KEYWORDS
Anti-TNF agents, health insurance database, inflammatory bowel disease, pharmacoeconomics, real-world analysis
INTRODUCTION
The introduction of anti-tumour necrosis factor (anti-TNF) antibodies has revolutionised the therapy of Crohn’s disease and ulcerative colitis, collectively known as inflammatory bowel disease (IBD). Anti-TNF agents are able to induce and maintain remission in IBD patients.1-6 Infliximab was registered in the Netherlands for Crohn’s disease in 1999 and for ulcerative colitis in 2006 and adalimumab was registered in the Netherlands for Crohn’s disease and ulcerative colitis in 2007 and 2012, respectively.
The clinical management of IBD patients with anti-TNF agents is complicated by primary and secondary non-response. Approximately 30% of patients do not respond to anti-TNF induction therapy (primary non-responders),1-7 and up to half of initial responders will gradually lose response over time (secondary non-responders).1,8-11 Primary and secondary non-response are related to low serum drug concentrations and the development of anti-drug antibodies.12-19 The proportion of IBD patients with a durable response to anti-TNF treatment in a real-life setting has been investigated in relatively small cohorts.10,11
Several strategies are used to prevent and treat primary and secondary non-response to anti-TNF agents. Firstly, combination therapy (consisting of an anti-TNF agent combined with an immunomodulator) is more effective compared with anti-TNF monotherapy,20 which can (at least partly) be explained by reduced anti-drug antibody formation.21 Secondly, loss of response can often be managed by increasing the dose and/or decreasing the dosing interval of the anti-TNF agent.22 Thirdly, loss of response to anti-TNF agents, especially when this is related to anti-drug-antibody formation, can be overcome by switching to another anti-TNF agent,22 or by adding an immunomodulator if a patient is receiving anti-TNF monotherapy.
It is unknown how many IBD patients receive combination therapy and how often anti-TNF treatment is intensified in daily practice. Furthermore, associated treatment outcomes and drug costs of anti-TNF agents in a large real-life population are relatively unknown. Van der Valk et al. studied IBD health care and medication costs in a Dutch cohort of 2252 patients in 2011.23 Bernstein et al. assessed costs of IBD management in a large real-life Canadian cohort in 2005 and 2006, but they did not specifically focus on anti-TNF use and related treatment outcomes.24 The aim of the present study was to investigate: (i) drug survival rates of anti-TNF agents, (ii) clinical outcomes of anti-TNF therapy, and (iii) drug costs of TNF blockers in a large population consisting of approximately 22,000 Dutch IBD patients.
METHODS
Database
Health insurance claims data were provided by Achmea Healthcare, the largest health insurance provider in the Netherlands. Data were available from 2008 to 2014 on approximately 2.7 million insured persons in 2008, gradually increasing to approximately 4.2 million insured persons in 2014. This population is a representative sample of the urbanised area of the Netherlands.25
Data collection
The following data were collected from subjects who received IBD-related healthcare between 2008 and 2014 (observation period).
Background information: year of birth, gender, number of days insured by Achmea per year, year of death (if applicable), start and stop date of the insured period. IBD-related healthcare: diagnosis (Crohn’s disease or ulcerative colitis) and treatment setting (inpatient or outpatient).
IBD-related medication use: administration/dispensation date, dose and costs of infliximab, adalimumab, corticosteroids (prednisone or budesonide), thiopurines (azathioprine, 6-mercaptopurine or 6-tioguanine) and methotrexate. Data on infliximab use was available from 2012 to 2014 due to a different reimbursement system before 2012. Prior to 2012, infliximab costs were reimbursed as part of hospital care, thus treatment details were not specified in healthcare claims before 2012. As of 2012, infliximab costs are directly reclaimed by pharmacies based on specific dosages and dispensation dates.
Comorbidity: documented healthcare claims for psoriatic arthritis, ankylosing spondylitis, psoriasis and rheumatoid arthritis.
Outcomes
The primary outcome was anti-TNF drug survival (i.e. time from start of anti-TNF therapy to discontinuation). Secondary outcomes included time to anti-TNF dose intensification, time to corticosteroid initiation and time to IBD-related hospitalisation in anti-TNF starters and analysis of potential determinants for time to drug discontinuation, treatment intensification, hospitalisation, and corticosteroid initiation. Moreover, treatment intervals, dosing regimens and drug costs of anti-TNF therapy were analysed.
Classifications, definitions, calculations and selection criteria
All analyses were performed on patients aged ≥ 18 years at the end of the observation period. Patients who received their first infliximab infusion > 16 weeks after the start of the observation period were considered to be infliximab starters. Patients who received their first pharmacy dispensation of adalimumab > 6 months after start of the observation period were considered adalimumab starters. These cut-offs were based on the assumption that infliximab intervals are unlikely to exceed a 16-week period and that the amount of dispensed adalimumab vials is unlikely to cover a treatment period longer than 6 months. In order to distinguish between patients starting on anti-TNF monotherapy or combination therapy, pharmacy dispensations of immunomodulators and anti-TNF agents were divided into semesters. Anti-TNF starters receiving a prescription for an immunomodulator in the first semester of anti-TNF treatment were defined as patients using combination therapy.
An infliximab dose adaptation was defined as a dose increase or decrease of at least 50 mg and/or an increase or decrease in the treatment interval between two infusions of ≥ 25%. Infliximab discontinuation was defined as a definitive treatment stop or an infusion interval of > 16 weeks. Infliximab restart was defined as at least one infliximab infusion after treatment discontinuation.
Adalimumab dosing regimens were based on the average amount of adalimumab provided at each dispensation (amount dispensed in mg divided by the time until next dispensation). Adalimumab dosing regimens were categorised into < 40 mg every other week, 40 mg every other week, 40 mg every week and > 40 mg every week based on the following cut-offs: < 15 mg per week, 15-30 mg per week, 30-60 mg per week and > 60 mg per week, respectively. Adalimumab dose adaptations were defined as a change in dosing regimen category that was maintained for at least two consecutive dispensations. Adalimumab discontinuation was defined as a definite treatment stop or when the average amount of adalimumab that was dispensed by the pharmacy was < 10 mg per week. Adalimumab restart was defined as at least one adalimumab dispensation after discontinuation.
Time to drug discontinuation, treatment intensification, hospitalisation, out of hospital and in-hospital corticosteroid initiation (prednisone and budesonides) were analysed in all patients who started on anti-TNF therapy within the observation period. For all survival analyses, patients were censored on 31 December 2014, at time of death or at the time of an interruption of the insured period (i.e. if patients switched to another health insurance provider). In order to analyse time to corticosteroid initiation, hospitalisation and treatment intensification, patients were also censored at the time of anti-TNF discontinuation.
Corticosteroid use during anti-TNF induction therapy (4 weeks for adalimumab and 6 weeks for infliximab) was used as a cut-off point for analysing time to corticosteroid initiation. Because the definitions of infliximab and adalimumab treatment intensification were not comparable, time to treatment intensification was analysed for both agents separately.
Average anti-TNF treatment intervals and dosages were determined in patients who started on anti-TNF treatment during the observation period at 3, 6, 12 and 24 months after treatment initiation if they were not censored and still receiving the same anti-TNF agent. Mean infliximab dose relative to body weight was estimated using an average body weight of Dutch men and women of 70 kilogram.26 Drug costs of each anti-TNF dispensation were provided by Achmea. Total anti-TNF costs were calculated as the sum of all dispensations within the observation period and for each year separately.
Statistical analysis
All analyses were performed using SPSS 23.0 (IBM, Chicago, Illinois). Descriptive statistics were used to study cohort characteristics. Observed periods are presented in person-years. Comparisons between groups of not normally distributed dichotomous data were performed using Fisher’s exact tests. Survival data are presented as Kaplan-Meier curves. Univariate and multivariate analysis of time to event data was performed using Cox proportional hazards regression. The proportional hazards assumption was tested using visual inspection of log minus log survival plots. The threshold for statistical significance was set at p < 0.05.
Ethical approval
All provided data were completely anonymised. Data were requested and obtained through official procedures. Therefore, no ethical approval was required.
RESULTS
Cohort characteristics
A total of 22,082 patients who received IBD-related care between 2008 and 2014 were identified. The total observation period comprised 131,134 person-years. Cohort characteristics are provided in table 1. From 2008 to 2014, 1498 patients were treated with adalimumab, and 1671 patients were treated with infliximab between 2012 and 2014. The proportion of patients receiving anti-TNF treatment increased from 17% in 2012 to 19.7% in 2014 (infliximab and adalimumab combined). In this period, 476 out of 2929 (16.3%) patients had received both infliximab and adalimumab. From 2008 to 2014, 24% of IBD patients receiving an anti-TNF agent also received care (indicated by a documented health insurance claim) for at least one other disease for which anti-TNF agents are indicated, such as psoriatic arthritis, ankylosing spondylitis, psoriasis or rheumatoid arthritis.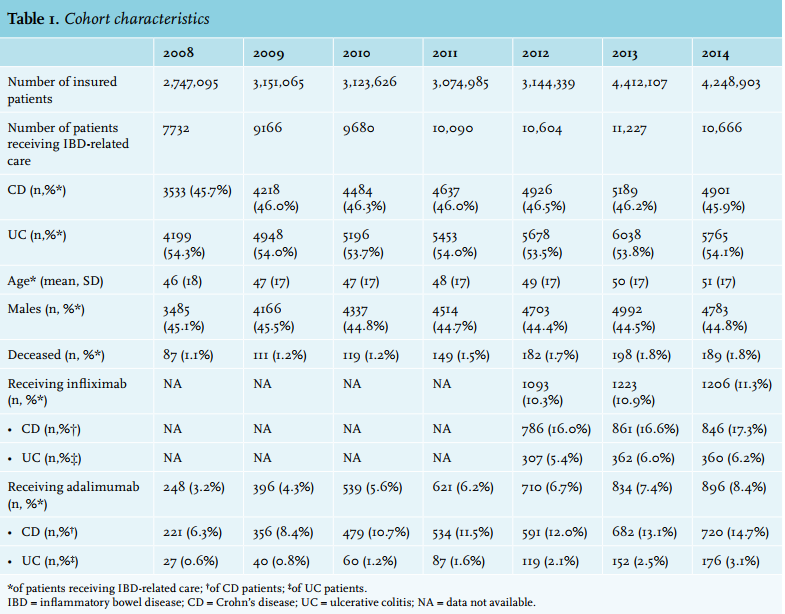
Anti-TNF use
Infliximab
Of the patients receiving IBD-related care, the proportion that were treated with infliximab increased from 10.3% in 2012 to 11.3% in 2014. In these patients, yearly drug costs of infliximab treatment were € 17.4 million in 2012, increasing to € 19.7 million in 2014. At the start of infliximab therapy, the proportion of patients receiving combination therapy was 60.4%, of whom the vast majority received azathioprine (66.5%) or 6-mercaptopurine (26.6%). The proportion of patients receiving combination therapy was comparable in 2012 (59.0%), 2013 (61.0%) and 2014 (61.4%).
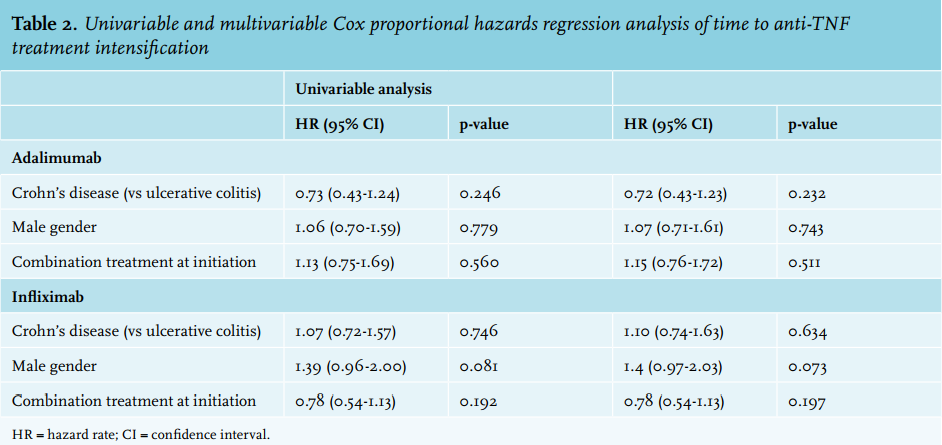
During the observation period, 20,252 infliximab infusions were administered. In total 855 patients (550 Crohn’s disease, 305 ulcerative colitis) started on infliximab within the observation period. The distribution of infliximab administration intervals in these patients over time is shown in figure 1. The proportion of patients receiving infliximab maintenance treatment with an infusion interval between 7 and 9 weeks decreased with longer treatment duration (treatment interval between 7 and 9 weeks at 3 months vs. 24 months: 72.3% vs. 60.9%, p = 0.02). The proportion of patients receiving infliximab with an infusion interval shorter than 7 weeks increased with longer treatment duration (treatment interval < 7 weeks at 3 months vs. 24 months: 22.2% vs. 33.6%, p = 0.01). No clinical factors were significantly associated with time to infliximab intensification (i.e. decreased infusion intervals) in univariable and multivariable analysis (table 2). No change in mean infliximab dose per kg bodyweight was observed over time (3 months vs. 24 months: 5.8 [SD 1.8] vs. 5.7 [SD 2.1], p = 0.64).
