KEYWORDS
Cryoglobulinaemic vasculitis, direct-acting antivirals, hepatitis C virus, immunosuppression
INTRODUCTION
Mixed cryoglobulins, circulating immune complexes consisting of polyclonal IgG and monoclonal or polyclonal IgM with rheumatoid factor activity, are detected in the circulation in up to 60% of patients with chronic hepatitis C virus (HCV) infection.1 Symptomatic cryoglobulinaemic vasculitis of small and medium vessels is observed in approximately 10% of patients with HCV.2 HCV-associated cryoglobulinaemic vasculitis accounts for more than 90% of cryoglobulinaemic vasculitis worldwide.1,3 In the Netherlands however, the prevalence of HCV is less than 0.1% and HCV-related cryoglobulinaemic vasculitis is extremely rare.4 In 754 consecutive patients presenting in the southeast of the Netherlands with cryoglobulinaemia, HCV was found in less than 2% (Aendekerk et al., in preparation). Mixed cryoglobulinaemia can be considered as a low-grade, indolent lymphoproliferative disorder at risk for evolution into non-Hodgkin’s lymphoma (NHL).5,6 The clinical spectrum of cryoglobulinaemic vasculitis is variable and ranges from myalgia, arthralgia and arthritis, skin lesions (purpura), to peripheral neuropathy and renal damage.6,7 We present a patient with cryoglobulinaemic vasculitis due to an HCV infection and discuss the treatment options and prognosis.
CASE STUDY
A 59-year-old male from Azerbaijan with an unremarkable medical history was referred to our Department of Immunology after a 2-month history of fever, fatigue, polyarthritis, myalgia and muscle weakness, abdominal pain, polyneuropathy, and intermittent skin lesions. In the referring hospital, repeated blood cultures and infectious serology remained negative, including HCV. Antinuclear antibodies (ANA) and antineutrophil cytoplasmic antibody (ANCA) were negative. A total body CT scan and bone marrow examination ruled out lymphoma. The electromyography was inconclusive. The patient was referred under the suspicion of a systemic autoinflammatory or autoimmune disease, such as Behcet’s disease. The kidney involvement (dysmorphic erythrocytes, low grade proteinuria, serum creatinine 113 µmol/l) however, suggested small vessel vasculitis or immune complex-mediated disease. Regretfully the patient refused kidney biopsy. The skin showed purpura at different stages. A CT angiography showed no signs of large or medium vessel vasculitis nor occlusion of abdominal vessels. Lab results showed a mixed cryoglobulinaemia (type II with a monoclonal IgM 0.30 g/l and polyclonal IgG 0.16 g/l), a strongly positive IgM rheumatoid factor (386 IU/ml), and classical complement activation (16%) (table 1). Due to the debilitating nature of his symptoms and the clinical diagnosis of cryoglobulinaemic vasculitis with presumed kidney involvement and vasculitis of the vasa nervorum, prednisolone (1 mg/kg), mycophenolate mofetil, and plasma exchange was started, followed by rituximab, according to local guidelines. PCR showed an HCV infection genotype 3a with a viral load (VL) of 400,000 copies/ml. Liver function tests were normal. A FibroScan showed a score F0-F1 (6.8 kPa) and an echography showed liver steatosis but no signs of cirrhosis or portal hypertension. Upon improvement of his clinical symptoms, the patient was discharged, the mycophenolate mofetil stopped, and a combination of direct-acting antivirals (DAA) was started according to national guidelines, predominantly based on the European Association for the Study of the Liver (EASL) guidelines;8,9 a pan-genotype HCV NS5A inhibitor (daclatasvir) and a pan-genotype HCV NS5B inhibitor (sofosbuvir) for a duration of 12 weeks were given. 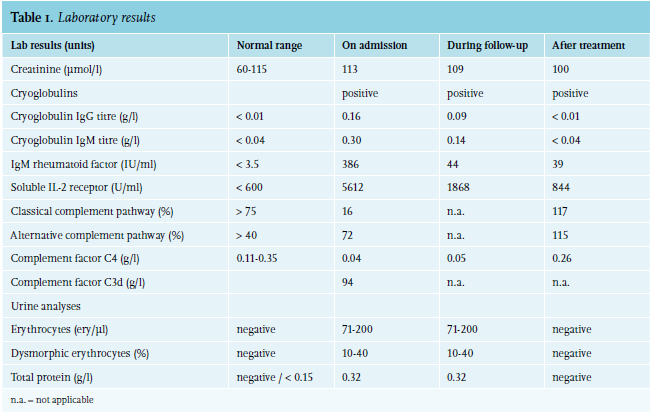
During out-patient follow-up the patient admitted having forgotten to take the medication three days consecutively halfway during the treatment. However, HCV PCR analyses done at weeks 6 and 11 of treatment showed an undetectable VL. Eight weeks after end-of-treatment, the initial presenting clinical symptoms of arthritis and myalgia returned and relapse of HCV infection genotype 3a was confirmed. Presuming possible resistance to the HCV NS5A inhibitor, and pending resistance testing, the patient was started on a combination of a pan-genotype HCV NS3/4A-protease inhibitor (pibrentasvir), a pan-genotype HCV NS5A inhibitor (glecaprevir), sofosbuvir and the synthetic nucleoside-analogue ribavirin, with an intended duration of 16 weeks. The patient stopped this treatment after three days due to side effects of extreme fatigue and conjunctivitis attributed to ribavirin. Combination therapy was reintroduced without the ribavirin. This was well tolerated and the patient completed his 16 -week treatment without any interruptions.
Meanwhile, resistance testing results showed a NS5A Y93H mutation, not yet present prior to the start of treatment. He most likely developed the mutation during his first treatment, presumably due to non-compliance. The second treatment was successful and follow-up during and 26 weeks after end-of-treatment showed a sustained virological response (SVR), marked reduction of the mixed cryoglobulins titres and normalisation of complement. Urinary abnormalities resolved as well.
DISCUSSION
This case illustrates the importance of adding the determination of cryoglobulins, according to strict procedures of blood sampling and processing, to prevent false-negative results in patients with the suspicion of a small vessel vasculitis. In addition, when cryoglobulins are present, underlying hepatitis C should be examined by PCR and in rare cases, even after resolving the cryoprecipitate. Cryoglobulinaemic vasculitis due to hepatitis C in the Netherlands is rare, although the diagnosis may be missed. Important novel treatment modalities for HCV have great impact for the prognosis of these patients.
In patients with a rapid, organ-threatening or life-threatening prognosis, immediate immunosuppressive therapy, in combination with plasmapheresis is indicated regardless of the aetiology of the mixed cryoglobulinaemia followed by treatment of the underlying cause.10 In moderate to severe cases, such as our patient, glucocorticoids are often combined with immunosuppressants such as cyclophosphamide, azathioprine, or mycophenolate mofetil and in some patients, plasmapheresis is added to more rapidly remove the circulating cryoglobulins and spare the use of glucocorticoids. Glucocorticoids to control inflammatory disease activity, together with rituximab for the depletion of B cells, improve outcome in HCV-associated cryoglobulinaemic vasculitis.1,10,11 In mild cases, treating the underlying cause is sufficient to control disease activity. Prior to the era of DAA treatment only a few options to achieve an SVR in patients with HCV were available and usually followed by a high relapse rate.12 In patients with HCV-associated cryoglobulinaemic vasculitis, the goals of antiviral treatment are to achieve SVR, obtain a clinical response, and minimise the use of immunosuppressive therapy.1
In the pre-DAA period, patients with an HCV-associated cryoglobulinaemic vasculitis had a poor long-term prognosis with 5-year and 10-year survival rates of 75% and 63%, respectively. In contrast, the 5-year survival rate of HCV infection in the absence of vasculitis is 95%.13 With the introduction of DAA treatment, prognosis for HCV-infected patients has improved significantly, including for HCV-associated cryoglobulinaemic vasculitis patients. Several studies have shown high rates of clinical remission (70-90%) after DAA therapy after a median follow-up duration of up to two years.1,6,12,14 Clinical response was associated with immunologic improvement in patients with HCV-associated cryoglobulinaemic vasculitis, yet circulating cryoglobulins seem to persist in up to 20% of patients despite an SVR and clinical improvement.1,6,12,14 This suggests that long-lived plasma cells persist and survive in niches long after viral eradication. Virus eradication does not necessarily mean that the immunological memory and signalling has stopped and several patients continue to have B-lymphocyte clonal expansion after SVR.15,16 In patients with persistent mixed cryoglobulinaemia with or without cryoglobulinaemic vasculitis symptoms, follow-up evaluation is warranted and a different underlying condition should be considered, especially B-cell lymphoma.12,16
Resistance Associated Substitutions (RASs) occur naturally in HCV infections. A Y93H mutation occurs in < 10% of patients with HCV genotype 3 and corresponds with resistance for a number of HCV NS5A inhibitors including daclatasvir.17 The current EASL guidelines suggest treatment regimens that do not necessitate any resistance testing prior to first-line therapy.9 The current Dutch guidelines advise resistance testing to be done in untreated patients with HCV genotype 3 with cirrhosis, and in patients with HCV genotype 3 without cirrhosis but who have been previously treated. The reason for this strategy is the much higher cost of the alternative regimen glecaprevir/pibrentasvir compared to sofosbuvir/ velpatasvir, which can be given if there is no corresponding RAS mutation. There is no known resistance against pibrentasvir (another HCV NS5A inhibitor) due to a Y93H mutation and retrospectively, our patient could have been treated with glecaprevir/pibrentasvir for a duration of 12 weeks. In our case, we did not wait for the results of resistance testing before administering the second broader and more robust regimen due to the patient’s returning symptoms; results of resistance testing can take up a couple of weeks.
In conclusion, the introduction of direct-acting antivirals has strongly improved the clinical and immunological outcome for hepatitis C virus-associated cryoglobulinaemic vasculitis patients. Most patients can now be treated for the HCV infection alone without the need for immunosuppressive therapy. In severe cases, immunosuppressive therapy is still warranted.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES