To the Editor,
Medical care in Dutch nursing homes is provided by elderly care physicians (ECPs). The three-year specialist training program for ECPs consists of three training periods in an educational nursing home, three internships, and a theoretical course lasting 100-130 days. Evidence-based medicine (EBM) is taught during the theoretical course. Currently, the EBM training in the ECP program at Leiden University Medical Centre comprises: 1) several lectures on the basics of research and critical reading, 2) the writing of three critically appraised topics (CATs)1,2 with questions initiated by the trainees themselves, and 3) participation in a group of ECP trainees to analyse an existing dataset and present the results to their peers. Teaching EBM is essential to create lifelong learners who can critically appraise information and assess the applicability of this information for the individual patient.3 This applies, in particular, to elderly care medicine, due to the underrepresentation of frail elderly persons and nursing home residents in medical research. Although classroom teaching of EBM improves knowledge, clinically integrated teaching improves not only knowledge but also related skills, attitude and behaviour.4 Compared with traditional teaching, a blended learning approach is more effective in improving the attitude towards EBM and results in a higher self-reported use of EBM in clinical practice.5 The EBM training is regularly evaluated and updated to maintain a state-of-the-art program. Our latest innovation is the integration of a prospective cohort study assessing the relation between caffeine and behavioural symptoms, and the EBM training program.
Of all patients admitted to Dutch nursing homes, ≥ 50% are diagnosed with cognitive disorders or dementia. In patients with dementia behavioural symptoms are often the main reason for nursing home admission, often due to the heavy burden placed on the caregivers,6 resulting in a high demand for care. In addition, behavioural symptoms lower the patient’s quality of life.7 Behavioural symptoms are present in ≥ 80% of patients with dementia in a nursing home.8,9 In patients with dementia the aetiology of behavioural symptoms is complex and thought to be multifactorial.10 To manage these symptoms, national guidelines recommend a detailed analysis of the patient, including contributing physical, psychological, social and environmental factors.10 Despite the fact that many pharmacological11,12 and psychosocial interventions have been studied,13,14 no standardised solution is available and all interventions targeting behavioural symptoms must be tailored.13,15
The Dutch national guideline on behavioural symptoms in patients with dementia mentions caffeine consumption as a possible contributing factor.10 However, this conclusion is not based on research in patients with dementia or in patients in nursing homes. To date, the only study available on caffeine and behavioural symptoms in older patients with dementia in nursing homes is a small observational study showing an association with apathy, and an inverse association with aberrant motor behaviour and caffeine consumption.16 On the other hand, the effect of caffeine on behaviour in adults has been widely investigated but the effects differ between individuals, and people normally adjust their consumption of caffeine based on their own experienced (non-)beneficial side effects.17,18 However, institutionalisation and cognitive disorders tend to impair the ability to self-adjust caffeine consumption. Based on research among healthy adults, both a positive and a negative influence of caffeine consumption on behavioural symptoms can be expected in older patients with dementia in nursing homes. Additional research in larger study populations is needed to gain more insight into the effects of caffeine consumption in older people.
The purpose of the BeCaf study is twofold. The primary aim is to assess the relation between caffeine and behavioural symptoms (e.g. apathy and agitation) in older patients in nursing homes and to assess factors contributing to this relation. The second aim is to create an educational innovation of EBM training for ECPs, leading to a new EBM curriculum which stimulates trainees’ interest in research and integrates research into clinical practice.
In the new EBM program several improvements will be made. First, the basics of research and critical reading will be taught using classroom activities (lectures and part-task practice) and online learning. Second, each trainee will participate in a complete medical study and this study will be embedded in their clinical practice. Writing three critically appraised topics (CATs) remains part of the program. The result is a complete EBM curriculum with research skills introduced in manageable parts, a blended learning approach, and integration of the EBM program in clinical practice.
The BeCaf study is a prospective multicentre cohort study, embedded in the ECP training program during the theoretical course. All trainees are asked to collect data from their own patients, thereby making every educational nursing home a possible centre of study. As the population in nursing homes is highly diverse, a more homogeneous study population was desired, but without limiting the study population to a specific ward or unit; this would allow every trainee, irrespective of their training period, to participate. Therefore, to create a more homogeneous study population, a ‘ward transcending’ factor was chosen, i.e. diabetes mellitus type 1 and 2. In European nursing homes, 21.8% of patients are diagnosed with diabetes mellitus.19 A trainee on a full-time contract is supposed to provide medical care for 50-80 patients. For this study, trainees were asked to include all patients under their care who had a diagnosis of diabetes (type 1 or 2); no other inclusion criteria were applied. All participants and educational nursing homes received adequate oral and written information about the study. The study protocol was approved by the Medical Ethics Committee of the Leiden University Medical Centre.
Trainees identify all patients under their care who have diabetes. Data of these patients are collected by the trainees, based on medical records and interviews with the nursing staff. The data are gathered according to the Somatic, Activities of daily living, Social, Psychological and Communication (SASPC) system, a problem-oriented system for multidisciplinary care,31 which creates a complete overview of the patient. Only reliable and validated instruments are used to collect the data. None of the instruments burdens or bothers the patient in any way. The instruments used are described in table 1. After assessment, the anonymised data are entered in a secure online platform (NetQ Healthcare) by the trainees. If any data are missing, the senior researcher contacts the trainee to complete the data. After trainees have formulated a research question, they are only provided with data required to answer their question.
Only a few studies have examined the effects of caffeine among older patients. To our knowledge, our study will potentially include the largest group of older patients with data on their behaviour, cognition and caffeine consumption.
Although EBM is considered essential in practising medicine, obstacles in teaching EBM include: insufficient interest and/or limited time of trainees and faculty, lack of trainee research skills, absence of a research curriculum, and inadequate funding.32 As this study is embedded in the EBM training program, the above obstacles related to teaching EBM have been tackled. Integration with clinical practice is beneficial for the trainees4,33 and might also improve the knowledge and attitude of current ECPs.34
In conclusion, this is the first large study to focus on caffeine and behavioural symptoms in older patients in nursing homes. If caffeine proves to be related to several types of behavioural symptoms, a relatively simple intervention (such as adjusting caffeine consumption) might prove beneficial and improve the patient’s quality of life. Embodiment of this study in the ECP training program serves to update the medical research training program and facilitates a continuous link between education and research. 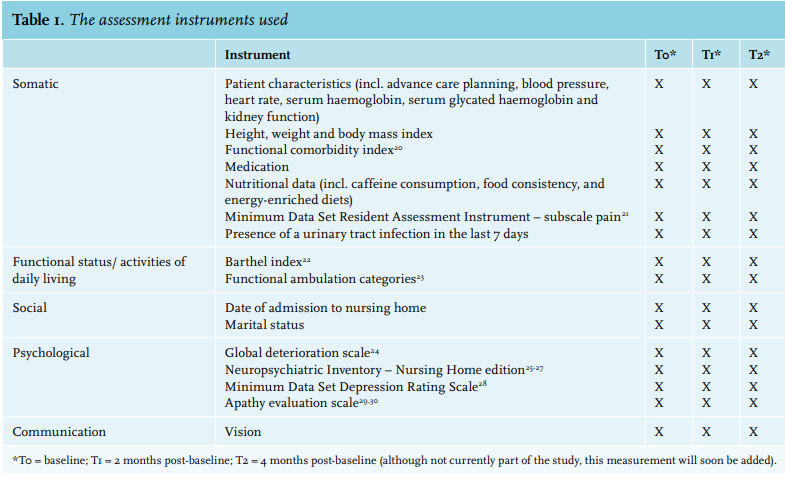
REFERENCES