KEYWORDS
Mycobacterium tuberculosis, donor-derived, liver transplantation
INTRODUCTION
Donor-derived infections remain a challenge after solid organ transplantation because screening of post-mortal donors is not possible for all potential pathogens. Whereas transmission of pathogens such as cytomegalovirus and Epstein-Barr virus is a known and accepted risk, other infections may be transmitted unexpectedly. Although the incidence of donor-derived infections is low at approximately 0.2%, recipient mortality may be as high as 25%.1,2 We present a case of donor-derived tuberculosis after liver transplantation, in which the donor origin of the Mycobacterium tuberculosis isolate could be demonstrated by DNA fingerprinting.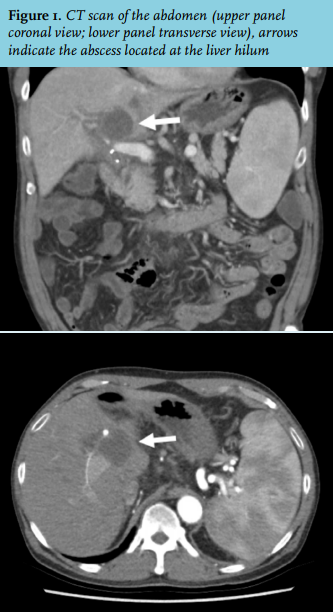
CASE REPORT
A 70-year-old man, born in Suriname, was referred to our centre with rapidly progressive liver failure. His medical history consisted of recent cholecystitis, treated conservatively with amoxicillin-clavulanic acid. On admission, the Model for End-Stage Liver Disease (MELD) score was 23. Further workup excluded infectious, hereditary, vascular and autoimmune disorders. During pre-transplant screening, a tuberculin skin test and interferon gamma release assay (Quantiferon-TB Gold in-tube®) were both negative and chest radiography showed no abnormalities.
Due to progressive liver failure, the patient underwent orthotopic liver transplantation in November 2013. The donor was a 57-year-old woman from the Philippines who suffered from a lethal brain injury after a complicated resection of a pituitary adenoma. Histopathology of the recipient’s explanted liver showed nodular regenerative hyperplasia and bland cholestasis, suggesting drug-induced liver injury as the cause of liver failure. Maintenance immunosuppression consisted of prednisolone and tacrolimus.
Six months post-transplantation the patient developed fever without other symptoms. A CT scan showed a mass of 3.3 × 3.7 cm in the liver hilum with portal vein thrombosis due to compression (figure 1). A diagnostic aspiration yielded pus. The Gram stain showed 5-20 leukocytes and 0-5 Gram-positive rods per high power field. Additional Ziehl-Neelsen staining showed +4 acid fast bacilli and a PCR for M. tuberculosis (MTB) complex (in-house, IS6110 target) was positive. Culture for common aerobic and anaerobic bacteria remained negative.
Since 1993, in the Netherlands all MTB isolates are routinely fingerprinted for epidemiological purposes at the Tuberculosis Reference Laboratory. Based on spoligotyping, the MTB isolate found in the present case was characteristic of the Manilla genotype family, which is commonly found in immigrants originating from the Philippines.3 Based on the genotype, characteristic of the donor’s origin, it was concluded that the infection was probably donor-derived. During pre-transplant screening of the donor, abdominal ultrasound and chest radiography showed no abnormalities. No tests for latent tuberculosis had been performed. The infection was reported to Eurotransplant. To date, the recipients of the kidneys and pancreas of the same donor have not developed tuberculosis.
Treatment consisted of isoniazid, ethambutol, pyrazinamide and levofloxacin and a portal stent was placed. Rifampicin was not used because of the interaction with tacrolimus. The isolate was later found to be fully susceptible. Pyrazinamide was discontinued after five weeks because of rising uric acid levels and levofloxacin was discontinued after seven weeks because the patient wanted to resume running. It was planned to treat him for 18 months. However, after eight months of treatment the serum aminotransferases were elevated (SGOT 229 IU/l, SGPT 553 IU/l). The tuberculosis therapy was discontinued followed by normalisation of the liver enzymes. Because imaging showed complete resolution of the abscess, the treatment was not resumed and the patient remained well, the follow-up time being 29 months at the time of this writing.
DISCUSSION
Infections are among the most frequent complications after solid organ transplantation. They can be categorised as a manifestation of pre-existing chronic infection in the recipient, a reactivation of latent infection in the recipient, a donor-derived infection or as exogenous de novo infection. The percentage of infections that are donor-derived varies in different reports.4,5
The incidence of tuberculosis in solid organ transplant recipients is higher than in the general population.6,7 The differentiation between endogenous reactivation and donor-derived infection can be difficult. A donor origin is very likely if infection is only localised in the transplanted organ or if multiple recipients from the same donor develop tuberculosis with an identical isolate.
Donor-derived tuberculosis from a liver transplant is rare, with only a few published cases.8-10 In contrast to the lack of proof in those reports, the donor origin of the infection in our patient was deducted from the MTB fingerprint in combination with the donor origin from the Philippines, where that specific MTB genotype was known to circulate. While post-transplant tuberculosis is notorious for poor graft and patient survival, the early diagnosis with only localised disease probably contributed to a favourable outcome.11
Potential organ donors are thoroughly screened to reduce the risk of transmission of infections. Eurotransplant guidelines prescribe which information is required to minimalise this risk. Specific screening of living donors for latent tuberculosis is possible, although there is debate on the value of such screening and the need for treatment.12 In case of post-mortal donors, screening for tuberculosis with skin testing is generally not feasible and the donor origin, a history of past tuberculosis or exposure and chest radiography have a very limited sensitivity for latent tuberculosis. Screening with a tuberculosis-specific interferon gamma release assay, which only requires a fresh blood sample, could be useful.12
The treatment of tuberculosis in transplant recipients can be challenging due to drug interactions and significant toxicity. According to current guidelines, treatment should be based on epidemiology and drug resistance.13
Treatment with a rifamycin is generally avoided because of interactions with calcineurin inhibitors and mTOR inhibitors. If a rifamycin is nevertheless used, the dose of immunosuppressive drugs has to be increased with close monitoring of drug levels. Significant hepatotoxicity can occur, especially when combining several hepatotoxic drugs including pyrazinamide, rifampicin and isoniazid.14,15 Consultation with a tuberculosis expert is always indicated in case of post-transplantation tuberculosis.
CONCLUSION
This case with donor-derived tuberculosis after liver transplantation illustrates that donors originating from high tuberculosis endemic countries may transmit tuberculosis via a transplanted liver, although this is probably very rare. The early diagnosis probably contributed to the favourable outcome in our patient.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES