DIAGNOSIS
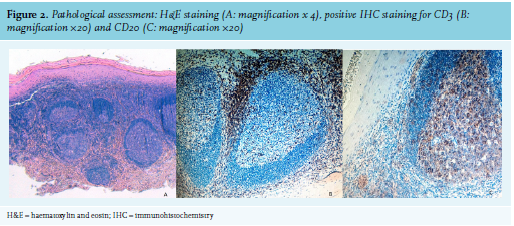
Our pathological assessment showed hyperplastic aspect of the epithelium and the subepithelial tissue contained a dense follicular lymphoid infiltrate. The interfollicular tissue contained small lymphocytes, occasional large lymphocytes, plasma cells, and a few eosinophils (Positive: CD20, CD3; Negative: Bcl2, Bcl6, CD10, Mib1) (figure 2). An incisional biopsy was repeated on the right buccal mucosa with the same pathological assessment. The specimens were analysed by a second pathologist, who confirmed the diagnosis.
To complete the diagnostic process, in agreement with the haematologist, a blood exam, an ultrasonography of the abdomen, a chest X-ray, and protein electrophoresis were performed. The exams ruled out any systemic involvement. The diagnosis of oral lymphoid hyperplasia was concluded from the joint assessment of these results, together with the previous investigations. FLH may also originate from an oral lichen planus (OLP). In fact, OLP is an autoimmune disease that extensively involves the immune system and due to the immune activation, OLP could give rise to lymphoid follicles. The patient has been followed-up for 12 months with no sign of worsening of the lesions, which remained lightly symptomatic.
Follicular lymphoid hyperplasia (FLH) of the oral cavity is a rare lymphoproliferative disorder which may be confused clinically and histologically with malignant lymphoma. The condition has been described in different regions of the body: notably skin, gastrointestinal tract, lungs, nasopharynx, larynx, and breasts. Although rare, the oral cavity may also be involved.1 The disease occurs in a wide age range, between 38 to 79-year-old patients, and is more common in women.2 Clinically, the manifestation is a firm, painless, nonulcerated, slowly growing mass or swelling on the one side of the palate. Occasionally, the lesions may be multifocal and the patients may have bilateral involvement.3 The lymphoid infiltrate may show the features of a benign reactive follicular hyperplasia, causing no difficulties in diagnosis but there is commonly an erroneous diagnosis of follicular lymphoma, with consequent staging procedures and unnecessary treatment. Oral manifestations of FLH have been reported in only approximately 30 cases, which showed the presence of swelling in particular of the hard palate. To the best of our knowledge, this is the first reported case of bilateral buccal mucosa involvement mimicking lichen planus. FLH is a rare and benign lymphoproliferative disorder, and interdisciplinary efforts are crucial to avoid diagnostic time delay.
REFERENCES