CASE REPORT
A 59-year-old female was admitted to the Intensive Care Unit (ICU) in respiratory distress. She was admitted to the general ward three days before with misery and fatigue, and became rapidly dyspnoeic at day three. Influenza A virus testing was positive, despite her annual preventive influenza vaccination.
Medical history revealed proven systemic lupus erythematosus (SLE), nephritis with slow progressive kidney failure, living related kidney transplant in 1995 resulting in chronic allograft nephropathy, living unrelated kidney transplant in 2015, mild mitral valve and moderate aortic valve insufficiency with left ventricular hypertrophy, and interstitial lung disease since 2018. Known prescribed medications were omeprazole, prednisolone, tacrolimus, everolimus, irbesartan and montelukast.
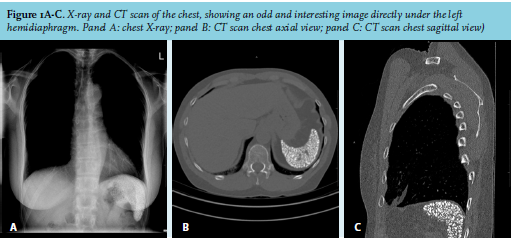
Physical examination showed a very tachypnoeic patient with use of accessory respiratory muscles, respiratory rate 40/minute, SatO2 68% with 15 litres/minute oxygen on a non-rebreather-mask, blood pressure of 190/105 mmHg, heart rate of 155/minute and tympanic temperature of 37.4°C. Blood gas analysis showed a non-compensated metabolic acidosis (pH 7.27, pCO2 6.1 kPa, HCO3- 21.0 mmol/l, base excess -5.9 mmol/l) and hypoxia (pO2 8.1 kPa, SatO2 88%). We started respiratory support with non-invasive ventilation. Laboratory results showed no leukocytosis, elevated C-reactive protein of 116 mg/l, lactate of 3.0 mmol/l and n-terminal prohormone of brain natriuretic peptide (NT-proBNP) of 34847 pg/mL. Chest X-ray showed extensive bilateral infiltration of lower lung fields and pleural effusion. CT scan of the chest was performed to exclude pulmonary emboli, which were not present. We suspected cardiogenic pulmonary oedema and started treatment with furosemide, nitroglycerine, milrinone, and hydrocortisone stress scheme. Moreover, we treated her with oseltamivir and cefotaxime, later on switched to ceftazidime because of a sputum culture showing Pseudomonas. With this treatment, our patient recovered rapidly, and we waived further diagnostics (on for instance Aspergillosis). While reviewing the X-ray and CT scan (figure 1), we noticed an odd and interesting image directly under the left hemidiaphragm.
WHAT IS YOUR DIAGNOSIS?
See page 164 for the answer to this photo quiz.