Dear editor,
Aplastic anaemia in pregnancy is a serious condition for both the mother and child. In the 20th century, maternal morbidity was reported to be 20-60% and termination of pregnancy at early gestation was recommended in pregnant women with aplastic anaemia.1-4 However, according to recent case series, current maternal and foetal outcome seem to be much better.5-8 Bone marrow transplantation is the treatment of choice in young patients with aplastic anaemia, but this is contra-indicated during pregnancy due to toxicity for the foetus (table 1).9 Although guidelines advise treatment with cyclosporine in pregnant woman, only a few transfusion-dependent women with aplastic anaemia received cyclosporine in addition to supportive care.3,10-12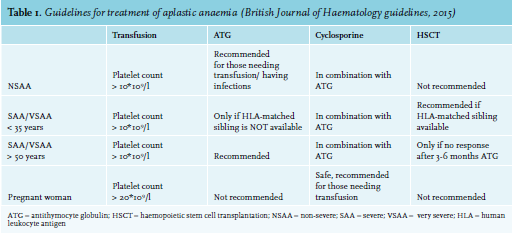
We diagnosed a 38-year-old second gravida with pancytopenia at week 12 of gestation (haemoglobin level 6.12 g/dl, (ref: 12-16), white blood cell count 2.3*109/l (ref: 4-10), neutrophilic count 0.5*109/l (ref: 1.5-3.5), platelet count 9*109/l (ref: 150-400), LDH within normal range). In retrospect, she had a platelet count of 57*109/l 6 months before presentation as determined by a general practitioner. Bone marrow biopsy revealed aplastic anaemia with a reduced marrow cellularity of 30-40%, without dysplastic signs. Direct antiglobulin test was negative and only a small glucose phosphate isomerase (GPI)-deficient population was found. Anamnesis and virology testing did not indicate another cause for this severe aplastic anaemia other than exacerbation of idiopathic aplastic anaemia by pregnancy. After consultation with a multi-disciplinary team and extensive counselling of the patient, she decided to continue her pregnancy. Initially, she was treated with supportive therapy to keep her haemoglobin level above 10 g/dL and platelet count above 20*109/l, and she was administered trimethoprim/sulfametrol as a prophylaxis. Because of a high transfusion need, treatment with cyclosporine was started in week 13 of gestation. After four weeks, transfusion necessity for platelets decreased from twice a week to once a week and her neutrophil count improved. There was no obvious decrease of erythrocyte transfusion need. She delivered a healthy boy at week 37. Cyclosporine was continued for six months and although pancytopenia persisted, no more transfusions were needed. After cessation of cyclosporine, only mild pancytopenia remained and no further treatment was required.
Based on our experience and review of literature, we do not recommend standard termination of pregnancy at early gestation, although we advise extensive investigation to exclude underlying causes of anaemia, and treatment with supportive care and cyclosporine when necessary.
ACKNOWLEDGEMENT
The authors report no conflicts of interest.
REFERENCES