KEYWORDS
Adherence, device-based therapy, hypertension, resistant hypertension
CASE PRESENTATION TO INTRODUCE THE TOPIC
A 55-year-old female with a history of Graves’ disease and thyroidectomy was referred due to severe hypertension from which she suffered for over 20 years. The patient reported that several antihypertensive drugs were replaced due to side effects, including perindopril, which was discontinued due to a dry cough and doxazosin, which was stopped due to palpitations. Despite a regimen of valsartan 320 mg once a day (qd), hydrochlorothiazide 25 mg qd, amlodipine 10 mg qd and metoprolol 100 mg qd, her blood pressure (BP) remained uncontrolled. She reported to be fully adherent to all medications. In addition to antihypertensive drugs, she was taking levothyroxine 100 microgram qd. Most of the time when she was late from work, she ordered ready-meals (3-4 times a week). Physical and laboratory examination including 24 hr urine sodium measurement and thyroid function tests revealed, in addition to a severely elevated BP (200/120 mmHg, heart rate 75 beats/min) and a high-salt intake of 170 mmol/24 hrs, no further abnormal findings. Additional workup showed no relevant secondary causes of hypertension. Twenty-four-hour ambulatory blood pressure monitoring (24h ABPM) confirmed true resistant hypertension with mean daytime BP 145/98 mmHg. Her physician proposed to intensify her antihypertensive drug regimen and offered her dietary support to reduce salt intake. However, the patient was curious about a new technology that she had read about on Facebook, something with heat and nerves that could result in a better blood pressure control: would she be a candidate for this technique?
DEFINITIONS
With the recent changes in the European and American hypertension guidelines, BP targets are lower than ever.1,2 However, the 2018 European Society of Cardiology/ European Society of Hypertension (ESC/ESH) and the 2017 American College of Cardiology/American Heart Association (ACC/AHA) guidelines vary in the recommendations regarding when treatment should be initiated. The ESC/ESH guidelines recommend initiation of treatment at an office systolic BP of ≥ 140 mmHg and/ or a diastolic BP ≥ 90 mmHg, with 24h ABPM values, in general, being lower than the office BP values (diagnostic threshold for hypertension is a mean daytime ABPM ≥ 135/85 mmHg).1 The ACC/AHA guidelines advocate an even lower threshold for commencing treatment (office BP ≥ 130/80 mmHg, daytime 24h ABPM >130/80mmHg).2
These thresholds were based on multiple clinical trials and meta-analyses, showing the beneficial effects of BPlowering therapy on cardiovascular events.3-7 Regardless of the final target value, Ettehad et al. showed that every 10 mmHg reduction in systolic BP significantly reduced the risk for all major cardiovascular events by 20% and led to a significant 13% reduction in all-cause mortality.3 BP that remains uncontrolled (> 140/90 mmHg) despite the prescription of three antihypertensive drugs (with at least one diuretic) in a maximally-tolerated dose is considered ‘resistant hypertension’ (RH).8 The RH definition was initially established to identify a high-risk patient population that would benefit from more specialised care and specific diagnostic testing.9 However, the definition remains rather nonspecific and could include patients with either true or pseudo-RH. Several factors play a role in persistent uncontrolled hypertension, and therefore a stepwise approach is recommended. 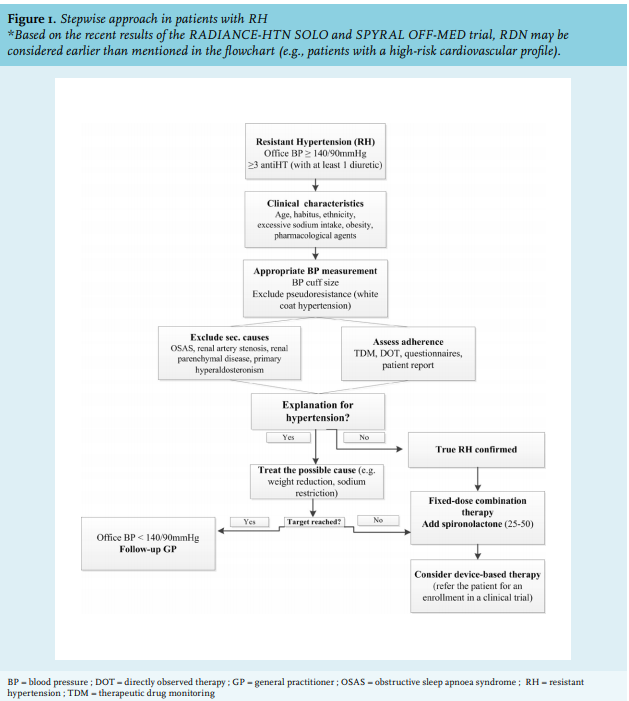
STEPWISEAPPROACH
General clinical characteristics
The American Heart Association emphasizes that RH is a multifactorial problem; individual patient characteristics include lifestyle factors, potential secondary causes of hypertension including drug-related causes, and potential pseudo-resistance should be assessed.9,10
Several patient characteristics such as older age, obesity, excessive sodium intake, diabetes, black race, female gender, high baseline systolic BP, and target organ damage (chronic kidney disease and left ventricular hypertrophy) proved to be strong predictors for uncontrolled BP.9 Lifestyle factors such as excessive sodium intake and heavy alcohol intake should be discussed and discouraged. Pimenta et al. studied the effect of dietary salt restriction on office and 24h ABPM in patients with RH,11 and demonstrated that low versus high-salt diet decreased both office BP (systolic and diastolic decrease of 22.7/9.1 mmHg, respectively) and 24h ABPM (20.7/9.6 mmHg). Additionally, the degree of BP reduction induced by salt restriction in the cohort with RH was larger than reductions observed in the normotensive cohort. These results demonstrate the importance of salt restriction in patients with RH.
A recently published randomised trial showed the effect of lifestyle change and weight management in football fans, in which the lifestyle programme helped to improve weight, waist circumference, and vitality, and significantly reduced diastolic BP at 12 months (mean difference between intervention and control group -1.2 mmHg (95% CI: -2.1 to -0.4, p = 0.004).12
Pharmacological agents that could increase BP such as the use of nonsteroidal anti-inflammatory agents, oral contraceptives, and sympathomimetic agents (cocaine), should be dissuaded.13 Furthermore, care should be taken in performing accurate BP measurements and general clues that could reveal secondary causes of hypertension should be identified during outpatient clinic follow-up.14 Additionally, non-adherence to prescribed antihypertensive drugs should be assessed.10,15
Appropriate BP measurement
Inaccurate BP measurements proved to be a frequent cause of pseudo-resistance.8 Automatic office BP measurement is recommended and BP should be measured in both arms during the first visit. As a rule of thumb, the health care provider should measure BP three times with intervals of at least one minute. The average of the last two measurements in the arm with the highest BP value should be used as a reference at follow-up.2,16 In the most optimal setting, BP should be measured unattended.17 Frequent mistakes comprise measuring BP before the patient could sit quietly for a couple of minutes and using to small BP cuffs, which will result in falsely high BP measurements.18
The gold standard, to rule out white coat and masked hypertension, is a 24h ABPM, which should be performed in all patients with suspected RH.16,19,20 Furthermore, home BP assessment proved to be a better predictor for cardiovascular morbidity than office BP.21,22 When home BP is combined with physician counselling, the adherence to antihypertensive drugs could improve, resulting in better BP control.23-25 Home BP measurement is recommended when the patient is able to measure his/ her BP by an automatic BP monitor.
Exclude secondary causes for hypertension
Secondary causes of hypertension can be found in up to 10% of cases.26 True RH should be the trigger towards more extensive workup.14 Attention should be paid to symptoms of snoring, daytime sleepiness, and morning headache, especially in overweight and obese patients in order to detect obstructive sleep apnoea which proved to be twice as common in RH compared to non-RH patients, with incidences reported to be more than 30%.8,14,27 Furthermore, other relatively common causes should be excluded based on clinical and laboratory findings such as renal parenchymal disease (e.g., especially in patients with diabetes or smokers; generalised atherosclerosis; and previous renal failure, for which, screening should be done with kidney ultrasound) and primary aldosteronism (6-23% of RH cases; clinical findings include observed muscle weakness; complaints of fatigue; constipation; polyuria and polydipsia) (figure 1). Finally, renal artery stenosis is a known secondary cause of RH present in 2-20% of RH cases and is either caused by atherosclerosis or fibromuscular dysplasia. Occurrence of flush pulmonary oedema might unravel bilateral renal artery stenosis. The importance of treatment, and in particular renal artery stenting or balloon dilatation, remains debated, but should be considered, especially in patients with rapidly decreasing kidney function or in patients with only one functional kidney.28
More uncommon causes to be ruled out include Cushing’s syndrome (< 1%), as well as hypo- as hyperthyroidism, coarctation of the aorta (< 1%) and phaeochromocytoma (< 1%).14 Of note, while helpful in lowering BP and improving patient prognosis, treatment of secondary causes does not always lead to normalisation of BP and pharmacotherapy remains necessary.29
Exclude non-adherence
One of the main causes of pseudo-RH is non-adherence, with a reported prevalence ranging from 23-66%.30 Non-adherence can mean that a patient is non-adherent to all drugs (full non-adherence) or to a limited number of drugs (partial non-adherence). As a matter of fact, non-adherence to antihypertensive drugs, as an underlying cause is the most difficult cause to treat for RH.31 A crucial step in the management of hypertension and especially in patients with RH, is the assessment of adherence to antihypertensive drugs. Assessing adherence has been recognised as the first step in improving non-adherence and clinical outcome.32 Scotti et al. showed that an enhancement of adherence from 52% to 60-80% led to a reduction in cardiovascular events from 85 to 83, and 77 events every 10,000 person-year, respectively.32
Clinicians in general tend to overestimate adherence rate.33 Several methods are available to assess adherence such as pill counts, patient self-reports, directly-observed therapy, and measurement of drug or metabolite levels.34,35 Direct methods (such as directly-observed therapy, electronic monitoring, and therapeutic drug monitoring (TDM)) are more accurate and reliable than indirect methods (such as questionnaires or pill count).30 Direct methods, however, are more expensive and more labour-intensive.30,34 In more complex cases, a combination of TDM and directlyobserved therapy might provide a better understanding and facilitate further counselling on drug adherence.36 Once non-adherence has been objectified, efforts should be made to find the underlying cause to help the patient in finding a solution.37 In a small pilot study, it appeared that using TDM to identify non-adherence, followed by counselling, led to improvement of adherence and BP regulation.38 Currently, the effect of TDM combined with counselling based on finding the underlying cause for non-adherence to improve BP regulation in pseudo-RH is being assessed in the Resistant Hypertension: Measure to Reach Targets (RHYME-RCT) (trialregister.nl; NTR6914, RHYME-RCT).
TREATMENT OPTIONS
Pharmacotherapy
The 2018 ESC/ESH guideline recommends the initiation of pharmacological treatment within the five major antihypertensive classes: angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor inhibitors (ARBs), calcium channel blockers (CCBs), diuretics, or beta-blockers, in which an overview per drug class and possible side effects can be found.16
When focusing on patients with RH, without finding a secondary cause and after confirming adherence to the prescribed antihypertensive drugs, BP targets can often still be achieved by optimising antihypertensive drug regimens (including a fixed-dose combination therapy).1,39 As a next step to an ACE inhibitor or an ARB (a CCB and a diuretic), the addition of spironolactone has shown to be effective in lowering BP.40 In the PATHWAY-2 study (Prevention and Treatment of Hypertension with Algorithm-based therapY-2), the BP lowering effect of spironolactone (25-50 mg) was greater than doxazosin and bisoprolol. New antihypertensive drugs, which are being studied, primarily target the renin-angiotensin-aldosterone system (RAAS), such as aldosterone synthase inhibitors or non-steroidal mineralocorticoid receptor blockers, with the aim to reduce the anti-androgenic side effects.41 Although vaccines targeting RAAS components were considered treatment options to avoid adherence issues, pharmacokinetic and pharmacodynamics issues hampered further development.42 A promising treatment option to date, is the combination of angiotensin II receptor blockade and neprilysin inhibitor (ARNI), currently registered for heart failure.41,43 ARNIs showed significantly greater reductions in BP as compared with an ARB alone and have been proven safe and well-tolerated.
Device-based therapy
Despite currently available interventions targeting lifestyle and pharmacotherapy including drug adherence, it is often not possible to reach the target BP. A recent study by Patel et al. reported that when causes for pseudo-resistance including non-adherence were excluded, 15% of patients with RH may be eligible for device-based therapies for hypertension. Moreover, recent studies showed that patients would prefer device-based therapy that may diminish the need for more antihypertensive drugs. Hutchins et al. showed that approximately one out of three respondents would be willing to trade two years of their life to avoid taking drugs. Additionally, respondents were willing to pay an average of $1445 to avoid daily medication.44 At present, several device-based therapies have been studied to control BP as an alternative or add-on therapy in patients with RH, by primarily targeting the autonomic nervous system.45
Renal denervation
The most studied device-based therapy to date is renal sympathetic denervation (RDN). The percutaneous treatment targets renal sympathetic nerves at the renal artery level and demonstrated reduction of sympathetic overactivity.46 Although several promising trials have been published, the treatment faced a significant decline in enthusiasm following the neutral results of the first sham-controlled RDN trial, the Symplicity HTN-3 trial (Renal Denervation in Patients With Uncontrolled Hypertension) in 2014.47-49 Dissecting the trial design identified several factors that could potentially have led to the failure of the trial of meeting its primary endpoint.50 As such, inadequate screening, frequent changes in antihypertensive regimens and the use of a first-generation RDN device along with a lack of operator experience were suggested to be responsible.51-53 Subsequently, three proof-of-principle studies with more advanced trial designs, proved the overall efficacy and safety of the technique.54-57 Both RDN techniques used in these studies seem efficacious in achieving a significant drop in blood pressure of approximately 6 mmHg as compared to a sham comparator arm at 2-3 months. The body of evidence supporting the efficacy of the treatment in patients with RH is steadily increasing. Given the positive data available thus far, referring patients with true RH to specialised centres participating in dedicated RDN trials should be strongly encouraged.
Several studies on BP efficacy and safety of renal sympathetic denervation, with strict entry criteria, are ongoing (RADIANCE II Pivotal; TRIO; NCT03614260; NCT02649426; REQUIRE study NCT02918305).
Barostim Neo system
Carotid baroreflex activation therapy is a relatively new surgical implantable device which stimulates the carotid baroreceptors and therefore down-regulates the sympathetic outflow with an increase in parasympathetic tone.58,59 The first sham-controlled studies in patients receiving bilateral implants showed significant BP reduction with a clear on/off phenomenon.58,60 A recently published study on the safety profile and efficacy of a second generation of the device, the Barostim Neo, showed that side effects such as syncope, hypertensive crisis, and arrhythmias occurred in 28% of patients. A significant BP drop was seen at six months in patients treated with Barostim Neo (from a mean of 169 ± 27 to 148 ± 29 mmHg, p < 0.001) and one year (a further decrease to 145 ± 24 mmHg as compared with baseline, p < 0.001) follow-up with a significant decrease in prescribed antihypertensive drugs.59 However, due to current lack of randomised controlled trials, the side effects, the high costs, and the need for frequent battery replacement, there was a quest for alternative methods to stimulate the baroreflex and lower BP.61,62
Mobius HD system
Carotid baroreceptor amplification therapy, the Mobius HD system, is an endovascular carotid implant. Its mechanism of action is based on passive activation of the baroreceptor by irreversibly changing the carotid sinus shape, resulting in pulsatile wall stretch and a linear increase in firing rate when BP increases.62 The latter phenomenon suppresses the sympathetic outflow and consequently decreases BP. The CALM-FIM study (Controlling and Lowering Blood Pressure with the MObiusHD) showed that the Mobius HD device significantly reduced BP (by 21/12 mmHg at 6 months, p < 0.001)., however this was a non-randomised, open-label study.63 Two patients developed neurological symptoms after implantation. CALM-2 study is now enrolling to further study the efficacy and safety (ClinicalTrials.gov NTC03179800).
Other non-pharmacological interventions
A number of non-pharmacological therapies are in the pipeline at different stages of development, such as the alcohol-mediated perivascular renal denervation with the Peregrine SystemTM (Ablative Solutions)64 and the ROX AV coupler (ROX Medical) which creates an arteriovenous (AV) anastomosis between the external iliac artery and vein to reduce vascular resistance and the effective arterial volume, that could immediately result in significant reductions of BP.65 Several studies are ongoing to evaluate their safety and efficacy further (Peregrine system, TARGET BP OFF-MED trial, NCT03503773); ROX coupler (CONTROL HTN-2 NCT02895386).
In general, based on the recent 2018 ESC/ESH guidelines, device-based therapy for hypertension is not recommended for the routine treatment of hypertension, unless performed within the context of a clinical (randomised) trial. The results of current ongoing larger clinical trials will provide more details on the safety and efficacy of the technology.1
Back to the case
Despite a substantial decrease in urine sodium excretion from 170 to 130 mmol/24h, BP remained uncontrolled. Further work-up of our patient included drug adherence testing using TDM in which we measured the drug levels by venous sampling. After confirming full adherence, spironolactone was added to her drug regimen resulting in daytime average 24h ABPM of 141/90 mmHg (mean office BP 165/100 mmHg). Due to a lack of response to the therapy above, the patient was enrolled in a double-blind, randomised controlled trial to assess the efficacy and safety of RDN in patients with RH.
CONCLUSION
The management of RH should contain advise on lifestyle modifications including the reduction of sodium intake, and accurate BP measurement, preferably by 24h ABPM, to rule out pseudo-RH. Additionally, assessment for secondary causes of hypertension should be considered and non-adherence to prescribed antihypertensive drugs should be ruled out. To note, adding a mineralocorticoid receptor blocker to the existing antihypertensive regimen could lead to an additional BP drop, also in essential hypertension. New drug- and device-based treatment options have been studied extensively over the past years, with promising results in the general hypertensive population. More evidence is warranted in order to determine the clinical relevance and cost-effectiveness of device-based therapies as compared with existing pharmacological treatment options.
DISCLOSURES
Joost Daemen received institutional research support from Medtronic, PulseCath, Abbott Vascular, Acist Medical, and Pie Medical, as well as consultancy and lecture fees from Acist Medical, Medtronic, PulseCath, and ReCor Medical. For the remaining authors no conflicts of interest were declared.
REFERENCES