KEYWORDS
Bowel preparation; capsule endoscopy; simethicone; standard of care; visualisation quality
INTRODUCTION
Small bowel capsule endoscopy (SBCE) has proven to play a crucial role in the diagnosis and management of several small-bowel diseases such as obscure gastrointestinal bleeding and Crohn’s disease.1-4 Unfortunately, its diagnostic yield may be limited by impaired small bowel visualisation quality due to intestinal juice, air bubbles or food residue and a lower completion rate of the examination caused by delayed gastric and small bowel transit time.
A bowel preparation regimen prior to SBCE might improve the quality of small bowel visualisation and thereby the diagnostic yield, but it may also have an adverse effect on gastric and small bowel transit time.5-7 Since the introduction of SBCE in 2000 a lot of research has been carried out in order to define the optimal preparation regimen prior to SBCE including polyethylene glycol (PEG) and the addition of anti-foaming agents or prokinetics. PEG showed to have a beneficial effect on small bowel visualisation compared with other purgatives.5,6,8,9 The addition of prokinetics mainly resulted in a shortening of gastric transit time while few effects on small bowel transit time and completion rate were seen.7,11 Addition of simethicone, an anti-foaming agent, to a preparation of PEG prior to SBCE showed improvement of bowel cleansing and small bowel visualisation in many cases; however, the effect on transit times, diagnostic yield and completion rate remains somewhat contradictory.12-17 Despite much research regarding the optimal preparation regimen prior to SBCE, no consensus has been reached.18,19 Differences in the preparation regimens used lead to heterogeneity. Moreover, no widely accepted measuring method and definition is available of adequate quality of small bowel visualisation, impeding standardisation of an effective bowel preparation regimen.
The primary aim of this study was to evaluate the added value of simethicone to SBCE preparation with PEG on small bowel visualisation quality. We hypothesise that a preparation including simethicone will lead to better small bowel visualisation compared with a preparation of PEG alone. The secondary aim was to evaluate the use of anti-foaming agents for SBCE preparation in the Netherlands.
MATERIALS AND METHODS
Study design and patients
In this single-blinded, retrospective cohort study, data were prospectively collected from patients who underwent SBCE from May 2011 until December 2012.
Exclusion criteria consisted of general contraindications for SBCE such as swallowing difficulties, known or suspected intestinal fistulas or stenosis and the presence of an implantable cardioverter defibrillator. Additional exclusion criteria were impaired intestinal motility, severe diverticulosis, pregnancy and age less than 18 years.
Bowel preparation and SBCE examination
Data on the two cohorts were collected from medical records. One cohort received a preparation with only PEG while the other cohort received PEG and simethicone prior to SBCE. Patients in the PEG group underwent SBCE before November 2012 and received standard bowel preparation consisting of a liquid diet 1 day before SBCE, 2 litres of PEG and a clear liquid diet in the evening before SBCE followed by an overnight fast. Patients in the PEG-S group, who underwent SBCE between March and December 2012, received simethicone in addition to standard bowel preparation with PEG. They ingested 2 ml of simethicone suspension containing a total amount of 82.4 mg of simethicone (Lefax, Bayer, Germany) with a small amount of tap water 15 minutes prior to SBCE. All patients who took iron supplements were asked to temporarily stop these seven days before SBCE.
SBCE was performed using the Pillcam SB (Given Imaging, Israel). All patients were allowed to drink clear liquids and eat a light meal 4 and 6 hours, respectively, after swallowing the capsule. Images were collected for a period of 8 hours until the battery ran out. Images were reviewed using RAPID 4.0 (MedTronic, United States).
Assessment of outcomes
Thirteen out of the total 64 videos were reviewed by two experienced investigators (D.D., S.B.) regarding evaluation of the quality of small bowel visualisation. Interobserver variability was assessed and after agreement was reached on any discrepancies, the other 51 videos were reviewed by only one investigator. In cases of disagreement, investigators discussed the video until consensus was reached. Investigators were blinded to which bowel preparation patients received prior to SBCE. All images of the videos were evaluated by the investigators.
To evaluate small bowel visualisation, the amount of intraluminal gas as well as faecal contamination limiting mucosal visibility was assessed for every video using a four-point grading scale: Grade 0: no intraluminal gas/ faecal contamination, Grade 1: a few gas bubbles/little faecal contamination, no limitations for interpretation of SBCE, Grade 2: presence of some intraluminal gas/ faecal contamination leading to moderate limitations for interpretation, Grade 3: presence of a substantial amount of intraluminal gas/faecal contamination leading to severe limitations for interpretation. Grade 0 and 1 were classified as not limiting for interpretation of SBCE whereas grade 2 and 3 were considered as limiting for the interpretation of SBCE. The quality of visualisation of the proximal and distal small bowel was assessed separately. The proximal part of the small bowel was defined as one hour of video after the first duodenal bulb image while the distal part of the small bowel began one hour before the first caecal image.
Small bowel transit time was defined as the time from the first image of the duodenal bulb until the first caecal image.
The diagnostic yield was classified as either ‘explanatory’ or ‘not explanatory’. If findings on images could explain the patient’s signs or symptoms, diagnostic yield was assessed as ‘explanatory’. Images were assessed as ‘not explanatory’ if they did not show any abnormalities.
Use of anti-foaming agents in the Netherlands
We randomly selected 16 Dutch hospitals who perform SBCE. Selected hospitals were spread over all regions of the Netherlands and consisted of a mix of university hospitals, regional teaching hospitals and peripheral hospitals.
To obtain information on the frequency of the use of an anti-foaming agent prior to SBCE in these hospitals, brochures were consulted and endoscopy departments were contacted by telephone. For this study, we focused on the use of an anti-foaming agent only. Use of purgatives was not included in our analysis.
Statistical analysis
Descriptive statistics were expressed in means ± standard deviation (SD). Differences in categorical variables between patient groups were compared with the chi-square test, differences in means were compared with the unpaired T-test. A p-value
RESULTS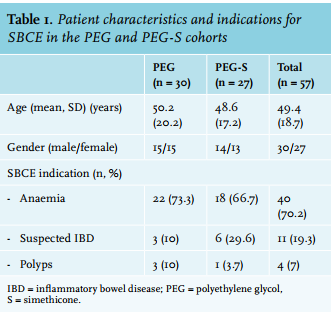 Patient characteristics
Patient characteristics
Data of 64 patients who underwent SBCE were analysed. Data of 7 patients, 4 in the PEG group and 3 in the PEG-S group, had to be excluded from analysis due to an empty battery of the Pillcam while the capsule was still in the small bowel. Therefore, a total of 57 patients were included in this study of which 30 patients in the PEG group (mean age 50 years, 50% men) and 27 in the PEG-S group (mean age 49 years, 52% men). There were no significant differences between the two groups regarding age (p = 0.75) and gender (p = 0.89). Indications for SBCE consisted of anaemia (70.2%), suspected inflammatory bowel disease (IBD) (19.3%), polyps (7.0%) or other (3.5%). Of the 4 patients with polyps as an indication for SBCE, 3 had a known polyposis syndrome and one patient was previously diagnosed with polyps. Patient characteristics are listed in table 1.
All patients ingested the capsule without difficulty and no serious adverse events were reported during the examination in the two groups.
Capsule endoscopy imaging quality
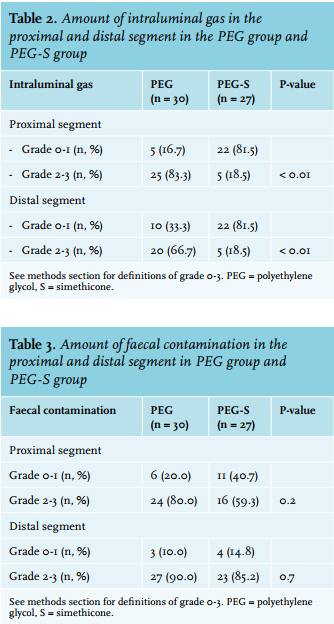
The amount of intraluminal gas limiting the visualisation quality of SBCE in the PEG group was significantly higher than in the PEG-S group at 83.3% vs 18.5%, respectively, in the proximal segment (p < 0.01) and 66.7% vs 18.5% in the distal segment (p < 0.01) (table 2). No significant difference was seen regarding the amount of faecal contamination limiting visualisation quality between both groups in the proximal segment (80.0% for PEG vs 59.3% for PEG-S, respectively p = 0.2) and distal segment (90.0% for PEG vs 85.2% for PEG-S, p = 0.7, respectively) (table 3).
Small bowel transit time and diagnostic yield
The mean small bowel transit time did not differ significantly between the two groups with a mean small bowel transit time of 4.0 hours (SD 1.1) in the PEG group and 3.9 hours (SD 1.3) in the PEG-S group (p = 0.7). A definitive diagnosis was established in 13 patients (43.3%) in the PEG group and 6 patients (22.2%) in the PEG-S group (p = 0.16).
Use of anti-foaming agents in the Netherlands
We assessed the use anti-foaming agents in SBCE bowel preparation of 16 hospitals. Of these 16 hospitals, 3 (18.8%) were academic hospitals, 8 (50%) were regional teaching hospitals and 5 (31.3%) were peripheral hospitals.
Of all contacted hospitals only 3 (18.8%) used an anti-foaming agent prior to SBCE as standard practice. One hospital (6.3%) reported not to use an anti-foaming agent as standard practice, but it was available to use in specific cases. Of the 3 hospitals routinely using anti-foaming agents, 2 were academic hospitals and 1 was a regional teaching hospital. Two of these hospitals were located in the same region in the Netherlands. The other 12 hospitals (75%) reported no use of anti-foaming agents prior to SBCE.
DISCUSSION
This study evaluates the effect of adding simethicone to a bowel preparation regimen with PEG prior to SBCE and showed an improvement in visualisation of small bowel mucosa by significantly reducing the amount of intraluminal gas in both the proximal and distal small bowel. However, the addition of simethicone did not have an effect on the amount of faecal contamination, small bowel transit time and diagnostic yield. The use of anti-foaming agents in SBCE preparation is not standard practice in the Netherlands.
An increase in the quality of small bowel visualisation by adding simethicone to a bowel preparation of PEG compared with fasting is in line with several randomised studies and a systematic review.13-17,20 Moreover, the preparation regimen of PEG with simethicone proved to improve small bowel visualisation in children.21 The quality of small bowel visualisation may be influenced by intraluminal gas, debris and juices. In this study, a bowel preparation of PEG and simethicone reduced intraluminal gas and thereby improved visualisation. However, it did not reduce the amount of faecal contamination possibly limiting the quality of visualisation. Similar results were obtained by Rosa et al.16 who demonstrated that a preparation of PEG and simethicone leads to a reduction of air bubbles in the entire small bowel while not reducing intraluminal fluid and debris. In contrast to our findings, this reduction was observed in comparison with fasting and not when comparing with PEG only. Our study seems to be the only study to show a decrease of intraluminal gas and no effect on faecal contamination when comparing bowel preparation of PEG and simethicone versus PEG only.
A few studies also investigated the effect of simethicone in reducing faecal contamination. Evaluation of faecal contamination is useful when assessing the quality of small bowel visualisation since this is not only influenced by intraluminal gas but also by other factors possibly limiting visualisation of the small bowel mucosa.
Our findings are in line with two randomised studies which also demonstrated no effect of simethicone on intraluminal fluid and debris.12,16 Only one study assessing fluid and debris in the context of small bowel visualisation reported an increase of the quality of visualisation in the distal small bowel when using simethicone and PEG compared with PEG only.14 That study also showed that PEG only led to a better quality of small bowel visualisation compared with fasting. Importantly, the amount of PEG used in their study was less (1 litre) than in our study (2 litres) while the amount of simethicone was higher (300 mg). This leads to the hypothesis that the increase in the quality of small bowel visualisation reported in their study might be caused by a reduction of intraluminal gas rather than a reduction of intraluminal debris and fluids. Moreover, it is to be expected that adding simethicone to a preparation of PEG does not lead to a decrease of faecal contamination since simethicone only reduces the surface tension of air bubbles.
The present study showed that the addition of simethicone to a bowel preparation with PEG has neither an effect on small bowel transit time nor on diagnostic yield. This finding is supported by most other studies comparing a preparation of PEG and simethicone to PEG except for one study in which the addition of simethicone led to a significantly longer small bowel transit time.12-14,16,22 To our knowledge, no previous study has reported a better diagnostic yield after adding simethicone to PEG.12,16,21,22
Although simethicone causes a better visibility of the small bowel mucosa, this does not lead to an increase in positive findings. Hence, simethicone causes a better quality of small bowel visualisation but does not lead to a better diagnostic yield. A possible explanation might be that visualisation is influenced by several other factors than intraluminal gas. Another explanation might be that all these studies are underpowered to detect a significant positive effect on diagnostic yield. Overall, the rate of positive findings in our study is low. This could be explained by the fact that SBCE has become a more widely used diagnostic instrument since its introduction in 2000 with a more flexible indication and therefore may lead to more patients undergoing SBCE without underlying pathology.23
This study demonstrated that the use of simethicone prior to SBCE is not standard practice in the Netherlands. Although SBCE guidelines did not reach consensus on the standard preparation regimen, previous literature demonstrated improvement in small bowel visualisation by simethicone. The present study emphasises this improvement in the quality of small bowel visualisation. Moreover, the costs of simethicone are low, there have been no serious adverse events reported when using simethicone prior to SBCE and it is widely available in endoscopy units for foam reduction for oesophagogastro-duodenoscopy and colonoscopy.14,15,17 Therefore, we suggest to consider the use of simethicone in bowel preparation prior to SBCE in the Netherlands.
This study has several limits. First, patients were not randomly allocated to either the purgative or purgative with simethicone cohort. On the other hand, the two assessors evaluating the images were blinded to which preparation patients had received. Second, the two groups were relatively small, however big enough to obtain significant results regarding quality of small bowel visualisation. Another limitation is the assessment of intraluminal gas and faecal contamination. This is measured by a relatively subjective scale which has not been validated. The scale we used was also used by Ge et al.15 Although recent studies have proposed a validated scale, at the time of our study no validated scale was available.24,25 It is to be questioned if a quantitative measuring method (i.e. the counting of air bubbles) has an additional value for clinical practice. The scale we used seems to be closely related to the evaluation of SBCE images in daily practice.
In conclusion, this study demonstrates that a preparation of PEG and simethicone prior to SBCE improves the visualisation quality of the small bowel by reducing intraluminal gas. Moreover, the use of anti-foaming agents in SBCE preparation is not standard practice in the Netherlands. To date, there is no consensus on a standardised bowel preparation regimen prior to SBCE. Considering the potential benefit, low costs and good safety profile, we recommend simethicone as part of standard bowel preparation in patients undergoing SBCE. As demonstrated by our study and previous literature, the addition of simethicone does not improve diagnostic yield. Therefore, we recommend that future research should focus on stricter purgative regimens in order to investigate its potential beneficial effect on diagnostic yield.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES