KEYWORDS
Compression ultrasound, superficial vein thrombosis, residual thrombosis, venous malformation, venous thromboembolism
INTRODUCTION
Venous malformations (VMs) are the most prevalent vascular anomalies, with an incidence of almost 2% in the general population. The slow-flow, thin-walled vascular lesions present as bluish or purple lesions, which are mainly localised on the skin and mucosa, but can be found in any tissue or organ. Most of the lesions are asymptomatic, although swelling and pain can occur.1,2
Coagulation abnormalities associated with VMs of the extremities are reported as localised intravascular coagulation and are characterised by elevated D-dimer levels. Severe localised intravascular coagulation is associated with elevated D-dimer and low fibrinogen levels. The severity of the activated coagulation state is related to the extent of the malformation.3,4 Thrombosis may present as a local superficial thrombosis or palpable phlebolith, a stone-like structure due to calcification of the thrombus. VMs usually occur in a pure form; however they can also be part of more complex syndromes, such as the Klippel-Trenaunay syndrome, a low-flow VM of the capillary, venous and lymphatic systems, characterised by a triad of port-wine stains of the affected extremity, and bony and soft tissue hypertrophy. The prevalence of venous thromboembolism in patients with Klippel-Trenaunay syndrome is high (approximately 20%).5,6 The prevalence of venous thromboembolism in patients with pure VM is, however, unknown. Similar to patients with Klippel-Trenaunay syndrome, blood stagnation with activation of coagulation within the distorted, enlarged venous blood vessels is also present in patients with pure VMs. It is therefore conceivable that patients with pure VMs similarly have an increased risk of thrombotic complications, such as extension of the superficial vein thrombosis or venous thromboembolism.3,7 If this is the case, venous thromboembolism could be more common in these patients than presently assumed.
The objectives of this study are 1) to determine the prevalence of superficial vein thrombosis and/or venous thromboembolism, and 2) to assess whether patients with pure VM have a hypercoagulable state.
METHODS
We performed a cross-sectional study among patients with pure VM.
Population
The study population consisted of outpatients of the Department of Plastic, Reconstructive and Hand Surgery, at the Academic Medical Center, Amsterdam, the Netherlands, included between May 2009 and July 2012. Patients were consecutively asked to participate after their elective visit, regardless of whether symptoms of thrombosis were present. Inclusion criteria were patients aged ≥ 12 years with a pure VM. Patients with an VM other than a pure VM, such as patients with Klippel-Trenaunay syndrome, or with a maximum surface area of less than 4 cm2 with an estimated depth less than 4 cm or patients who refused informed consent were not eligible. The institutional review board approved the study protocol and written informed consent was obtained from all included patients.
Demographic and clinical data were collected, such as age, gender, and details of the symptomatic episodes of the VM. The patient’s medical history was carefully considered for a history of thrombotic and major bleeding events, use of anticoagulant therapy and risks for thrombosis such as immobilisation within four weeks prior to inclusion, surgery in the last three months, use of oral contraception, pregnancy or an active malignancy. If prior venous thromboembolism was reported, a copy of the original investigation (ultrasound, CT scan, or other imaging study) was collected. If prior major bleeding was reported, we did not register it specifically, since bleeding was not a predefined outcome of this study.
We did not perform MRI for study purposes. However, when an MRI was performed in patients < 18 years of age within one year prior to enrolment or in patients ≥ 18 years within five years prior to enrolment, the MRI result was used to estimate the surface area of the VM, in combination with physical examination. If no MRI was available, only physical examination was used to estimate the surface area. In case of multiple VMs, we measured the largest malformation to estimate the surface area of the VM.
Compression ultrasonography (CUS)
Flow characteristics of the VM and signs of superficial or deep vein thrombosis or residual thrombosis in the VM were obtained by CUS, performed by one of in total three experienced sonographers. They used the same criteria for thrombosis and residual thrombosis. In case of the latter, another sonographer and one of the researchers were contacted to reach consensus. The CUS was performed on the affected parts of the body after collecting the clinical data, such as current symptoms of thrombosis. If, after physical examination, thrombosis was suspected in a limb not affected by a VM, CUS of that limb was performed as well.
Vein compression was performed in the transverse plane; vein diameter was measured during maximal compression and was expressed in millimetres.
Because this study had a cross-sectional design, we could only compare the results with previous CUS if patients had ever had a thrombosis. In these cases the CUS findings were categorised according to Prandoni and colleagues8 as negative for deep vein thrombosis or recurrence if both the veins were fully compressible or, in the non-compressible veins, if the residual vein diameter was reduced or unchanged (± 1 mm), compared with the previous assessment; positive for proximal deep vein thrombosis recurrence if a previously normal vein had become non-compressible or if the residual vein diameter in either venous segment had increased in size (> 2 mm) compared with the previous assessment.
If patients had no history of thrombosis, we considered the CUS negative if the veins were fully compressible, and positive for deep vein thrombosis if a vein had become non-compressible or if the residual vein diameter in either venous segment was enlarged (> 2 mm). Furthermore, we made an arbitrary distinction between residual thrombosis and ‘fresh’ thrombi, depending on the density (old thrombi usually have a larger density compared with fresh thrombi), contour (old thrombi are mostly re-canalised and have lost their irregular shape) and the presence of calcifications or bypasses.
Because this is not a standardised method to report residual thrombus, we reported all CUS findings. Depending on the localisation of the clots, we classified thrombosis as superficial vein thrombosis or deep vein thrombosis.
Coagulation parameters
Blood samples were collected in citrated tubes (Becton Dickinson, San Jose, CA), and centrifuged within 30 minutes for 20 minutes at 1700 g and 15 °C, the plasma was re-centrifuged for 15 minutes at 3000 g and 15 °C. Plasma was stored at -80 °C.
Activated partial thromboplastin time (APTT) and prothrombin time were determined as indicators of the intrinsic and extrinsic pathways, respectively. We also measured D-dimer, a marker of fibrin clot formation and fibrinolysis, Von Willebrand factor, a marker of endothelial activation and involved in the adhesion and aggregation of platelets, and P-selectin, an adhesion receptor on activated platelets for monocytes. The coagulation assays, APTT and prothrombin time, were performed on an automated coagulation analyser (Behring Coagulation System, BCS) with reagents and protocols from the manufacturer (Siemens Healthcare Diagnostics, Marburg, Germany). Von Willebrand factor and P-selectin antigen levels were determined by ELISA using antibodies from Dako (Glostrup, Denmark) and Human SP-selectin/CD62P (R&D Systems), respectively. D-dimer was determined with Innovance D-dimer (Siemens Healthcare Diagnostics).
Statistical analysis
All numbers are expressed as medians with corresponding interquartile ranges (IQR) or ranges, unless otherwise stated. The Mann-Whitney U test was used for nonparametric numeric data; the chi square test was used for categorical data. Statistical analysis was performed using statistical software (SPSS 19.0.2, SPSS, Chicago, IL). Statistical difference was set at p < 0.05. 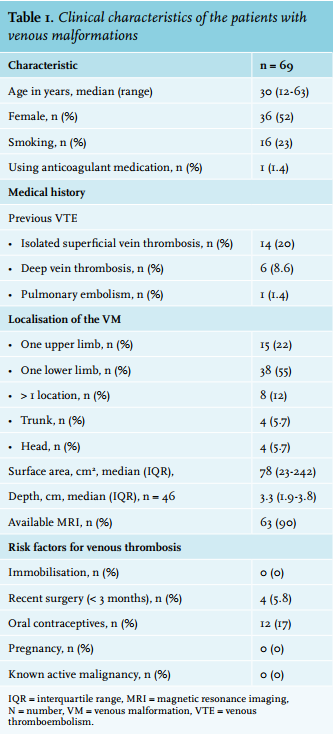
RESULTS
In total 70 patients with pure VM were eligible for the present analysis. One patient was shown to have no VM left after he underwent surgery, so this patient was excluded. The clinical and VM characteristics of the remaining 69 patients are described in table 1. Median age was 30 (range 12-63) years and 36 (52%) patients were female. The median estimated surface area of the VMs was 78 cm2 (IQR 18-240, range 3.4-645 cm2 ). The lesions were localised in the following anatomical regions: head and neck (n = 4, 6%), one arm (n = 15, 22%), one leg (n = 38, 55%), trunk (n = 4, 6%), and in more than one region (n = 8, 12%).
A total of 20 patients had a proven previous thrombotic event: 14 patients (20%) had superficial venous thrombosis and 6 patients (8.6%) had a documented venous thromboembolism (6 patients had deep vein thrombosis 1 of whom also had proven pulmonary embolism). The deep vein thrombosis had been located in the region of the VM in 4 of the 6 patients with previous deep vein thrombosis; in the remaining patients the location of the thrombus was not related to the VM.
Nine patients (13%) were using medicine that can affect coagulation: 7 NSAIDs, 1 aspirin and 1 a vitamin K antagonist (phenprocoumon). This last patient was excluded from analysis of the coagulation parameters. None of the patients reported major bleeding in their medical history.
A total of 63 patients (92%) reported intra-lesional pain and/or swelling of the VM. Frequency of the pain episodes ranged from daily (n = 12, 17%) to once a year (n = 3, 4.3%).
In 78% of the cases, the pain was provoked by physical activity, pressure on the VM, change in temperature, stress or a combination of these factors. None of the patients had symptoms of thrombosis at the time of inclusion, although 40% of the included patients reported their usual, mild chronic pain. The mean and the median intensity of the pain were 1.7 and 0 (scale 0-10) respectively. The surface area of the VM was not related to the severity or frequency of localised pain, neither was the pain correlated to superficial or deep vein thrombosis or a thrombotic event in the past.
Compression ultrasound
A total of 68 out of 69 patients had a CUS result; 1 patient was not able to undergo CUS, because he fainted during blood sampling. Of the 68 remaining patients, 1 patient was using anticoagulant therapy for only a short period. This patient had twice had a deep vein thrombosis; we therefore did not exclude this patient from the CUS analysis. In these 68 patients, superficial vein thrombosis was observed in 10 (15%) cases, in 1 patient an older previously unknown muscle vein thrombosis was found and in another patient asymptomatic deep vein thrombosis was diagnosed (table 2). None of the patients with thrombosis, deep vein or superficial, had undergone recent surgery.
Residual thrombosis was observed in 16 patients (24%). In 9 of the 20 patients with a history of a thrombotic event, a residual thrombosis was seen with CUS (table 2).
Of the 48 patients with no history of thrombosis, 7 patients had current thrombosis and 7 patients had residual thrombosis on CUS (table 2). Hence, in total 29% (14/48) patients either had asymptomatic thrombosis or residual thrombosis on CUS or an older thrombosis which had not been recognised as such by either the patient or physician. None of the patients with thrombosis or residual thrombosis used anticoagulation therapy and 1 of these patients had undergone surgery within the last three months.
When combining the results of medical history and CUS, 34 out of 69 patients (49%) had either a history or current signs of a thrombotic event: 20 patients had a medical history of documented superficial or venous thromboembolism (6 patients with deep vein thrombosis, 1 of whom had documented pulmonary embolism), and 14 patients without a history of thrombosis had current thrombosis or residual thrombosis on CUS. In total, 7 patients in the study population (10%) had venous thromboembolism either in their medical history or at the moment of CUS examination (table 2). No relation was found between the size or location of VM and the presence or history of superficial vein thrombosis or venous thromboembolism.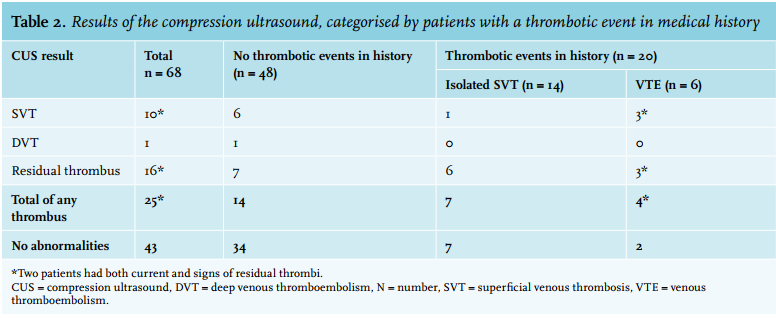
Coagulation parameters
The levels of the coagulation parameters of 67 of the 69 included patients are listed in table 3: 1 patient was using phenprocoumon and 1 patient had no CUS result. In order to evaluate whether coagulation parameters differed between patients with and without current thrombosis, patients were categorised by CUS results showing thrombosis (n = 11) or no thrombosis (n = 56) on CUS, regardless the presence of residual thrombosis or whether the thrombosis was deep or superficial.
Median D-dimer level was 0.57 mg/l (IQR 0.3-1.2, range 0.17-16.1). A total of 37 patients (51%) had a D-dimer level above 0.5 mg/l, the usual cut-off level to exclude thrombosis in combination with a clinical decision rule in patients younger than 50 years.9 Patients with a superficial vein thrombosis or deep vein thrombosis on CUS had similar median D-dimer levels compared with those without, 0.57 versus 0.55 respectively (p = 0.64). The D-dimer levels above the 75th percentile ranged from 1.2-16.1 µg/l. We found a clear association between D-dimer levels and extent of the VM (Spearman’s r = 0.50, p < 0.0001). Median P-selectin level was 29 ng/ml (IQR 21.5-34.0). Patients with a history of either superficial or venous thromboembolism had a significantly higher median P-selectin level compared with patients with no history of thrombosis (34 ng/l versus 25 ng/l, p < 0.001), whereas the mean age in both groups was comparable (32 years, p = 0.9). A significant correlation was also observed between the surface area of the VM and the level of P-selectin (Spearman’s r = 0.53, p < 0.0001). However, the P-selectin levels in the group of VM patients with thrombosis observed on CUS were comparable to those without thrombosis on CUS (p = 0.27) (table 3). The median plasma Von Willebrand antigen level was in the middle of the normal range, and the number of patients with a level below 50% was 3 with a median Von Willebrand antigen of 43% (range 29-45).
Because to our knowledge the influence of residual thrombosis on coagulation parameters is uncertain, we additionally categorised patients into neither current thrombi nor residual thrombosis (n = 42) and patients with current and/or signs of residual thrombosis (n = 25). This categorisation gave comparable results for the median D-dimer and Von Willebrand antigen level (table 3). However, median (IQR) P-selectin levels were significantly higher in patients with a residual, superficial vein thrombosis or deep vein thrombosis on CUS 32 ng/ml (24-48) versus 26 (20-33) in patients with no thrombosis (p = 0.03).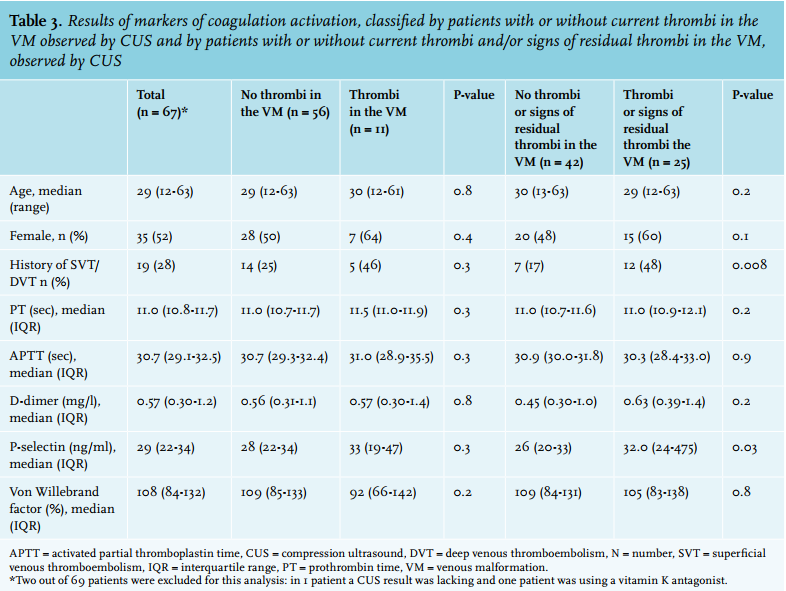
DISCUSSION
In this cohort of patients with pure VM we observed that almost half of the patients had either a history of thrombosis or current signs of a thrombotic event, including superficial vein thrombosis and deep venous thromboembolism. Furthermore, in patients without a thrombotic event in their medical history, CUS showed the presence of thrombosis or residual thrombosis on CUS in 14/48 (29%), which may indicate that many thrombotic events happen asymptomatically.This number of patients with asymptomatic events is higher than the 5.5% (95% confidence interval, 3.1-9.5%) in the normal population.10 Also the number of previous or current venous thromboembolisms (7/69, 10%) is higher than what may be expected for a cohort of patients with a median age of 30 years. In the normal population the incidence rate of venous thromboembolism is 0.005% in childhood to nearly 0.5-0.4% in patients aged 60-64 years.11,12 The number of patients with any superficial vein thrombosis was also much higher. This is relevant since superficial vein thrombosis may extend and progress to deep vein thrombosis.13 The median D-dimer level was higher than 0.5 mg/l, the usual cut-off value to exclude thrombosis in the normal population younger than 50 years,9 while some patients had very high levels. We only had a few patients with a low Von Willebrand factor. Finally, D-dimer values and P-selectin were clearly related to the extent of the VMs, suggesting the bigger the VM, the more coagulable.
Until now, only a few studies have addressed the coagulation parameters of patients with pure VM. The D-dimer level in patients with pure VM was investigated in two studies14,15 and the rates of a D-dimer level higher than 0.5 mg/ were 43% and 58%, respectively, which is comparable with the rate of 53% in our study. Oduber and colleagues16 quantified the frequency of venous thromboembolism in a cohort of 75 patients with Klippel-Trenaunay syndrome (median age 24) with CUS. Additionally, they performed a case-control study to evaluate whether coagulation alterations were related to venous thromboembolism and magnitude of VMs. A total of 29 (39%) patients had signs of current or previous venous thromboembolism, including superficial venous thrombosis, and 6 (8%) had ever had venous thromboembolism, comparable with our cohort of pure VM. Compared with the age-matched controls (n = 105, median age 33 years) D-dimer levels were also higher: 0.46 mg/l (IQR 0.27-3.84) versus 0.27 mg/l (IQR 0.20-0.36) and comparable with our median of 0.54 mg/l. The extent of the vascular malformations on MRI was, similar to our results, positively correlated with D-dimer plasma levels (r = 0.33; p < 0.05). Other studies have demonstrated that high plasma levels of soluble P-selectin are strongly associated with venous thromboembolism.17-20 In our cohort, P-selectin levels were higher in patients with thrombi compared with patients with no thrombi in their VM; nevertheless, this difference did not reach significance. The shift towards significance in patients with thrombosis or residual thrombosis versus patients with no thrombosis is probably due to power. The patient with current deep vein thrombosis observed on CUS, however, had a high P-selectin level of 57 ng/ml, suggesting that platelet activation in VM only occurs in case of deep venous or superficial thrombosis.
Some aspects of the study require comment. First, we did not perform MRI in this study and we could only determine the size of the VM and the tissue types involved of the 63 patients (91%) who underwent an MRI for clinical reasons before inclusion. Second, we did not recruit a matched control group of patients without VM, Klippel-Trenaunay syndrome or thrombosis to compare our results with. However, the laboratory results may be compared with the results of Oduber and colleagues,16 since they used a control group which was comparable to our cohort and used similar laboratory assays. Furthermore, due to practical issues, we did not standardly perform CUS of all limbs irrespective of the location of the VM. Consequently, we may have even underestimated the number of asymptomatic thrombotic events. Moreover, patients were asked to participate after their elective visit to the plastic surgery outpatient clinic, regardless of their current complaints. We did not, however, report an exclusion list of patients who were not able to participate, which may have masked an inclusion bias. Also, our results should be interpreted with caution because of the moderate sample size. Last, the distinction between thrombosis and residual thrombosis is arbitrary. The definition of residual thrombosis, made by Prandoni et al.8 was in patients with proven deep vein thrombosis in contrast to our cross-sectional design in a high-risk group for thrombosis. However, we think this distinction makes our interpretation a more accurate reflection of clinical practice, because residual and fresh thrombi have a different appearance on CUS. Because of this arbitrary distinction, we have shown all the data. We consider that this is more complete than only reporting the new thrombi. When we performed analyses including and excluding residual thrombosis our main findings did not change. However, this arbitrary distinction makes our results less generalisable. And, although the interobserver concordance rate of residual vein thrombosis on CUS is high (κ = 0.92),21 the interobserver reliability in the measurement of residual thrombosis in VMs is unknown. In conclusion, superficial vein thrombosis and venous thromboembolism are common in this cohort of apparently healthy and young patients with pure VM and a significant proportion of these patients have high D-dimer levels. Treating physicians should be aware of this, especially in those pure VM patients with exposure to risk factors for venous thromboembolism.
ACKNOWLEDGEMENTS
We would like to thank A. Terpstra, M. Pannekoek and E. Althuizen from the department of radiology for performing all the compression ultrasounds.
DISCLOSURES
There are no conflicts of interests to disclose.
REFERENCES