DIAGNOSIS
The pathologists concluded an atypical population of T cells suspicious for mycosis fungoides or Sezary-syndrome (cutaneous T-cell lymphoma). To confirm this diagnosis, blood samples were sent to a reference centre for immunophenotyping. However, this showed a more reactive T-cell population with CD8+ cells with an effector phenotype, activated HLA-DR (Human Leukocyte Antigen - DR isotype) and normal expression of CD2,3,4,5,7 and 8; only a small number of CD8+ cells expressed CD30. Hence, the diagnosis of cutaneous T-cell lymphoma was not confirmed. Treatment of this T-cell lymphoma was postponed because of his critical illness. During his stay in the ICU, his skin condition somewhat improved after systemic antibiotics (meropenem and ciprofloxacin) were started for a pulmonary infection. Anti-retroviral therapy with dolutegravir, emtricitabine and tenofovir was initiated almost directly after admission but did not affect his skin lesions. Two weeks after the start of systemic antibiotics, steroid cream (class 4) was advised by the dermatologist and applied twice daily for treatment of his T-cell lymphoma. The patient experienced less itching, the crusted skin lesions disappeared slowly, and the non-crusted skin became darker. However, the skin lesions did not disappear completely, still affecting the face, armpits, elbows, legs, and abdomen.
Approximately two months after ICU admission of our patient, a nurse was diagnosed with scabies by his general practitioner. This fact alarmed the staff that the patient could have unrecognized crusted or “Norvegian scabies”. A skin-scraping and microscopy examination was then performed on the patient, which identified countless mites and mites eggs (figures 2A and B) and thus confirmed the diagnosis of crusted scabies. Treatment consisted of ivermectin orally on days 1, 2, 8, 9, 15, 22, and 29. Permetrin 50 mg/g cream was applied on the skin daily. After a few days, his crusted skin lesions completely disappeared. With the diagnosis of scabies in mind, the histopathology was revised and sent out for second opinion; in addition to scabies, there was still a strong suspicion of a cutaneous T-cell lymphoma (CD8-positive mycosis fungoides). Unfortunately, the patient died due to other complications before receiving treatment for this suspected T-cell lymphoma.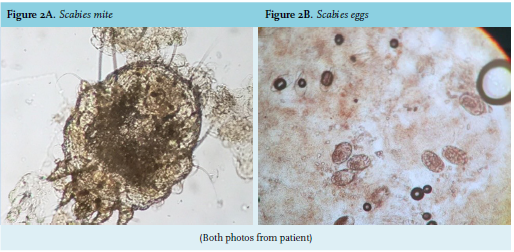
Crusted or disseminated scabies is a diagnosis that is frequently missed and can lead to hospital outbreaks.1 It can occur in patients that have compromised cellular immunity, e.g. HIV-infection, human T-cell lymphotropic virus type 1 (HTLV-1) infection, lymphoma, and Hansen’ disease (leprosy). A high number of scabies mites are present, and it is therefore very contagious. In our hospital, the Outbreak Management Team identified approximately 400 health workers who had some form of contact with the patient. They all received, according to Dutch national guidelines a prophylactic treatment of a single dose of ivermectin. Four individuals who nursed the patient intensively in the ICU department were diagnosed with scabies. The high-level standard hygienic measures (strict hand hygiene, wearing gloves and medical gowns at all patient-related activities) probably explains the low number of health workers infected, compared to other previous hospital outbreaks.2 Retrospectively, the skin lesions significantly improved and the skin was less discoloured 2-3 days after starting meropenem and ciprofloxacin. There are no similar reports published, except for a 7-day course of co-trimoxazol which was not effective against scabies.3 The most plausible explanation in our opinion, is that these systemic antibiotics treated unrecognised secondary bacterial infections of the skin (e.g. cellulitis), which are common in crusted scabies but more difficult to diagnose in dark skin. The effects of topical corticosteroids are known to diminish hyperkeratotic skin lesions and reduce the pruritus, and is therefore often described as “scabies incognito”. It is known that a skin biopsy in crusted scabies can mimic other cutaneous diseases, such as Langerhans cell histiocytosis.4 The revised histopathology showed a strong suspicion of a T-cell lymphoma; however, several diseases can mimic CD8+ T-cell lymphoproliferative disorders.5 This emphasizes the indispensability of clinicalpathological correlation in pathology requests.
This case illustrates that we, as physicians, are prone to several forms of cognitive bias. We relied too heavily on the presumptive diagnosis of the pathologist and we failed to make a proper list of differential diagnosis. This is a form of “anchoring”, a cognitive bias when a person relies too heavily on the initial piece of information he/she receives when making a diagnosis. Here, anchoring resulted in premature closure in the diagnostic process and delay in appropriate treatment.
REFERENCES