KEYWORDS
Adverse drug reaction, dasatinib, nephrotic syndrome
INTRODUCTION
Dasatinib (Sprycel®) is indicated in adults for newly diagnosed Philadelphia chromosome-positive (Ph+) chronic myeloid leukaemia (CML), Ph+ acute lymphoblastic leukaemia (ALL) and CML in the chronic, accelerative or blastic phase resistant to previous therapy including imatinib. Dasatinib belongs to the group of protein kinase inhibitors. The mechanism of action is inhibition of BCR-ABL-kinase, kinases from the Src family and several other oncogenetic kinases including c-KIT, ephrin receptor kinases and PDGFβ receptor. Dasatinib was granted marketing authorisation in the Netherlands in 2006.1
CML is a myeloproliferative neoplasm, with in general three disease phases: the chronic phase, the accelerated phase and the blast crisis.2 ALL is a lymphoid neoplasm which shows a progressive disease course, where symptoms may progress over weeks to months with others presenting even more acutely. The Philadelphia (Ph) chromosome refers to a balanced translocation between chromosomes 9 and 22 that can be present in CML and ALL, resulting in BCR-ABL1 fusion, with different breakpoints giving rise to a p190 and p20 protein. Subsequent BCR-ABL1 activity promotes uncontrolled proliferation of transformed cells.2,3
Nephrotic syndrome can have various causes and is defined by the presence of heavy proteinuria (protein excretion > 3.5 g/24 hours), hypoalbuminaemia (< 30 g/l), and peripheral oedema. Proteinuria results from defects in the capillary wall of the glomeruli, which consists of the fenestrated capillary endothelium, the glomerular basement membrane and the podocytes (the epithelial cells in the glomeruli).4
This article describes cases concerning dasatinib associated with nephrotic syndrome from the spontaneous reporting database in the Netherlands maintained by the Netherlands Pharmacovigilance Centre Lareb, the European Pharmacovigilance database EudraVigilance maintained by the European Medicines Agency (EMA), and cases published in scientific literature.
It must be noted that cases from pharmacovigilance databases concern spontaneous reports of possible adverse drug reactions reported by healthcare professionals, manufacturers, patients or others, and the likelihood of a causal relationship can differ between cases.
CASE SERIES
The detailed cases are described below. A summary of the cases is listed in table 1.
Case received by Lareb
The Netherlands Pharmacovigilance Centre Lareb received one report of nephrotic syndrome with the use of dasatinib,5 after initial treatment with imatinib which was poorly tolerated (muscle and joint pain). The patient was a male in the age group 11-20 years with Ph+ ALL, who developed nephrotic syndrome (oedema with a weight gain of 6 kg, proteinuria with a protein-creatinine ratio 126.7 mg/mmol, and hypoalbuminaemia with a blood albumin of 12 g/l), 27 days after starting dasatinib 60 mg/m2 once daily. Dasatinib was withdrawn and fluid intake restricted. One week after withdrawal of dasatinib the patient had recovered from the nephrotic syndrome. Previous treatment included cytarabine and mercaptopurine; the Dutch summaries of product characteristics (SmPCs) for these drugs do not report nephrotic syndrome or proteinuria as adverse reactions.6,7 No other potential causes were identified either. After dasatinib was withdrawn the patient was switched back to imatinib and nephrotic syndrome has not recurred since.
EudraVigilance cases
The European Pharmacovigilance database EudraVigilance contained another seven strongly supportive cases of dasatinib associated with nephrotic syndrome. All seven cases concerned female patients. One case was a patient under the age of 18 years, the other cases were all adults. The mean age was 42 years. The latencies varied from about one month to seven months and one patient had a longer latency of almost five years. In one case latency was not reported. In six cases dasatinib was withdrawn and in one case the dose was decreased. Six patients recovered or were recovering from the reaction at the moment of reporting, and in one report the outcome was unknown. In one case it was reported that slight recovery after temporary interruption of dasatinib was followed by recurrence of the reaction after resumption of dasatinib, and again by recovery after withdrawal of dasatinib. In one patient treatment other than withdrawal of dasatinib for the nephrotic syndrome was reported. In two reports results from renal biopsy were specifically described: in one case focal segmental glomerulosclerosis was seen and in one case focal and segmented hyalinosis. In one report membranous glomerulonephritis was reported as reaction without mentioning whether this was biopsy-proven.12
Cases in scientific literature
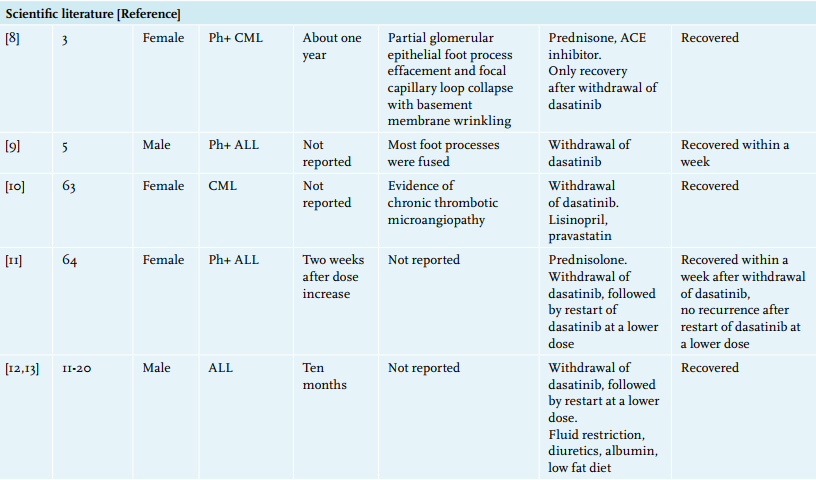
The scientific literature describes five other patients with nephrotic syndrome associated with dasatinib use.
A nine-month-old girl was diagnosed with Ph+ CML. She was treated with imatinib for a year and was then switched to dasatinib 60 mg/m2 because of BCR-ABL positivity. At the age of three years she developed nephrotic syndrome. Electron microscopy of a renal biopsy showed partial glomerular epithelial foot process effacement and focal capillary loop collapse with basement membrane wrinkling. She was treated and the reaction improved, but the patient only recovered from the reaction after withdrawal of dasatinib.8
A five-year-old boy with Ph+ ALL developed nephrotic syndrome 26 days after haematopoietic stem cell transplantation while using dasatinib (dose not reported). At electron microscopy most podocytes foot processes were fused, which could indicate minimal change disease. Within a week after withdrawal of dasatinib, the nephrotic syndrome resolved.9
A 63-year-old woman with CML experienced nephrotic-range proteinuria, while using dasatinib 100 mg/day. Kidney biopsy showed evidence of chronic thrombotic microangiopathy. The patient recovered from the proteinuria after switching to imatinib.10
A 64-year-old woman with Ph+ ALL used dasatinib in addition to a regimen of chemotherapy comprising cyclophosphamide, daunorubicin, vincristine, prednisolone, methotrexate, cytarabine and dexamethasone. Two weeks after the dose of dasatinib was increased from 110 mg to 140 mg daily, she developed nephrotic syndrome. After withdrawal of dasatinib the nephrotic syndrome resolved within a week. Dasatinib was restarted in a lower dose of 70 mg daily without recurrence of nephrotic syndrome.11
One literature case was described in the EudraVigilance database, but the original article was not available through PubMed. This case concerned a male in the age group 11-20 years with Salmonella sepsis and nephrotic syndrome receiving treatment with dasatinib 60 mg/m2 for ALL with a latency of ten months. The reaction was treated with fluid restriction, diuretics and albumin infusions. Five weeks later the patient developed chylothorax. Dasatinib was withdrawn and a low-fat diet was started. Within two weeks, the chylothorax resolved. Dasatinib was restarted at a reduced dose of 48 mg/m2 /day instead of 60 mg/m2 without recurrence of nephrotic syndrome and chylothorax.12,13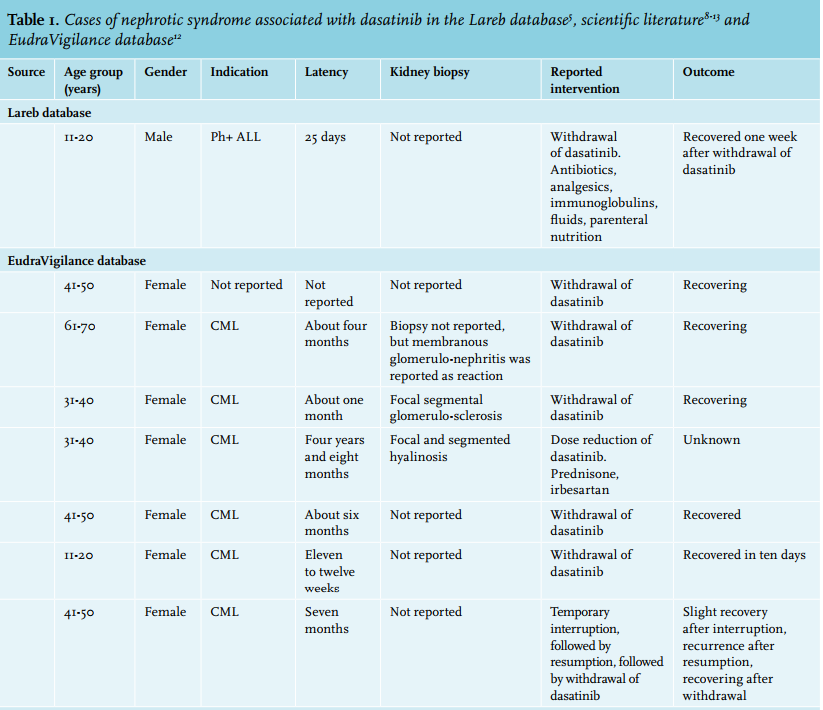
DISCUSSION
A possible mechanism of how dasatinib might cause nephrotic syndrome is disruption of the vascular endothelial growth factor (VEGF) signalling pathway through inhibition of the Src family kinases, one of the targets of dasatinib. VEGF expression occurs in human podocytes and is involved in maintaining normal glomerular function.10 Disrupting VEGF signalling through therapy targeting VEGF or through inhibition of the VEGF receptors is associated with minimal change nephrotic syndrome which may evolve to focal and segmental glomerulosclerosis, and thrombotic microangiopathy in the glomerular and peritubular capillaries.14 Proteinuria after inhibition of VEGF signalling is considered a dose-related side effect.15
The Dutch SmPC for dasatinib mentions proteinuria as a sometimes occurring adverse reaction and nephrotic syndrome was also recently added to the list of adverse reactions, with unknown frequency of occurrence.1 In the Dutch SmPCs of the Src family kinase inhibitor bosutinib and the BCR-ABL kinase inhibitors imatinib, nilotinib and ponatinib, neither nephrotic syndrome nor proteinuria are mentioned as adverse reactions.16-19 Concerning other tyrosine kinase inhibitors nephrotic syndrome is a labelled adverse reaction for sorafenib and sunitinib, both drugs with therapeutic targets that include VEGF receptors.20,21 Based on the report received by Lareb, the other cases in EudraVigilance and the cases described in the scientific literature, supported by a possible mechanism, it is suggested that dasatinib might cause nephrotic syndrome. Nephrotic syndrome was recently added to the list of adverse drug reactions in the Dutch SmPC for dasatinib.
It is important to realise that when a patient develops nephrotic syndrome while on therapy with dasatinib, this may concern an adverse drug reaction of dasatinib.
DISCLOSURES
CMZ declares research collaboration with Novartis, BMS and Pfizer for paediatric development of tyrosine kinases. The other authors have no conflicts of interest to declare.
DISCLAIMER
The authors are indebted to the national pharmacovigilance centres that contributed data to the EudraVigilance database, maintained by the European Medicines Agency (EMA). The opinions and conclusions, however, are not those of the various centres, nor of the EMA. The information originates from a variety of sources, and the likelihood that the suspected adverse reaction is drug related can vary between cases.
REFERENCES