INTRODUCTION
Cat bites are common and Dutch guidelines advise to prescribe antibiotic prophylaxis of amoxicillin/ clavulanate for five days.1 Infected bite wounds often contain a combination of pathogens. Common aerobic bacteria include Pasteurella (75%), Streptococcus (46%), Staphylococcus (35%), Neisseria (35%) Moraxella (35%) and Corynebacterium (28%) species. Anaerobic microorganisms are less common and include Fusobacterium (33%), Porphyromonas (30%) and Bacteroides (28%) species.2 Anaerobiospirillumsucciniciproducens is a rare Gram-negative spiral-shaped anaerobic rod that can cause life-threatening infection. With the introduction of matrix-assisted laser desorption/ionisation time-of-flight mass spectrometry (MALDI-TOF MS), we expect that this bacterium will be identified more often. Therefore, it is important to learn more about the characteristics, the clinical course and treatment of disease caused by this microorganism. In addition, A. succiniciproducens can be mistaken for Campylobacter species, which requires a different treatment.
In this case report, we aim to demonstrate the clinical signs of A. succiniciproducens sepsis and hypothesise about the source of this bacterium. In addition, we emphasise the need to consider a wide range of pathogens after a cat bite.
CASE REPORT
A 40-year-old woman was referred to the emergency room because of anaemia and fever. Her medical history included diabetes mellitus type 2 and liver cirrhosis (Child Pugh class C) with portal hypertension, ascites and a recent episode of bleeding oesophageal varices. Underlying alcohol abuse was suspected. Four weeks earlier she was bitten by a cat in her right thenar. She had received tetanus vaccination and a prescription for amoxicillin/clavulanate. She reported malaise and diarrhoea for one week. Five days before presentation she fell from the stairs. The body temperature was 38.1 °C, blood pressure 100/60 mmHg and heart rate 105/minute. An extensive haematoma with swelling was seen from her right hip to knee. Table 1 shows the laboratory results. Fluid resuscitation, transfusions with erythrocyte concentrate and plasma and empiric cefuroxime and gentamicin were initiated immediately. A chest X-ray showed no infiltration.
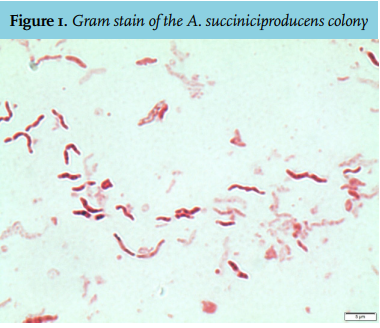
Computed tomography (CT) scan of thorax, abdomen and legs, primarily performed to explore other foci of bleeding and foci of infection in lungs, abdomen and the haematoma, confirmed an extensive haematoma in the right leg but no localised infection. Ultrasound excluded deep venous thrombosis. She was admitted to the intensive care unit for additional support with inotropic medication. Two days later, an anaerobic blood culture became positive. Gram staining showed Gram-negative spiral-shaped rods, suspected of Campylobacter species. Anaerobic subculture on sheep blood agar showed flat translucent colonies, identified as A. succiniciproducens by MALDI-TOF MS (Bruker Daltonics, Bremen, Germany) with a score of 2.47. Figure 1 shows a Gram stain of the colony. Three other blood cultures, including two aerobic, became positive later with the same microorganism. The isolate appeared susceptible to penicillin (minimum inhibitory concentration (MIC) 0.25 mg/l), amoxicillin/clavulanate (MIC 0.064 mg/l) and metronidazole (MIC 4 mg/l) and resistant to clindamycin (MIC 24 mg/i).
Treatment was switched to benzylpenicillin monotherapy, and later to oral amoxicillin/ clavulanate for a total duration of 14 days. The clinical response was good. Amoxicillin/clavulanate was chosen because a purulent discharge appeared on a wound overlying the haematoma. The hypothesis of an abscess was later rejected and the haematoma reabsorbed spontaneously. After discharge the patient admitted that she had not taken the amoxicillin/ clavulanate prophylaxis after the cat bite. 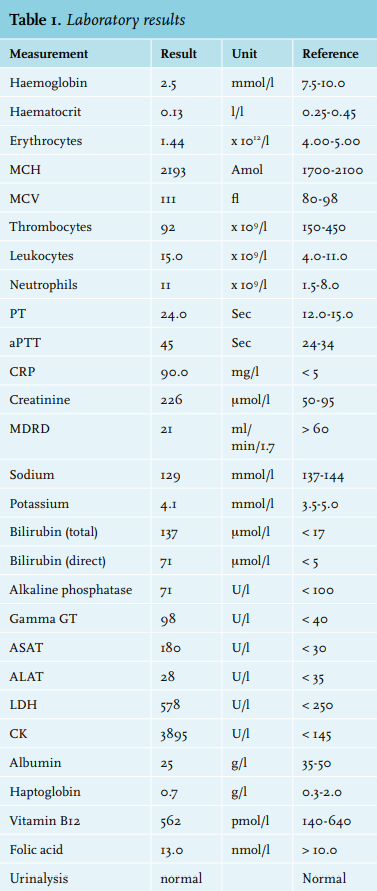
DISCUSSION
A. succiniciproducens blood stream infection is a serious but rare condition. This Gram-negative, spiral, anaerobic rod was first isolated by Davis et al. from the throats and faeces of beagle dogs.3 Two types of Anaerobiospirillum species have been identified: A. succiniciproducens and A. thomasii. 4A. succiniciproducens mainly resides in the gastrointestinal tract of healthy dogs and cats, while A. thomasii was also isolated from human faeces.3,4 Because of its morphology, Anaerobiospirillum can be mistaken for Campylobacter species, which requires another choice of antibiotic.5 In 33 reported patients with A. succiniciproducens blood stream infection, 90% had an underlying disease, 39% had a history of alcohol abuse and 11% had pre-existing liver disease.6 Of 24 symptomatic patients, 17 (71%) had gastrointestinal symptoms and 18% had a polymicrobial blood stream infection. Mortality was substantial at 31%. Exposure to animals (not even specified to bites) was documented in only three cases. Transmission of A. succiniciproducens might occur through cat bites but also through dog bites.3
The identification of A. succiniciproducens has become much easier, faster and more reliable since the introduction of MALDI-TOF MS. This technique is based on identification of the protein particles that are produced when bacteria are exposed to laser ionisation. Recognition of these products depends on the database behind the system. The Bruker database to date contains spectra of three A. succiniciproducens isolates. The species is also correctly identified by the Vitek MS system (bioMérieux Inc., Durham, NC).7,8
Correct determination of A. succiniciproducens is essential for choosing effective antibiotic therapy. When mistaken for Campylobacter species, macrolides will probably be prescribed, to which Anaerobiospirillum is usually resistant. It is generally susceptible to amoxicillin/clavulanate, second and third generation cephalosporins, carbapenems and fluoroquinolones.5,7,8 As polymicrobial infection is often present, antibiotic treatment should be carefully chosen on an individual basis.
Our patient visited the emergency room four weeks before she was admitted with A. succiniciproducens sepsis, with an ongoing bleeding wound after a cat bite. She was treated with compresses but did not take the prescribed antibiotics. The cat bite is still a possible cause of the infection, although the incubation time seems to be rather long. A median duration of 12 hours between cat bites and the appearance of the first symptoms of infection has been described.2 Another possibility is that A. succiniciproducens became part of the gastrointestinal flora in our patient, because of her daily contact with her cat and dog, and that translocation from the gut occurred, facilitated by her liver cirrhosis and portal hypertension. A. succiniciproducens is usually not isolated from faeces of healthy humans, but it was isolated in two patients with diarrhoea.9,10 A third, less likely option, is that the haematoma became infected with A. succiniciproducens.
A. succiniciproducens is a rare but potentially lethal pathogen and infection with this microorganism should be managed with antibiotics in an early phase. Especially in immunocompromised patients or patients with underlying diseases, a complete history with attention to contact with animals is needed.
REFERENCES