attendees once again about the campaign and the current status. For feasibility reasons, we visited half of all university medical centres (UMCs) in different parts of the Netherlands, and one teaching hospital and one nonteaching hospital in the direct environment of that UMC. The presentations were mostly planned during existing meetings, for example the morning report. During the presentation we asked all attendees to vote through VoxVote, which is a free mobile voting tool via the Internet. All attendees, physicians, and residents, were eligible to participate voluntary. The survey contained 11 closed-ended questions in Dutch, including the option ‘not applicable’. Afterwards, there was a discussion per recommendation to evaluate possible barriers for the implementation. There was no incentive for completing the survey. The presentation can be found in the supplementary appendix.
STATISTICAL ANALYSIS
Categorical data were summarized as frequencies and percentages. Chi-square or Fisher’s exact test were used to assess relationships between variables, especially the relationship between awareness of the Choosing Wisely campaign and total score of self-reported implementation of recommendations. A two-sided p value less than 0.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA) and R software, version 3.6.1 (R Foundation, Vienna, Austria).
RESULTS
Between May 17th, 2018 and November 5th, 2018, we visited four UMCs, five teaching hospitals, and four nonteaching hospitals. We surveyed 281 physicians and residents of the departments of internal medicine, consisting of 158 respondents from a UMC, 91 from a teaching hospital, and 32 from a nonteaching hospital (table 2). We received 2625 answers via VoxVote, which is an 85% response rate of all starting participants. The results per hospital were send as feedback for internal use.
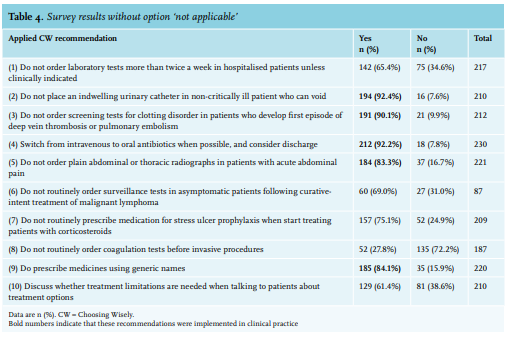
Four years after the introduction of the Choosing Wisely Netherlands Campaign, 178 (68.5%) of the 260 physicians were not aware of the international, national campaign, or the national Choosing Wisely recommendations of internal medicine (table 3). In total, we had 2365 responses to the questions about the implementation of Choosing Wisely recommendations. We excluded the 362 ‘not applicable’ answers; of all recommendations, 1506 (75.2%) of 2003 answers stated that they were applied in clinical practice. We found no differences in the reported implementation of the recommendations between responders who were aware versus those unaware of the Choosing Wisely campaign, 529 (76.1%) of 695 versus 854 (74.2%) of 1151; p = 0.357, respectively.
The percentages not applicable were less than 20% for all recommendations (table 3), except for recommendation 6 ‘Do not routinely order surveillance tests in asymptomatic patients following curative-intent treatment of malignant lymphoma’. For this, 62.5% of the attendees stated that this recommendation was not applicable to their clinical practice, because only haematologists treat these patients in the Netherlands.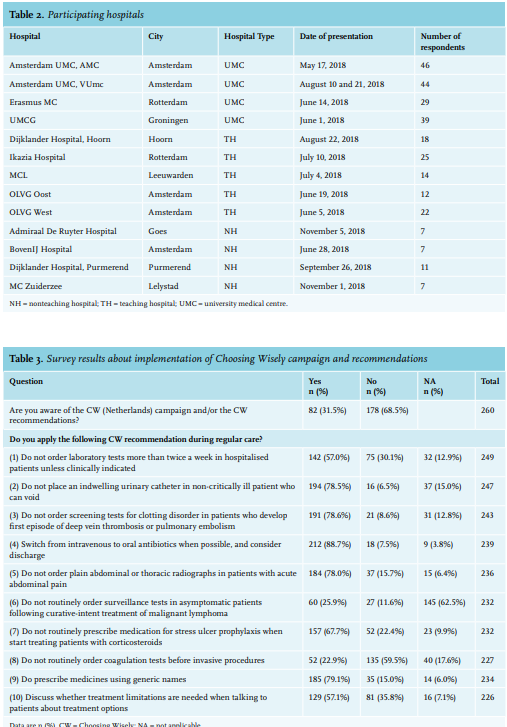
The results without the option ‘not applicable’ are found in table 4. We found that half of the Choosing Wisely recommendations were sufficiently implemented, defined as minimal 80% of the physicians who self-reported that the recommendation was part of his or her regular care.
Table 5 shows the differences between hospital types. The awareness about the Choosing Wisely campaign was the lowest (22%) in the nonteaching hospitals in comparison with 37% in UMCs. Most results of the reported implementation of the Choosing Wisely recommendations were similar between hospital types. However, we found differences in four recommendations, indicating a better reported practice in nonteaching hospitals of recommendations 2 ‘Do not place an indwelling urinary catheter in non-critically ill patient who can void’; 6 ‘Do not routinely order surveillance tests in asymptomatic patients following curative-intent treatment of malignant lymphoma’; and 8 ‘Do not routinely order coagulation tests before invasive procedures’. Further, the implementation of recommendation 10 ‘Discuss whether treatment limitations are needed when talking to patients about treatment options’ was better in teaching hospitals compared to the other hospitals.
DISCUSSION
Four years after the introduction of Choosing Wisely Netherlands campaign, only 32% of physicians and residents of the departments of internal medicine were aware of this campaign. In addition, this was even lower in nonteaching hospitals (25%). Nevertheless, half of the Choosing Wisely recommendations (numbers 2 to 5, and 9) are implemented in clinical practice. The other recommendations (1, 6 to 8, and 10) are not or insufficiently implemented in clinical practice.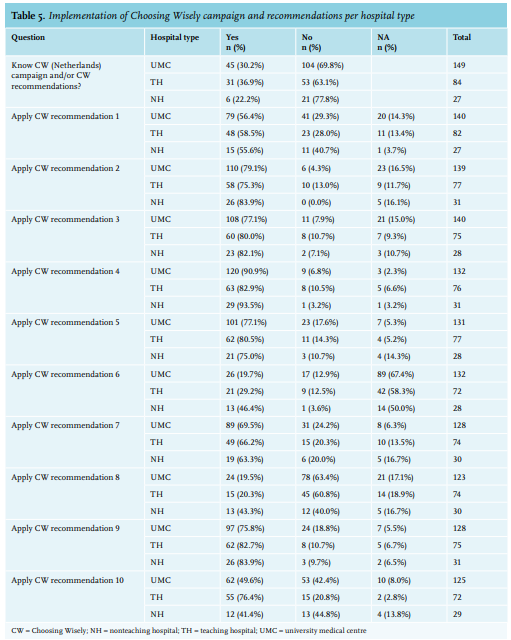
The initial goal of Choosing Wisely was to raise awareness about overuse. However, this first step did not receive enough attention in the Netherlands. One explanation is that Choosing Wisely or the concept of overuse is not implemented in medical schools and residency programs, and thus does not reach medical students and residents. However, from 2016 to 2018, a project entitled ‘Bewustzijnsproject’ (‘Awareness project’) was implemented to increase awareness among residents for high-value cost-conscious care. Next, the Choosing Wisely recommendations were published and communicated explicitly by the medical specialist societies without public and physician awareness campaigns, including for example, educational sessions, digital education materials, or social media attention.
The international spread of Choosing Wisely is promising and shows acceptance of the campaign. However, effectiveness has not been demonstrated in outcomes of quality and safety that are relevant to clinicians and patients.6 A critical step is to raise awareness of unnecessary care and harm and waste, which results in a change of attitudes and behaviours from ‘more is better’ to ‘more is NOT always better’.4 However, after four years, only one-third of clinicians were aware of the Choosing Wisely campaign in the Netherlands. This seems similar to the United States, where approximately 20% of clinicians knew about the campaign after two years;9 overall awareness among primary care physicians was higher four years after the start of the campaign at 40%.10 Interestingly, in that survey, the authors found a relationship between awareness of the campaign and the report of fewer unnecessary tests or procedures in the past year. In contrast, we found no relation between awareness and the reported implementation of the recommendation. Choosing Wisely recommendation 1 ‘Do not order laboratory tests more than twice a week in hospitalized patients unless clinically indicated’ and 6 ‘Do not routinely order surveillance tests in asymptomatic patients following curative-intent treatment of malignant lymphoma’ were followed by 65-70% of the respondents. This can be due to another national program, ‘To Do or Not to Do?’, which was introduced during the same time in the Netherlands to reduce unnecessary care.11 From this program, two projects aimed to improve the same aspects as the Choosing Wisely recommendations 1 and 6. First, a multifaceted intervention reduced unnecessary laboratory tests by 11%,12 amongst others, by a nationwide approach, during which, a toolkit in Dutch was developed to provide specific tools for healthcare workers focused on reducing unnecessary laboratory tests in hospitals.13 A remarkable observation was that 60% of the internal medicine physicians and residents stated that recommendation 6 was not applicable for their clinical practices. One explanation is that the follow-up of patients treated for malignant lymphoma is explicitly performed by physicians in haematology departments. Since our results include all subspecialties in internal medicine, we do not know the implementation of this recommendation in the haematology departments. However, routine surveillance testing in asymptomatic patients leads to unnecessary radiation, possible false-positive outcomes, unnecessary anxiety, and psychosocial issues for patients, as well as accumulated costs.14 Since CT scans are frequently routinely ordered and have a substantial false-positive rate, the improvement potential in quality of care and costs remain important.
More than 90% of respondents stated that they followed Choosing Wisely recommendation 2 ‘Do not place an indwelling urinary catheter in non-critically ill patient who can void’. However, this was a substantial problem in a recent quality improvement project in seven hospitals in the Netherlands, where inappropriate use of urinary catheters occurred in 32% of 324 patients.15 For this project, the program ‘To Do or Not to Do?’ also developed a toolkit for further implementation in the Netherlands.16
The reported implementation of Choosing Wisely recommendation 4 ‘Switch from intravenous to oral antibiotics when possible and consider discharge‘ was very good. This could be due to the introduction of the antimicrobial stewardships (A) teams, which is successful probably due to obligation and surveillance by the Health and Youth Care Inspectorate (Inspectie Gezondheid en Jeugd) of the Netherlands. Furthermore, the is a growing awareness from the surgery departments for recommendation 5 ‘Do not order plain abdominal or thoracic radiographs in patients with acute abdominal pain’. Therefore, it is clear to healthcare workers that there is no added value of a plain abdominal X-ray.17 Our results showed that there is also consensus in clinical practice regarding recommendation 3 ‘Do not order screening tests for clotting disorder in patients who develop first episode of deep vein thrombosis or pulmonary embolism’, since screening tests for clotting disorders have no treatment implications.
We found a reasonable implementation of recommendation 7 ‘Do not routinely prescribe medication for stress ulcer prophylaxis when start treating patients with corticosteroids’. However, during discussion of the presentations, it appears that for this recommendation, the internal medicine physicians were dependent on the pharmacy. In several hospitals, respondents stated that the pharmacists regularly advised and offered proton-pump inhibitors (PPIs) to patients. Since low-dose PPIs are sold over-the-counter, patients do not need a prescription in the Netherlands. The actual implementation in clinical practice for patients is therefore unclear. In addition, recommendation 9 ‘Do prescribe medicines using generic names’ is generally incorporated into the electronic prescription systems in the Netherlands. Since not all medicines have a generic name, a complete prescription in generic names is not possible.
The worst implemented recommendation was number 8 ‘Do not routinely order coagulation tests before invasive procedures’. In contrast to other recommendations, internal medicine physicians are dependent on radiologists for the implementation. In practice, a substantial part of the invasive procedures was performed by radiologists. However, they regularly demand a coagulation test (INR) before procedures. Therefore, the implementation of recommendation 8 should be multidisciplinary, for example, in collaboration with the Radiological Society of the Netherlands (NVvR).
The final recommendation 10 ‘Discuss whether treatment limitations are needed when talking to patients about treatment options’ was followed in 61% of respondents, mostly in teaching hospitals. In UMCs and nonteaching hospitals, only 50% followed this recommendation. During discussion of the presentation, most physicians declared that they consciously did not discuss possible treatment limitations in certain patient groups. For example, in the outpatient clinic, physicians did not discuss this with young patients without comorbidities and who had a short follow-up. Moreover, it is unclear, even among physicians, what the exact content of patient discussions should be, with respect to possible treatment limitations. If possible, the discussion should be held in an elective setting with the general practitioner, or with the treating physician in an outpatient setting.18 In addition, the best way to discuss treatment limitations is unclear. It seems better to ask for any objections to certain procedures, for example, by asking “Are there any treatments or procedures that you do not want to receive?” instead of “I have one more routine question that I should ask. Do you wish to be resuscitated if your heart stops or you stop breathing?”.19
The strength of this survey is the high response rate of 85% of the attendees to all questions and the multicentre design with an active assessment of the implementation of the Choosing Wisely campaign and recommendation in the Netherlands. The results should therefore be generalisable for all hospitals in the Netherlands, yet the results of this survey should be interpreted considering the limitations. The main limitation is that the results were based on self-assessment of internal medicine physicians and residents, because in general, healthcare workers overestimate themselves. Although they reported all answers anonymously, they could have reported more socially-acceptable answers. Another limitation is that the respondents only represented a part of our target populations, since we only included participants who were present during the survey day. Although our in-person survey was during a regular meeting (mostly after the morning handover), this could still introduce selection bias. Further, we could not distinguish physicians from residents, because participating in the active survey was completely anonymous and thus, did not collect any data about the respondents themselves.
CONCLUSION
In conclusion, after four years only one-third of internal medicine physicians and residents were aware of Choosing Wisely Netherlands campaign. Nevertheless, half of the Choosing Wisely recommendations were sufficiently implemented in clinical practice. There is room for improvement of the other recommendations, mainly in the recommendations that require a multidisciplinary approach.
ACKNOWLEDGEMENTS
We thank all physicians and residents from the participating hospitals for their participation and interaction during the presentations.
Conflict of interest statements
We declare no conflicts of interest.
Funding
This project was started in collaboration with the Netherlands Association of Internal Medicine (NIV) and is funded by the national board of medical specialists (Stichting Kwaliteitsgelden Medisch Specialisten). The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
*Supplementary appendix is available from the authors upon request.
REFERENCES