Adalimumab
Of patients receiving IBD-related care, the proportion who were treated with adalimumab increased from 3.2% in 2008 to 8.4% in 2014. From 2008 to 2014, 121,406 adalimumab syringes were dispensed with a median of 60 (IQR 28 - 118) syringes per patient. Yearly drug costs of adalimumab treatment increased from € 3.2 million in 2008 to € 13 million in 2014. At the start of adalimumab treatment, the proportion of patients receiving combination therapy was 52.5%, of whom the vast majority received azathioprine (64.4%) or 6-mercaptopurine (18.1%). The proportion of patients starting adalimumab combined with an immunomodulator increased from 42.1% to 51.5% between 2008 and 2014.
A total of 1199 subjects (940 Crohn’s disease, 259 ulcerative colitis) started on adalimumab treatment within the observation period. The distribution of adalimumab administration intervals among these subjects over time is shown in figure 2. The proportion of patients receiving 40 mg adalimumab every other week decreased with longer treatment duration (at 3 months vs. 24 months: 81.5% vs. 71.2%, p < 0.001), whereas the proportion of patients who received intensified adalimumab treatment (i.e. ≥ 40 mg every week) increased with longer treatment duration (at 3 months vs. 24 months: 10.5% vs. 19.3%, p < 0.001). No clinical factors were significantly associated with time to adalimumab intensification in univariable and multivariable analysis (table 2).
Drug survival
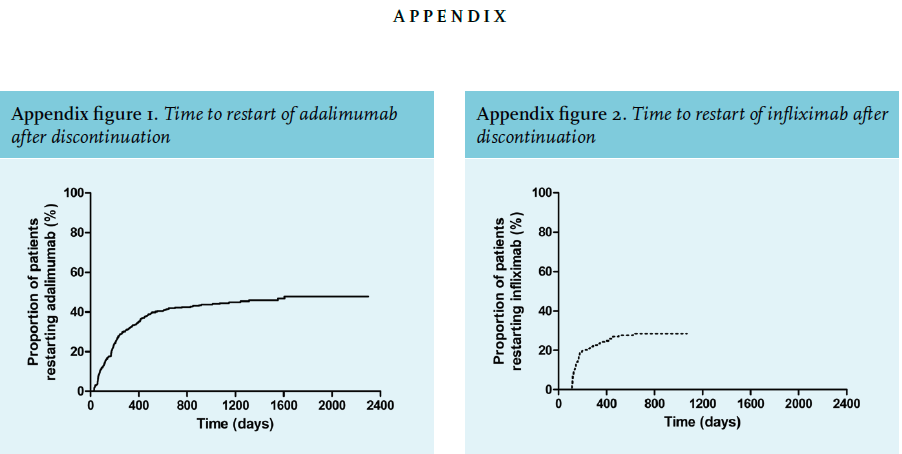
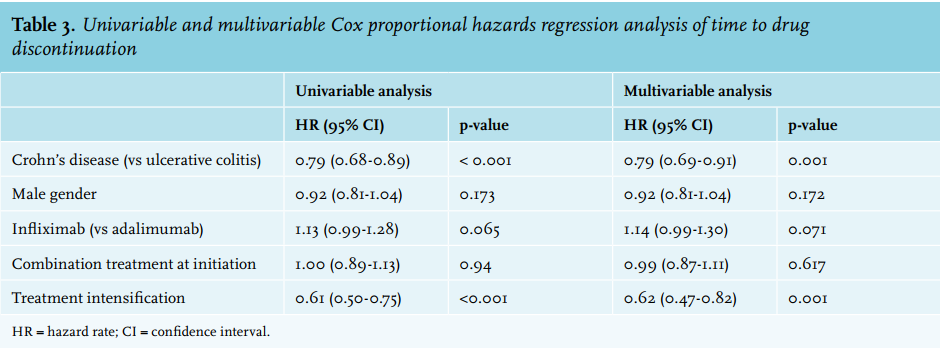
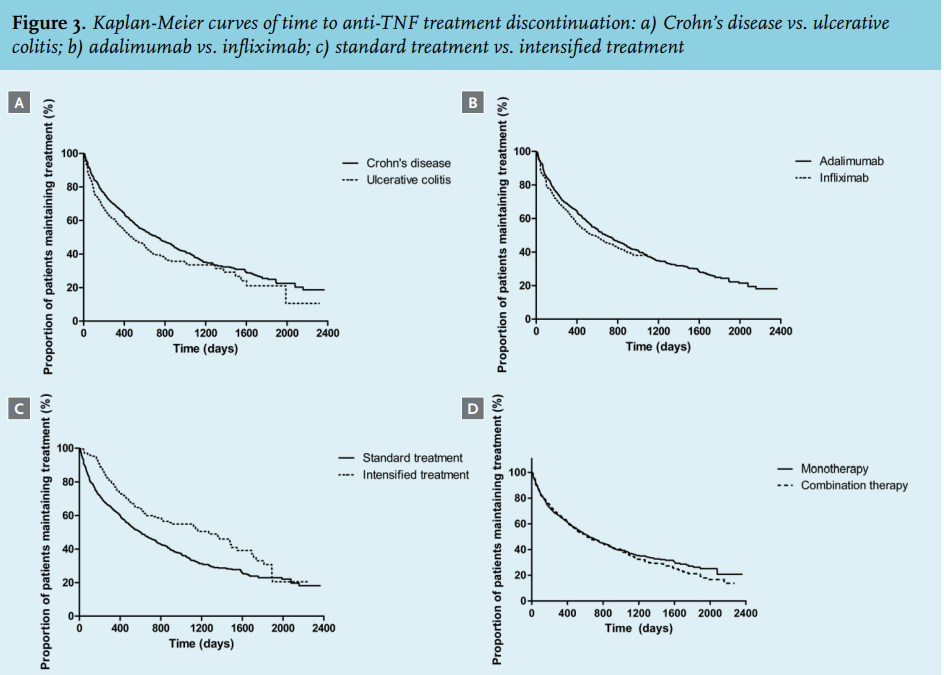
Median time to anti-TNF treatment discontinuation was 600 days (IQR 156-1693 days). At 6, 12 and 24 months after initiation of anti-TNF treatment, the proportion of patients receiving continuous treatment with anti-TNF agents was 72.5% (95% CI 70.5-74.5), 61.5% (95% CI 59.1-63.9) and 45.6% (95% CI 43.1-48.1), respectively. Univariable and multivariable analysis of factors associated with time to drug discontinuation are shown in table 3. Patients with Crohn’s disease were less likely to stop anti-TNF treatment compared with ulcerative colitis patients (hazard ratio [HR] 0.79 [95% CI 0.69-0.91], p = 0.001). Patients who received anti-TNF treatment intensification were less likely to discontinue their treatment (HR 0.62 [95% CI 0.47-0.82], p = 0.001). A trend was observed towards a higher discontinuation rate in patients receiving infliximab compared with adalimumab (HR 1.14 [95% CI 0.99-1.34], p = 0.071). Combination treatment at initiation of anti-TNF therapy was not associated with longer drug survival (HR 0.99 [96% CI 0.87-1.11]). Kaplan-Meier curves of time to anti-TNF discontinuation are shown in figure 3. The proportion of patients who restarted infliximab or adalimumab treatment within 6 months after discontinuation was 19.2% and 21.4%, respectively.
The proportion of patients restarting infliximab and adalimumab within 12 months after cessation of anti-TNF therapy was 24.3% and 33.4%, respectively (Appendix figure 1 and 2). 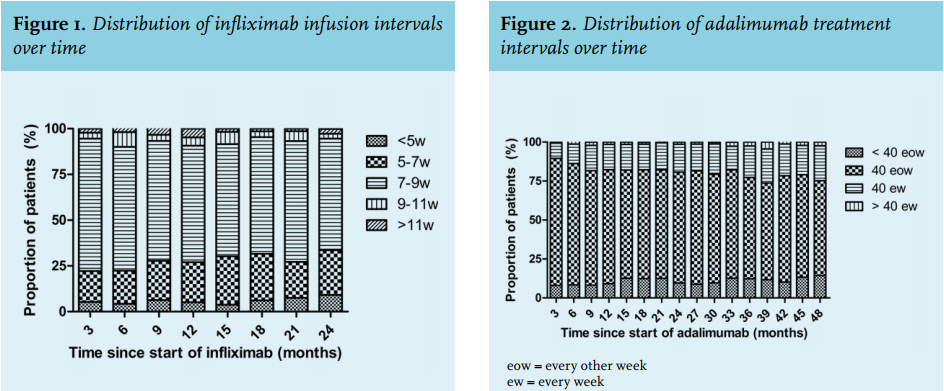
IBD-related hospitalisation
Among patients who started on anti-TNF treatment within the observation period, the cumulative proportion of patients hospitalised for IBD-related problems was 9.2% (95% CI 7.8-10.6), 13.7% (95% CI 11.9-15.5) and 19.8% (95% CI 17.3-22.3), at 6, 12 and 24 months, respectively.
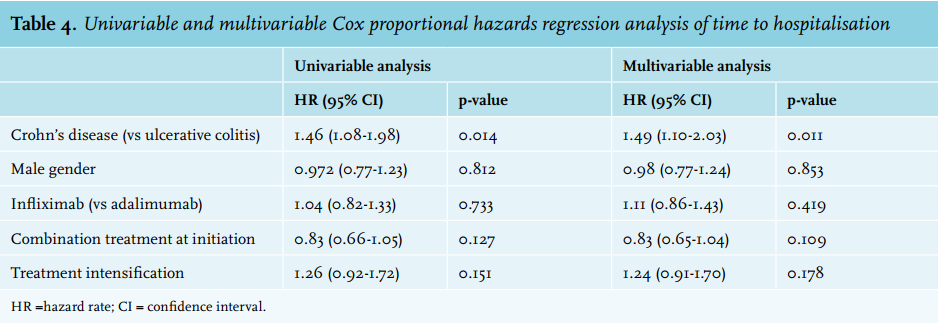
Univariable and multivariable analysis of factors associated with time to hospitalisation is provided in table 4. Crohn’s disease was the only factor that was significantly associated with hospitalisation (HR 1.49 [95% CI 1.10-2.03], p = 0.011). A Kaplan-Meier plot of time to hospitalisation is shown in figure 4. 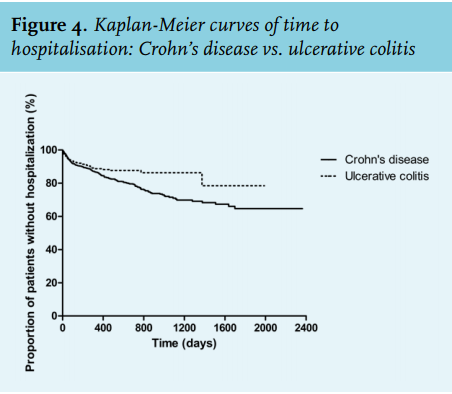
Corticosteroid initiation
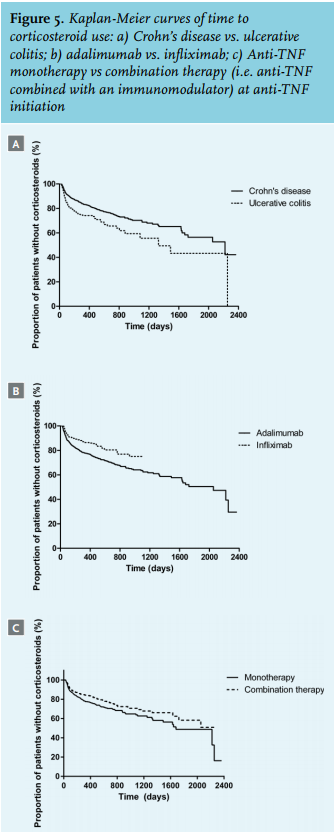
The cumulative proportion of patients receiving corticosteroids after initiation of anti-TNF treatment was 14.4% (95% CI 12.4-16.4), 19.2% (95% CI 16.8-21.6) less likely to receive treatment with corticosteroids. Patients who received combination therapy at the time of initiation of anti-TNF treatment used significantly less corticosteroids as compared with patients receiving anti-TNF monotherapy (HR 0.80 [95% CI 0.64-1.00] p = 0.048). Kaplan-Meier plots of time to corticosteroid initiation are depicted in figure 5.
DISCUSSION
To our knowledge, this study is the first to describe real-life patterns of anti-TNF use and associated treatment outcomes in a large IBD population in the Netherlands. In this cohort of more than 22,000 Crohn’s disease and ulcerative colitis patients, the proportion of patients receiving infliximab or adalimumab increased to approximately 20% in 2014 which accounted for € 32.7 million of drug costs. However, it is important to note that drug costs of anti-TNF therapy decreased substantially after the introduction of biosimilar infliximab in the Netherlands in 2015. Anti-TNF discontinuation occurred in approximately 40% of patients within the first year after treatment initiation and this was associated with a diagnosis of ulcerative colitis, infliximab use and non-intensified anti-TNF treatment regimens. Thus, we show here that the real-life anti-TNF discontinuation rate is substantially higher than previously reported. Moreover, we demonstrate that the proportion of IBD patients receiving intensified anti-TNF treatment gradually increases over time.
Anti-TNF discontinuation rates range from 5% to 23% at 12 months of follow-up according to different studies.8,27 There are several potential explanations for these differences. Firstly, most of these studies concern analyses of clinical trials and tertiary care cohorts,8,10,11 which may not provide reliable estimates of real-life drug survival. Furthermore, early discontinuation (due to primary non-response or intolerance) may not have been included in these estimates. On the other hand, we may have overestimated the discontinuation rate due to the definitions that were applied. These definitions could not account for poor treatment adherence, short drug holidays or episodic treatment strategies. This may also have contributed to a higher proportion of patients restarting the same anti-TNF agent within 12 months (24% and 33% for infliximab and adalimumab, respectively). However, we presume that the number of patients receiving episodic treatment with TNF blockers is very low in this cohort, since it is well known that scheduled continuous treatment is the preferred treatment strategy.
Strikingly, immunomodulator use at the start of anti-TNF treatment was not associated with a longer drug survival or time to anti-TNF intensification. This is an unexpected finding because combination therapy appears to be more effective than either therapeutic agent alone, explained by reduced immunogenicity, increased anti-TNF serum levels and possible synergistic effects.20,28
Nevertheless, several previous studies also found no significant association between time to anti-TNF intensification and concomitant immunomodulator use.29-31 We hypothesise that patients with more severe disease are more likely to receive combination therapy. Consequently, the potential beneficial effect of combination therapy may be neutralised by patients’ poorer prognosis. Furthermore, some patients in our cohort could have been misclassified as patients who started on combination therapy. We defined combination therapy at the time of anti-TNF initiation as a pharmacy dispensation of an immunomodulator in the same semester as the first anti-TNF administration. As a result, some patients may have already discontinued the immunomodulator prior to anti-TNF initiation. However, we did find a significantly longer time to corticosteroid initiation in patients on combination therapy as compared with anti-TNF monotherapy, which reflects the beneficial effect of concomitant immunomodulator use.
A diagnosis of ulcerative colitis was associated with a shorter time to anti-TNF discontinuation and corticosteroid initiation. This could reflect lower response rates to anti-TNF agents in ulcerative colitis compared with Crohn’s disease patients. Although head-to-head studies are lacking, it has been suggested that anti-TNF agents may be more effective in Crohn’s disease as compared with ulcerative colitis.32 In line with this notion, previous studies have found higher rates of anti-TNF treatment intensification in ulcerative colitis compared with Crohn’s disease patients.29-31 A possible explanation for this difference is a higher inflammatory burden and a higher drug clearance in ulcerative colitis patients.19,29,33 However, we did not find a significant association between time to treatment intensification and a diagnosis of ulcerative colitis. Furthermore, other studies found no difference in time to infliximab discontinuation between Crohn’s disease and ulcerative colitis.29
It is currently unclear if infliximab or adalimumab is superior for the treatment of IBD because head-to-head studies are lacking. Results from meta-analyses and several studies show conflicting results.34-41 A population study in IBD patients showed no difference in efficacy between these two agents.40 In our study, infliximab use was associated with a reduced risk of corticosteroid initiation compared with adalimumab. However, the difference in cut-off point between adalimumab and infliximab that we used for time to corticosteroid initiation (an induction period of 4 and 6 weeks, respectively) might have influenced the results. Nevertheless, this finding has also been reported previously in another administrative claims database study that consisted of 1400 ulcerative colitis patients starting anti-TNF therapy.35 Furthermore, no difference in time to hospitalisation was found, and a trend towards a higher drug discontinuation rate was seen in infliximab users compared with adalimumab. We postulate that the small difference in discontinuation rate could be explained by the fact that IBD patients with severe disease requiring hospitalisation are more likely to receive treatment with infliximab.42 Disease severity at the start of anti-TNF treatment could not be assessed in our database, which can cause potential bias for the comparison of the two agents. Hence, based on our results we cannot draw firm conclusions with regard to differences in therapeutic efficacy between infliximab and adalimumab. An ongoing study will determine if higher induction and maintenance doses of adalimumab will improve the outcome in ulcerative colitis patients (NCT02065622).
The present study cohort is a representative sample of the Dutch IBD population, consisting of both second and third line patients. More than 22,000 IBD patients receiving IBD-related care between 2008 and 2014 were included. Long-term data from large population-based cohorts allow for robust analyses of patterns of drug use. However, this study has several limitations. Firstly, adalimumab use was based on the amount of drug that was dispensed by pharmacists to patients. Therefore, actual drug use, premature drug discontinuation, therapeutic compliance and variation in drug dispensing rates because of logistical reasons (such as lost drug) could not be assessed. Secondly, the definitions that were used for patient selection and classification (such as selection of anti-TNF starters, anti-TNF discontinuation, combination therapy, treatment intensification and corticosteroid initiation) may have resulted in selection bias. Thirdly, relevant clinical information such as disease location, behaviour and severity or reasons for anti-TNF discontinuation and corticosteroid initiation could not be obtained. In addition, surgical interventions could not be evaluated since detailed data on IBD-related surgery were not available. Furthermore, the Dutch health insurance claims system does not allow for a diagnosis of unspecified IBD. Consequently, all IBD cases were categorised as either Crohn’s disease or ulcerative colitis, while approximately 8% of the Dutch IBD population is diagnosed with unspecified IBD.43 Despite these limitations, this study contributes to the knowledge on the use of anti-TNF agents and is the first to describe patterns of anti-TNF use in a large real-life population in the Netherlands.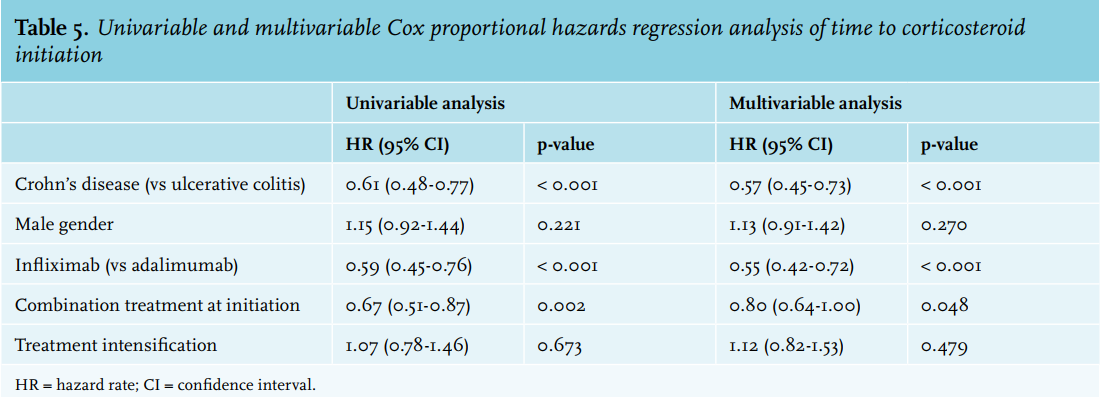
CONCLUSION
The proportion of IBD patients receiving anti-TNF treatment increased to almost 20% in 2014, which is a major cost driver. Discontinuation of anti-TNF agents appears to occur earlier than previously reported, which was associated with a diagnosis of ulcerative colitis and non-intensified anti-TNF treatment regimens, but not with combination therapy. However, immunomodulator use at the start of anti-TNF treatment was associated with a longer time to corticosteroid initiation.
ACKNOWLEDGEMENTS
We thank Hugo Smeets and Anne Hollinga from Achmea healthcare for providing us with the database.
Conference presentations
Part of this work was presented at: Digestive Disease Week 2016, San Diego; ECCO congress 2016, Amsterdam; UEGW 2016, Vienna; ECCO Congress 2017, Barcelona; Digestive Disease Week 2017, Chicago.
DISCLOSURES
S.J.A Bots has served as speaker for Abbvie, Merck, Sharp & Dome, Takeda, Jansen Cilag, Pfizer and Tillots.
C.Y. Ponsioen has served as advisor for Abbvie, Takeda; has received research grants from Takeda; has received speaker’s fees from Abbvie, Takeda, and Dr. Falk Pharma G.R. D’Haens has served as advisor for Abbvie, Ablynx, Amakem, AM Pharma, Avaxia, Biogen, Bristol Meiers Squibb, Boerhinger Ingelheim, Celgene, Celltrion, Cosmo, Covidien, Ferring, DrFALK Pharma, Engene, Galapagos, Gilead, Glaxo Smith Kline, Hospira, Immunic, Johnson and Johnson, Lycera, Medimetrics, Millenium/Takeda, Mitsubishi Pharma, Merck Sharp Dome, Mundipharma, Novonordisk, Pfizer, Prometheus laboratories/Nestle, Protagonist, Receptos, Robarts Clinical Trials, Salix, Sandoz, Setpoint, Shire, Teva, Tigenix, Tillotts, Topivert, Versant and Vifor and received speaker fees from Abbvie, Ferring, Johnson and Johnson, Merck Sharp Dome, Mundipharma, Norgine, Pfizer, Shire, Millenium/Takeda, Tillotts and Vifor.
M. Löwenberg has served as speaker and/or principal investigator for Abbvie, Covidien, Dr. Falk, Ferring Pharmaceuticals, Merck Sharp & Dohme, Receptos, Takeda, Tillotts and Tramedico. He has received research grants from AbbVie, Merck Sharp & Dohme, Achmea healthcare and ZonMW.
The other authors have no potential conflicts of interest to report.
Grant support: No external funding was obtained.
REFERENCES