KEYWORDS
Antiemetic prophylaxis, chemotherapy, drug-drug interactions
INTRODUCTION
Over the last years, great improvements have been achieved in the control of chemotherapy-induced nausea and vomiting (CINV). A new group of antiemetics, the neurokinin-1 (NK1 ) receptor antagonists, has been developed. In combination with 5-HT3 antagonists and dexamethasone, this treatment prevents 70-80% of CINV.1 In the last years the international guidelines of the American Society for Clinical Oncology (ASCO), Multinational Association of Supportive Care in Cancer (MASCC), the European Society of Medical Oncology (ESMO), and the National Comprehensive Cancer Network (NCCN) were updated.2,3
The antiemetic regimens implemented in the Netherlands, based on scientific evidence, availability and costs, are shown in table 1. Patients on highly emetogenic chemotherapy (> 90% of the patients experience CINV in the absence of antiemetic prophylaxis) receive a standard antiemetic regimen of three medications: ondansetron, aprepitant and dexamethasone. The addition of aprepitant to ondansetron and dexamethasone has significantly increased efficacy in controlling nausea and vomiting.4-6 With moderately emetogenic chemotherapy (30-90%), the prophylaxis involves a 5-HT3 -receptor antagonist (ondansetron) and dexamethasone. Low emetogenic chemotherapy (10-30%) only requires antiemetics on the day of administration, without specific preference for one class of drugs. When patients experience breakthrough or refractory symptoms another drug can be added, e.g. olanzapine or metoclopramide.2,3 Olanzapine might soon become part of the standard regimen for highly emetogenic chemotherapy.7 In patients who have anticipatory CINV or extreme anxiety, lorazepam or another anxiolytic drug can be administered, prior to and during the chemotherapy.8
In the international guidelines, several drugs are included in the standard regimens, which are not yet implemented in our national or local guidelines9 because they are not yet available or not reimbursed due to high costs, such as fosaprepitant, rolapitant, netupitant, palonosetron and NEPA, a combination of netupitant and palonosetron. Fosaprepitant is an intravenous prodrug of aprepitant, which showed non-inferiority of a single intravenous dose of fosaprepitant compared with oral administration of aprepitant for three days.10 Palonosetron is a newer 5-HT3-receptor antagonist with a longer half-life than ondansetron (40 vs 3 hours), with superior efficacy in moderately and highly emetogenic chemotherapy.11-13
Besides the better prevention of CINV, the concurrent use of several antiemetic drugs simultaneously, especially including aprepitant, may pose an increased risk of drug-drug interactions.14 Here, we will discuss the complexity and clinical significance of possible drug-drug interactions with aprepitant in anti-cancer treatment.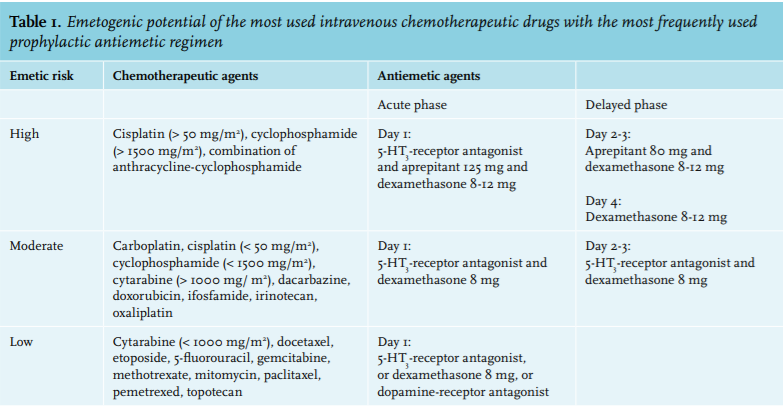
Pharmacokinetic drug-drug interactions due to aprepitant
Aprepitant is a moderate inhibitor of CYP3A4 during the chemotherapy treatment,15 while after a three-day treatment with aprepitant it induces CYP2C9, and to a lesser extent, CYP3A4.16 The induction effect is maximum at three to five days after the last dose of aprepitant, and thereafter gradually declines over two weeks.17 The most important interactions are due to the effect of aprepitant on other drugs, i.e. on the other antiemetics, mainly dexamethasone, on anticancer drugs, and other drugs that are frequently used in this population (painkillers, anticoagulants, and psychoactive drugs) (table 2). 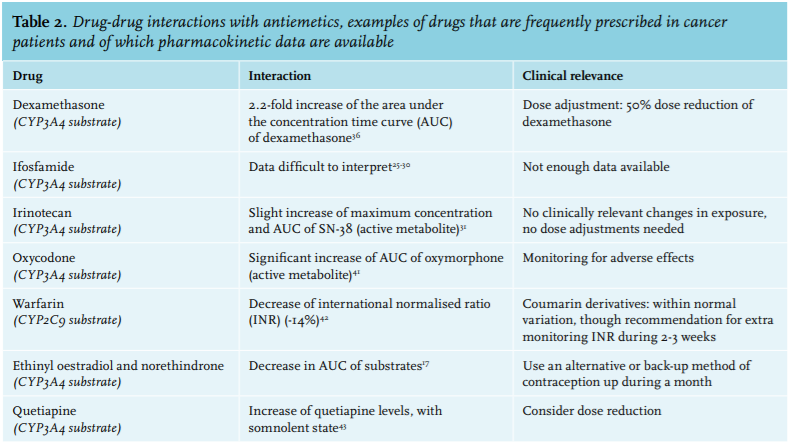
Interactions between aprepitant and anticancer drugs
Aprepitant could potentially inf luence the pharmacokinetics of anticancer drugs that are CYP3A4 or CYP29C substrates. Known substrates of CYP3A4 include cyclophosphamide, docetaxel, erlotinib, etoposide, gefitinib, ifosfamide, irinotecan, imatinib, paclitaxel, tamoxifen and vinca alkaloids. Some of the anticancer drugs are metabolised by multiple CYP enzymes, such as CYP3A4, CYP2B6 and CYP2C9 for cyclophosphamide, and CYP3A4 and CYP2D6 for tamoxifen.18 Several of these compounds are pro-drugs, e.g. irinotecan, cyclophosphamide and ifosfamide, of these, cyclophosphamide and ifosfamide need the CYP3A4-enzyme to be activated.19-21 No chemotherapeutic drugs are predominantly metabolised by CYP2D9.18 Here we will give an overview of the most important current data on potential drug-drug interactions with anticancer drugs.
Several studies have investigated the metabolism of cyclophosphamide during co-administration of aprepitant. Although one of the studies found a greater exposure to cyclophosphamide,22 no important difference in the exposure of the active (4-OH) metabolite was found, only lower exposure to its neurotoxic metabolite.22-24
Aprepitant is suspected to increase the risk of encephalopathy when co-administered with ifosfamide, but just a few case reports and retrospective studies are available.25-30 Only one case report showed pharmacokinetic data, but these are difficult to interpret.25 Further studies are needed to confirm this effect on the pharmacokinetics of ifosfamide and a causal relation with an induced risk of encephalopathy. However, if encephalopathy develops during a course containing ifosfamide, a different antiemetic regimen should be considered in subsequent treatment.
The effect of aprepitant on the pharmacokinetics of irinotecan and its active metabolite SN-38 was studied in a pilot study. The maximum concentration and the area under the concentration time curve (AUC) of SN-38 were slightly higher when co-administered with aprepitant (23.5 vs 18.8, and 18 vs 15, respectively), but this difference does not seem to be clinically relevant.31
Pharmacokinetic studies of vinorelbine combined with aprepitant showed no difference in AUC on day 1 compared with day 8, excluding a clinically relevant inhibiting effect.32 Likewise, aprepitant did not influence the pharmacokinetics of docetaxel.33
Among the anticancer drugs, not only chemotherapeutic agents are CYP substrates, but also many of the oral kinase inhibitors. However, most of them will not often be used concomitantly with aprepitant, due to their lower emetogenic impact. One of these compounds, erlotinib, was shown to have a relevant drug interaction with aprepitant when it was used off-label for pruritus. Erlotinib had a two-fold higher serum level, which could increase toxicity as well as efficacy.34
For many other chemotherapeutic agents which are CYP3A4 substrates, there is a theoretical interaction with aprepitant, but no clinical studies have been performed to investigate this effect, for example for doxorubicin, etoposide, gefitinib, imatinib, paclitaxel, vinblastine or vincristine.35
Interactions between aprepitant and other antiemetic agents
Due to the moderate inhibition of CYP3A4 by aprepitant, the metabolism of dexamethasone is decreased, leading to a 2.2-fold increase of the AUC of dexamethasone.36 High-dose dexamethasone gives a high risk of serious adverse effects, such as infections and mental disturbances.37 In the guidelines, it is recommended that the dose of dexamethasone is decreased by 50% when combined with aprepitant. Pharmacokinetic studies with aprepitant did not reveal a different effect for oral versus intravenous dosing of dexamethasone.38
Ondansetron, the other compound of the three-drug combination to prevent CINV with highly emetogenic agents, is also a substrate of CYP3A4, as well as CYP1A2 and CYP2D6.39 In contrast to dexamethasone no clinically relevant pharmacokinetic interaction was observed when co-administered with aprepitant.40 This can be explained by the fact that the other CYP enzymes are alternative routes for ondansetron when CYP3A4 is blocked.
Interactions between aprepitant and other medications
Other CYP3A4 or CYP2C9 substrates that are frequently used by cancer patients and therefore could potentially have an interaction with aprepitant include oxycodone (CYP3A4), coumarin derivatives (CYP2C9), and hormonal contraceptives (CYP3A4).14,35
In pharmacokinetic studies with oxycodone, its active metabolite oxymorphone had a significantly higher AUC (+34%), but this did not result in more adverse effects (e.g. respiratory depression, sedation, constipation, nausea or vomiting).41 It seems reasonable not to make preventive dose adjustments, but to monitor patients more closely during combined therapy.17
All studies on coumarin derivatives were done with warfarin instead of acenocoumarol or phenprocoumon. From five days after the first administration of aprepitant (three-day schedule), the S-warfarin plasma levels were decreased, with a maximum difference at day 8 (-34%), resulting in a lower international normalised ratio (INR) of -14%.42 A point of discussion is whether this is a clinically relevant effect, taking into account the normal variation in INR. In daily practice, extra INR monitoring for two or three weeks after aprepitant administration is recommended.
There is also an effect of aprepitant on hormonal contraceptives due to CYP3A4 induction. A pharmacokinetic study showed a long-lasting (three to four weeks) decrease in the AUC of ethinyl oestradiol and norethindrone (> 60%). Patients should be advised to use an alternative or back-up method of contraception for up to one month after the last dose.17
Psychoactive agents are often used by patients with cancer, but most of these drugs are metabolised by CYP2D6, so are not susceptible for CYP inhibition or induction due to aprepitant. Quetiapine is an exception of a psychoactive drug that has been demonstrated to have a clinically relevant drug-drug interaction with aprepitant. This drug is a CYP3A4 substrate and has showed higher plasma levels when co-administered with aprepitant.43
DISCUSSION
In this review, we give an overview of the potential risk of clinically relevant drug-drug interactions with aprepitant, an NK1 -receptor antagonist. In particular, it can influence the pharmacokinetics of other drugs, including oncolytic drugs, as it is initially an inhibitor and later on an inducer of CYP3A4. When CYP-enzyme induction leads to lower exposure of its substrate, this could theoretically result in loss of effectiveness. The same holds true for enzyme inhibition when a pro-drug needs CYP enzymes to form the active drug. So far, it is not known if this will result in clinically relevant changes during chemotherapy combined with aprepitant. Because it takes several days before enzyme induction reaches its effect, the effect depends on the timing of the different drugs. However, when a serious interaction occurs, this might be unrecognised since pharmacokinetic results are not usually available. In curative regimens, such as bleomycin-etoposide-cisplatin for carcinoma of the testis, this potential risk should be avoided. So far, only a few pharmacokinetic studies have investigated these serious potential interactions. In our hospital, when we suspect an interaction between a chemotherapeutic drug in a therapy with curative intent, we have decided not to use aprepitant until studies have demonstrated that the anti-tumour effects are not decreased.
Apart from the need for more data on the effects of aprepitant, newer NK1 -receptor antagonists, such as netupitant and rolapitant, which interfere less with CYP enzymes compared with aprepitant, might be safer options. Several phase III studies have shown good responses of rolapitant compared with placebo.44,45
However, no studies were powered to compare the efficacy and safety of aprepitant, netupitant (in the combination with palonosetron as NEPA) and rolapitant.46 Moreover, for the two newer agents very few studies have been conducted to prove that they might have less impact on the pharmacokinetics, and thus the effect and toxicity, of chemotherapeutic agents. Besides, these agents are not yet available in the Netherlands.
In conclusion, it is crucial that more studies on drug-drug interactions with aprepitant and their influence on pharmacokinetics are performed. Therapeutic drug monitoring of oncolytic drugs could be useful to assess the clinical relevance of the interactions. However, it is crucial that more research is done to define the concentration-effect relationships. This knowledge should then put into perspective the clinical consequences and recommendations for each drug, such as dose adjustments (for example for dexamethasone when co-administered with aprepitant), avoidance or extra monitoring. In the meantime, physicians should be aware of the potential risk of drug-drug interactions with aprepitant, especially in regimens with curative intent. Close collaboration between oncologists and pharmacists is essential for safe drug administrations during chemotherapy.
CONCLUSIONS
Aprepitant, an NK1 -receptor antagonist, is now standard treatment in patients receiving highly emetogenic chemotherapy, combined with ondansetron and dexamethasone. Aprepitant is an inhibitor and inducer of CYP3A4, so it could influence the pharmacokinetics of CYP3A4 substrates, including chemotherapeutic drugs. The new NK1 -receptor antagonists netupitant (in the combination with palonosetron as NEPA) and rolapitant might be safer options, as they interfere less with CYP enzymes compared with aprepitant. However, they do not have EMA approval at this moment. More studies should investigate these potential drug-drug interactions to provide data on their clinical relevance. High awareness of these risks among oncologists and close collaboration with pharmacists could increase the safety of cancer patients receiving highly emetogenic chemotherapy. This is especially true in regimens with curative intention.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES