KEYWORDS
Cost-management, insulin therapy, liraglutide, type 2 diabetes, weight gain
INTRODUCTION
Insulin treatment is frequently needed to maintain glucose control in patients with type 2 diabetes, but often at the expense of pronounced insulin-associated weight gain.1,2 Average weight gain has been estimated at 2 kg per 1% (13 mmol/mol) drop in HbA1c, but can be much higher (up to 5% of the body weight or more) in individual cases.1 Such weight gain is obviously undesirable in an already overweight population, leads to a more unfavourable cardiometabolic profile, and may offset the beneficial effects of better glucose control.3
Glucagon-like peptide-1 (GLP-1) receptor agonists are a relatively new class of glucose-lowering agents that also induce weight loss.4 They can be used as an adjunct to diet, in combination with oral drugs and in combination with insulin.5,6 However, treatment with GLP-1 receptor agonists is expensive and many healthcare systems have limited their reimbursement.7-9 In individual cases, where more commonly used treatments fail or lead to significant side effects, GLP-1 receptor agonists may be a suitable treatment alternative. In the Effect of Liraglutide on insulin-associated wEight GAiN in patients with Type 2 diabetes (ELEGANT) trial, we showed that addition of the GLP-1 receptor agonist liraglutide reversed body weight, decreased insulin requirements and improved glycaemic control in patients with type 2 diabetes who had pronounced weight gain after the initiation of insulin.10,11 Approximately 40% of patients lost all the body weight gained after initiating insulin and 20% of patients were able to stop insulin therapy completely.
While addition of GLP-1 receptor agonists increases direct treatment costs, costs associated with insulin therapy such as glucose monitoring and hypoglycaemia decrease.6,12 Because liraglutide also reduces the incidence of cardiovascular disease and death,13 indirect costs may decrease as well. As not all patients respond to treatment with GLP-1 receptor agonists, extra costs may be further reduced by early selection of patients with a positive response, allowing timely discontinuation in non-responders. The aim of the present study was to determine the best cost-controlling treatment strategy for additional GLP-1 receptor agonist treatment in patients with type 2 diabetes and pronounced insulin-associated weight gain: the shortest possible trial period while yielding the highest number of effectively treated patients.
MATERIALS AND METHODS
A simulation model was developed using data from the ELEGANT randomised controlled trial, which was conducted in the Netherlands between February 2012 and April 2014.10,11 The methods of this trial have been described previously. Briefly, patients with type 2 diabetes who had shown pronounced (≥ 4% of body weight) weight gain between 3 and 16 months after the initiation of insulin therapy were randomised either to addition of liraglutide (1.2 or 1.8 mg) to insulin therapy or to continuation of standard insulin therapy for 26 weeks. The study had a waiting-list design so that patients who initially continued insulin therapy from 0-26 weeks, which was uptitrated when necessary to achieve treatment targets, were also offered liraglutide treatment from 26-52 weeks. As clinical effects of liraglutide treatment were similar for both groups of patients,11 we pooled the 26-week data on liraglutide-insulin combination therapy from the entire study population (n = 47). These data were compared with the 26-week data from the group of patients initially randomised to continuation and uptitration of standard insulin therapy (n = 24), and used for the simulation model to calculate 8, 12, 16 and 26-week health outcomes.
Study protocol
After inclusion, participants in the ELEGANT trial were evaluated every 4-6 weeks (study visits at 0, 4, 8, 12, 16, 20 and 26 weeks) for adverse events, hypoglycaemia, body weight and insulin dose, and every 8 weeks for HbA1c (determined at 0, 8, 16 and 26 weeks). Liraglutide was initiated at 0.6 mg/day and increased over two weeks to 1.8 mg/day. When adverse events occurred, participants were allowed to return to the 1.2 mg dose. When liraglutide was started, the total insulin dose was decreased by 20% to avoid hypoglycaemia. Participants were instructed to perform daily (4-point) capillary blood glucose profiles during the first 3 weeks after the start of liraglutide, and twice weekly thereafter. Patients who continued standard insulin treatment were instructed to perform capillary blood glucose profiles at their own discretion, but at least once weekly. At every study visit, the insulin dose was adjusted aiming for a fasting glucose target of 4.0-6.5 mmol/l. The dose of oral glucose-lowering agents (metformin and sulphonylurea) remained unchanged unless hypoglycaemia persisted after the discontinuation of insulin.
Simulation model structure
The model was developed as a decision tree that compared health outcomes within a treatment period of 26 weeks consisting of: 1) continuation and uptitration of standard insulin therapy, or 2) liraglutide 1.2-1.8 mg once daily added to standard insulin therapy (figure 1). The second treatment strategy could result in three different scenarios: a) adverse events, prompting the discontinuation of liraglutide; b) ineffectiveness of the therapy (not meeting treatment targets) without adverse events, which should also lead to discontinuation of liraglutide; or c) effectiveness of the therapy, justifying the continuation of liraglutide from a clinical point of view. Effectiveness was defined as achieving at least two of the following treatment targets after 26 weeks of liraglutide treatment: 1) ≥ 4% weight loss, and/or 2) HbA1c ≤ 53 mmol/mol (7%), and/or 3) discontinuation of insulin therapy without adverse events. Key events and changes in therapy over the 26-week treatment period included changes in insulin dose, uptitration of liraglutide to the maximum tolerable dose (1.2 or 1.8 mg), treatment discontinuation due to adverse events (trial-based: at 4 weeks and within 12 weeks), and failure to achieve treatment targets regarding weight loss, HbA1c and discontinuation of insulin therapy.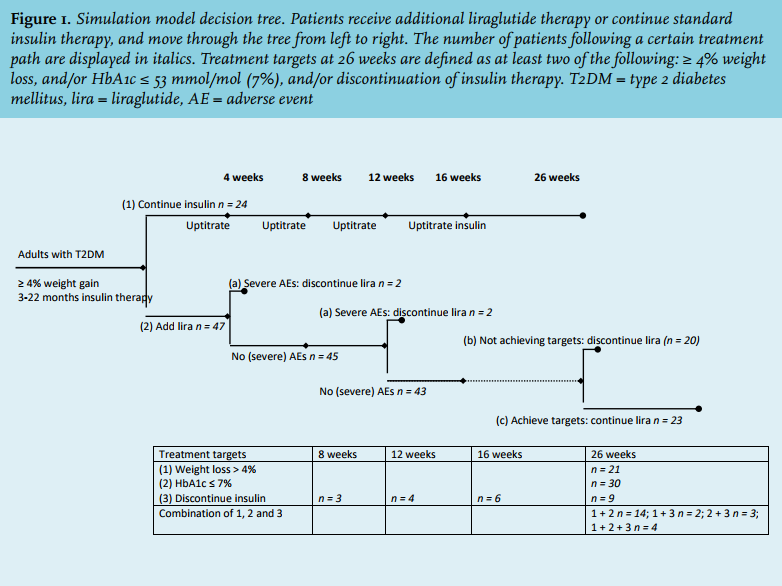
Model inputs
Model inputs were derived from the ELEGANT trial; medical expenditure inputs were derived from pharmacy costs (Zorginstituut Nederland9), as explained below. Costs were defined from a health care perspective, societal costs were excluded.
Effectiveness of liraglutide and insulin use
Effectiveness inputs and patient flow including drop-out rates for the use of liraglutide and/or insulin were derived from the ELEGANT trial (figure 1 and table 1). Treatment efficacy was evaluated based on body weight, HbA1c, and insulin dose.
Treatment costs
Direct medical expenditure, consisting of medicationrelated costs (insulin, liraglutide, needles, and test strips needed to perform daily self-measured capillary blood glucose profiles), was derived from pharmacy costs (Zorginstituut Nederland9) and evaluated at 8, 12, 16 and 26 weeks.
Nine of 47 (~1/5) patients were on a liraglutide dose of 1.2 mg, so that the average liraglutide dose for all patients was 1.7 mg (at ~€ 2.83 per mg). For insulin, we calculated the average costs per unit of insulin, based on the insulin regimens that were used by the trial participants: 54% used basal insulin only (~€ 0.037 per unit); 34% were on basal-bolus regimens (~€ 0.033 per unit); and 12% were on biphasic insulin (~€ 0.027 per unit). This translated into € 0.034 per unit of insulin. The change in insulin dose (units per day) for each participant and treatment group was derived from the ELEGANT trial and included the 20% decrease in insulin dose when liraglutide was started. We assumed a 100% adherence for both liraglutide and insulin, while on treatment.
We assumed that injection needle costs increased with one additional needle (~€ 0.20 per needle) per day after the start of liraglutide, and were reduced by two needles per day after the discontinuation of insulin. Patients used disposable test strips for performing self-measured capillary blood glucose profiles (~€ 0.50 per strip). Following the study protocol, 28 strips per week were used in the first 3 weeks after the start of liraglutide to perform daily (4-point) capillary blood glucose profiles, and eight strips per week thereafter. We assumed that patients continuing standard insulin therapy used four strips per week and that patients who could discontinue insulin therapy no longer performed blood glucose profiles.
We did not model costs related to the use of metformin and sulfonylurea. Also, we did not include the costs associated with a visit to the doctor or laboratory in the model, as these were the same for patients in both groups.
Treatment discontinuation and adverse effects
In the ELEGANT trial, 4 of 47 (8.5%) patients discontinued liraglutide due to adverse effects. We assumed that two patients stopping liraglutide within 4 weeks incurred drug costs for 28 days, and those stopping later (within 8 and 9 weeks) incurred drug costs for 12 weeks of treatment, but not with any additional costs. We also assumed return to baseline levels of insulin dose, HbA1c, and body weight in patients who discontinued therapy. Two of 24 patients (8.3%) who were initially assigned continuation of standard insulin treatment withdrew consent after 1 and 10 weeks of follow-up, respectively, both of whom are included in the present analysis.
We did not take into account costs related to adverse effects. Although particularly gastrointestinal adverse effects occurred more frequently with liraglutide than with standard insulin therapy (52.8% versus 8.3%), they were mostly mild-to-moderate in severity, typically resolved after 4-8 weeks, and did not lead to hospital admission, increased medication costs or unscheduled outpatient visits. As hypoglycaemia rates did not differ between the two groups,10,11 we did not incorporate hypoglycaemia into our model either. 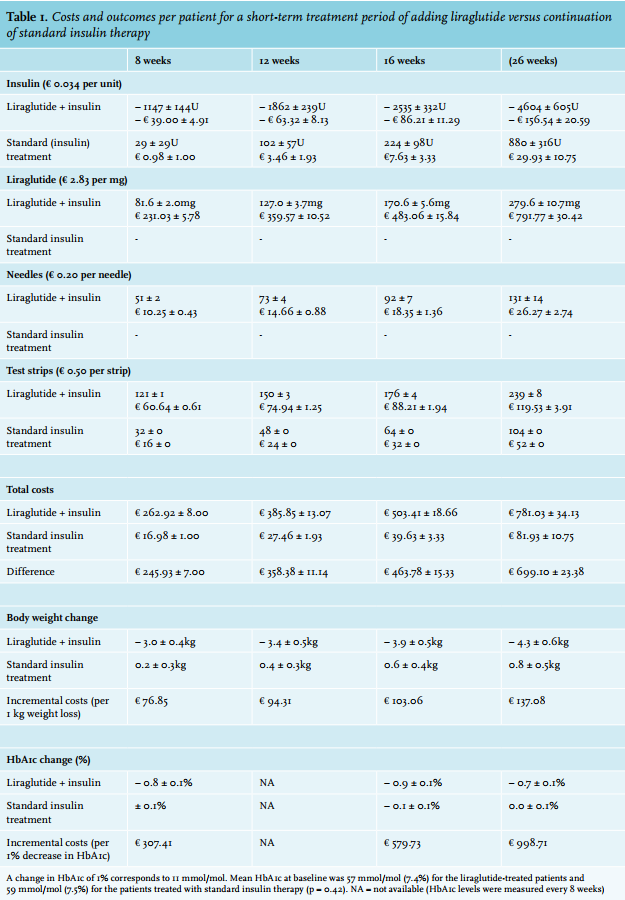
Model outcomes
The simulation model was used to answer the following questions. First, the total costs of adding liraglutide to insulin for 26 weeks were calculated, on the basis of intention to treat. Then, we calculated costs associated with a trial period of 8, 12 or 16 weeks of adding liraglutide to existing insulin therapy, as compared with continuation and uptitration of standard insulin therapy. Second, the incremental costs (ICER = incremental cost-effectiveness ratio) per 1 kg weight loss and per 1% decrease in HbA1c were calculated. Third, several thresholds regarding weight loss (in %), change in HbA1c, and reduction in insulin dose (in %) at 8, 12 and 16 weeks were explored, to predict if a patient would meet the predefined treatment targets after 26 weeks of liraglutide treatment. We assumed that patients who would not meet these targets discontinued liraglutide treatment. These calculations were performed to find the shortest possible trial period that would yield the highest number of successfully treated patients and the lowest number of patients not meeting treatment success, translating into the lowest costs per successfully treated patient.
Statistical analyses
All statistical analyses were performed using SPSS (IBM SPSS Statistics for Windows, Version 20.0, IBM Corp, Armonk, NY). Missing data were imputed according to last-observation-carried-forward. As both groups were comparable at baseline regarding insulin regimen (both 2.1 insulin injections per day) and insulin dose (55.6 ± 34.9 units/day for liraglutide arm, 50.0 ± 32.9 units/day for standard insulin therapy, p = 0.51), we used raw data to calculate treatment costs, not using a linear mixed model. Results for subgroups were tested for normal distribution and are displayed as mean ± standard error.
RESULTS
Figure 1 represents the simulation model, including the number of participants in the ELEGANT trial assigned to a certain treatment, dropping out, and achieving the predefined treatment targets of ≥ 4% weight loss, HbA1c ≤ 53 mmol/mol (7%) and discontinuation of insulin after 26 weeks of treatment. In total, 23 out of 47 patients achieved at least two of these treatment targets.
Costs of additional liraglutide treatment
The additional costs of adding liraglutide to insulin treatment in the ELEGANT trial amounted to € 246 per patient after 8 weeks of treatment, and € 699 per patient after the full 26 weeks of treatment, as compared with continuation and uptitration of standard insulin therapy (table 1). As liraglutide reduced body weight by -4.3 ± 0.6 kg, the ICER for a 1 kg reduction in body weight was € 137; the ICER for a 1% decrease in HbA1c was € 999 (table 1). These costs are spent in all patients, including non-responders.
Early predictors of treatment success at 26 weeks
Figure 2 represents changes in body weight, HbA1c or insulin dose at 8, 12 and 16 weeks for responders (patients meeting at least two of the predefined treatment targets at 26 weeks) and non-responders. An early weight loss of 2.5-3% was a strong indicator of long-term treatment success, whereas a change in HbA1c did not differentiate between responders and non-responders, neither at 8 nor at 16 weeks. The best treatment strategy for controlling costs, using weight change only, was to discontinue liraglutide after a treatment period of 8 weeks in patients showing less than 3% weight loss. This strategy would erroneously include four non-responders and exclude five responders not yet identified as such. At the 8-week time point, three of these five responders showed a more than 60% reduction in insulin dose. Consequently, a strategy based on a mixed criterion of either ≥ 3% weight loss or ≥ 60% decrease in insulin dose at 8 weeks would be more cost-controlling, correctly identifying 21 of 23 responders, whilst four non-responders would be treated ‘erroneously’ until week 26. Using such an 8-week trial period as a go/ no-go decision point would correspond to a sensitivity of 91%, specificity of 83%, positive predictive value of 84% and negative predictive value of 91%.
Treatment costs for the best cost-controlling treatment strategy
Application of ≥ 3% weight loss or ≥ 60% reduction in insulin dose at 8 weeks as early response criteria, with discontinuation of liraglutide in those not meeting one of these targets, would decrease additional treatment costs for the whole group of 47 patients from € 32,858 to € 22,888 for a period of 26 weeks, saving € 9970, or € 453 per non-responding patient. As costs for the 8-week trial period amount to € 246 per non-responder, total costs per effectively treated patient would decrease from € 1429 to € 1079 for the first 26 weeks with this strategy. After 26 weeks, the additional costs for liraglutide treatment are € 957 for 6 months, assuming that the insulin dose will not change.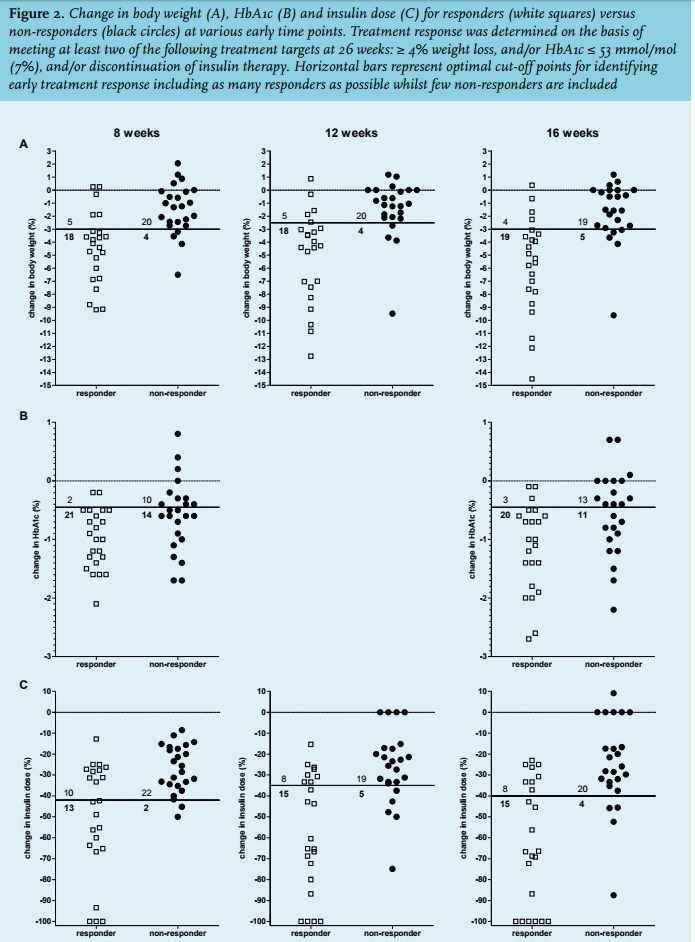
DISCUSSION
The present analysis of the ELEGANT trial shows that the addition of liraglutide to insulin treatment is associated with an additional cost of ~€ 700 for 26 weeks, or ~€ 140 per 1 kg weight loss, but that the total costs per effectively treated patient would decrease by € 350 for the first 26 weeks when liraglutide is discontinued after an 8-week trial period in patients not showing an early response. Early response, defined by either ≥ 3% weight loss or ≥ 60% decrease in insulin dose, had high positive and negative predictive values for treatment response after 26 weeks. The costs of this 8-week trial period are ~€ 250 for one patient. The analysis in this study may help in cost-controlling clinical decision-making by selecting those patients who are most likely to benefit from addition of a GLP-1 receptor agonist to insulin therapy.
Reimbursement for treatment with GLP-1 receptor agonists is limited because it is considered expensive.7,14 On the other hand, GLP-1 receptor agonist treatment may also yield indirect cost-savings: less hypoglycaemia, a decreased need for glucose monitoring, and cost-savings associated with improved glycaemic control, weight loss, simplification of diabetes treatment and potentially less cardiovascular complications.13,15 The present analysis only calculated direct costs associated with a relatively short treatment period of adding liraglutide to insulin. Replication in an independent cohort is necessary to reinforce our results. A complete cost-benefit analysis is complex and contains many undetermined factors, including a possible increase in costs on the longer term due to additional life years gained.
Earlier studies have assessed the cost-effectiveness of GLP-1 receptor agonists in general and of liraglutide in particular, but mainly in comparison with other glucoselowering therapies.12,16,17 The evidence review group from NICE reported an estimated cost-effectiveness of £ 15,130 per quality adjusted life year (QALY) for liraglutide 1.8 mg compared with insulin glargine.18 The investigators conducted additional sensitivity analyses and concluded that the factors that carried most weight in the comparison with glargine were the direct utility effects of body mass index changes and systolic blood pressure, underlining the significance of body weight. One other study assessed the cost-effectiveness of adding a GLP-1 receptor agonist to insulin and showed that the addition of lixisenatide to basal insulin treatment was associated with increased QALYs and reduced lifetime healthcare costs as compared with the addition of bolus insulin.19 These results support our previously reported findings of improved quality of life with liraglutide.11 Because liraglutide is more effective in weight loss and lowering HbA1c than lixisenatide,20,21 its potential benefits are greater. Nevertheless, outcomes of cost-efficiency calculations are largely dependent on assumptions regarding long-term benefits.22 While our treatment strategy yields less direct costs, our data can determine neither potential gain in QALYs nor their costs.
In this study, the cut-off points chosen can be regarded as arbitrary, but they were based on clinical reasoning. Thus, we chose the HbA1c cut-point as this is still the most widely recommended glycaemic target for patients with type 2 diabetes,5 and stopping of insulin because of its implications for daily management. A 4% weight loss was chosen because this was the average weight gain in patients starting on insulin treatment.2 In a recent study among patients with type 2 diabetes, a gain in body weight of ≥ 5% was associated with a 14% increase in medical costs, when glycaemic control was suboptimal (HbA1c ≥ 53 mmol/mol [7%]).23 Some may consider the clinical impact of 4% weight loss to be limited, but a minimal weight reduction of 3-5% in obese participants is already associated with a clinically relevant improvement in cardiometabolic health.3,24,25 Moreover, weight loss is considered to be very important by patients and is associated with higher treatment satisfaction, better treatment adherence and a healthier lifestyle.26-28
In the present analysis we have used quite strict criteria in defining treatment success. Current guidelines advise to aim for less strict treatment targets, especially concerning HbA1c in elderly people.5 The NICE guidelines define a beneficial response to GLP-1 receptor agonists as an HbA1c reduction of at least 11 mmol/mol (1%) or a weight loss of at least 3% after 26 weeks of treatment.8 Although one of the four ‘non-responders’ at 8 weeks in our trial stopped treatment because of adverse events, the three remaining subjects all had clinical responses at week 26 that many clinicians would view as clinically relevant. One 64-year old patient showed a 6.5% weight loss with a stable HbA1c of 58 mmol/mol (7.5%), another patient showed a 2.2% weight loss in combination with an 8.7 mmol/mol (0.8%) decrease in HbA1c and the third patient lost 3.9% of body weight and had an HbA1c decrease of 14 mmol/mol (1.3%). Surely, less strict targets could be applied, but such would result in more people being eligible for treatment, thereby increasing overall treatment costs.
Our findings extend those of a previous study on the predictive value of short-term weight loss with a GLP-1 receptor agonist to a more generic good response in the longer term and an earlier decision time point. Subgroup analyses of the SCALE diabetes trial, in which overweight or obese patients with diabetes were treated with liraglutide 3.0 mg, showed that an early (within 16 weeks) loss of > 5% of initial body weight with liraglutide was a good predictor of clinically meaningful weight loss after one year of treatment.29,30 In the present analysis, we show that the weight response after 8 weeks of such treatment may suffice and not only predicts a good weight but also a good glycaemic effect (either reduction of HbA1c or cessation of insulin therapy). This time point may aid the clinician in making treatment decisions with respect to continuation or discontinuation of GLP-1 receptor agonists. HbA1c did not discriminate between responders and non-responders, which might be explained by the relatively low HbA1c at baseline, the study protocol that was aimed at reducing body weight rather than HbA1c, and the fact that time is needed for HbA1c to respond. As current guidelines, such as the NICE guideline, mostly advocate a trial period for GLP-1 receptor agonists of 26 weeks,8 our approach would lead to a substantial decrease in costs.
The strength of the present analysis is that we were able to calculate additional treatment costs in a real-life situation, which might be helpful in clinical decision-making. Our strategy to select patients with prominent treatment responses that are likely to translate into long-term clinical benefit was associated with ~€ 1100 per successfully treated patient for the first 6 months and ~€ 1900 for each treatment year thereafter. The present analysis also has limitations. Our model includes several assumptions that may affect outcomes. For example, the current assumption of needing four test strips per week probably underestimated the actual use of strips, particularly in patients assigned to continuing standard insulin therapy on premixed or basal-bolus insulin regimens. None of these patients could simplify insulin treatment, which contrasts with three patients in the liraglutide group who simplified from basal-bolus to basal insulin alone. We also did not consider the drop in costs associated with the cessation of oral glucose-lowering agents in five patients on liraglutide versus none in the standard insulin group. Neither did we model the costs associated with adverse gastrointestinal events. Although these were mild to moderate and of relatively short duration, we cannot fully exclude loss of labour productivity and absence from work. These side effects should be balanced with the reduced risk of hypoglycaemia relative to better glycaemic control with GLP-1 receptor agonist treatment, which is also associated with substantial direct and indirect medical costs.31 Only one severe adverse event (myocardial infarction) occurred, which was deemed unrelated to the study drug. We were not able to identify lifelong costs, which may change as cardiovascular outcome improves,13,15 and as the effects of liraglutide on body weight and decrease in HbA1c tend to diminish over time. Finally, the analysis was based on selected patients who may not necessarily be representative for the entire diabetes population.
In conclusion, an 8-week trial period of adding liraglutide to insulin in patients with pronounced insulin-associated weight gain is a good strategy to control costs, when patients not showing ≥ 3% weight loss or ≥ 60% decrease in insulin dose discontinue such treatment. With prolonged treatment, costs are likely to decrease further due to a reduction in long-term diabetes complications mediated by weight loss and better glycaemic control.
ACKNOWLEDGEMENTS
We would like to thank Matthijs Versteegh, Institute for Medical Technology Assessment, Erasmus University of Rotterdam, the Netherlands, for his helpful comments regarding the manuscript.
DISCLOSURES
The ELEGANT trial was an investigator-initiated trial that was funded in part by Novo Nordisk B.V. (Alphen aan den Rijn, the Netherlands). Novo Nordisk also provided the medication. Novo Nordisk had no role in the design of the ELEGANT trial, or the collection, management, analysis and interpretation of the data and also no role in the present analysis, the writing of this manuscript or the decision to submit the paper for publication.
B.E. de Galan served as a consultant for Novo Nordisk and received a research grant from Astra-Zeneca. C.J. Tack has received research grants, served as a consultant for, or gave lectures organised by AstraZeneca and Novo Nordisk. The remaining authors declare that they have no conflicts of interest.
REFERENCES