KEYWORDS
Atypical illness presentation, elderly patients, emergency department.
INTRODUCTION
Older patients are a growing demographic in our healthcare system. The emergency department is one of the places where this can be encountered. In the emergency department, 12 to 43% of the patients are elderly.1-3 They visit the emergency department more frequently, with more urgent diseases, need more diagnostics and stay longer. Furthermore, they have a greater chance of being hospitalised and being misdiagnosed.1,3-6 Atypical presentation of illness could be the cause of misdiagnosis.
Presentation with well-known and highly prevalent atypical symptoms (e.g. immobility, impaired cognition and incontinence) is often referred to as geriatric syndromes.7 There is no gold standard definition for an atypical presentation of illness. Common presentations include altered mental state, failure to eat and drink, failure to develop fever, lack of pain, functional decline, reduced mobility, falling, fatigue and urinary incontinence.8 Limpawattana et al. defined atypical illness presentation as patients with no signs and symptoms or unusual signs and symptoms, unrelated to or even the opposite of what is usually expected.
It is known that the geriatric population often have with an altered clinical presentation.9,10 Moreover atypical presentation of illness seems to be an independent predictor of poor hospital outcome.9,11 Early recognition and management of atypical presentation potentially results in positive health outcomes by prompting accurate diagnosis, reducing the risk of new comorbidities, reducing hospital length of stay, and improving quality of life.12
Since little research has been carried out in this area, we conducted a monocentric retrospective observational study on 355 elderly patients presenting to the emergency department. We investigated the prevalence and clinical outcome of atypical presentations of illness among elderly patients in order to assess the clinical relevance of this categorisation.
MATERIALS AND METHODS
Setting and design
This retrospective observational study was conducted in Medical Center Slotervaart, Amsterdam. This is a large urban teaching hospital with 310 beds. Approximately 14,000 patients are admitted to the emergency department per year. The study was approved by the Medical Ethics Committee of the MC Slotervaart.
Patients
All patients of 80 years and older admitted to the emergency department between 1 June 2013 and 7 May 2014 were eligible for study inclusion. We reduced the size of the group by including only patients who were admitted to the emergency department in the first seven days of every month during this study period.
Data collection
Data were extracted from the electronic patient data management system: age, gender, communication difficulties, living situation, amount of medication, use of psychoactive drugs, triage colour (red: in need of immediate medical attention, orange: in need of delayed medical attention, yellow: in need of minimum medical attention), subsequent hospitalisation, history of dementia or mild cognitive impairment (according DSM-IV-TR), main reason of admission, history of falling, new urine incontinence, functional decline and cognitive decline prior to admission, Charlson comorbidity index, highest delirium observation score, decubitus during hospitalisation, length of stay on the emergency department, length of stay in hospital, referral to a care institution, and date of death.
To obtain survival data at one year after admission, we contacted general practitioners and nursing homes.
Definition
If the anamnesis in the emergency department included the usual symptoms of the underlying disease, it was defined as a typical illness presentation. If the anamnesis in the emergency department revealed none of the symptoms known for the underlying disease (e.g. lack of fever, dysuria and frequency in case of urinary tract infection, or lack of fever, coughing and dyspnoea in case of pneumonia), and/or the presentation was preceded by a geriatric syndrome (falling, new urine incontinence, functional decline or cognitive decline) with a known or unknown cause, it was also defined as atypical illness presentation. There was a second assessor (FvdH) to independently assess all patients for type of presentation. When no agreement was reached, a third assessor (CT) defined the category.
Statistical analysis
Analyses were performed using SPSS version 23 (SPSS, Inc., Chicago, IL). Patients with missing data were excluded from the relevant analyses. Outcome variables were categorised into atypical and typical presentations of illness. The chi-squared test was used to compare univariate associations between categorical variables. The Student’s t-test was used to compare continuous variables. For statistical comparison of the mean, the Mann-Whitney U test was used. For all tests a p-value of < 0.05 (two-tailed test) was considered to be significant. The interrater reliability for type of presentation was 0.92 (95% CI 0.87-0.96), evaluated with Cohen’s kappa statistic.
RESULTS
A total of 355 patients were included. Table 1 presents the baseline characteristics of the study population. The mean age was 86 years, and the proportion of female patients was 60%. Before admission 80% lived at home. A cognitive disorder was present in 30% and approximately the same number had communication problems. The median Charlson comorbidity index before admission was 2. Approximately half of the patients were triaged yellow. Neurological disease (15%), infectious disease (16%) and fracture (12%) were the most frequent causes of the visit to the emergency department.
In 53% of the patients there was an atypical presentation of the illness; 29 patients (15%) showed none of the usual symptoms for the underlying disease in the anamnesis. A cognitive disorder was present in 21 of these 29 patients without symptoms.
In 99% of the atypical presentations the patient had a geriatric syndrome, with falling by far the most frequent symptom (71%). New urine incontinence was seen in 3%, functional decline in 11% and cognitive decline in 29%. In 66% of these cases the cause of the geriatric syndrome was clear (figure 1).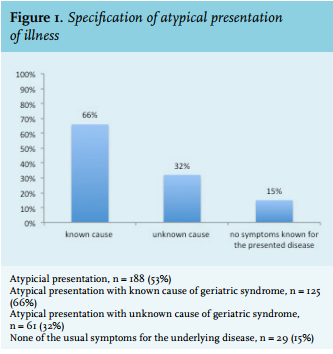
Patients with atypical presentations were significantly older (p = 0.000), more often resided in a care institution (p = 0.005), had higher rates of cognitive disorders (p = 0.001) and more frequently experienced problems with communication (p = 0.000).
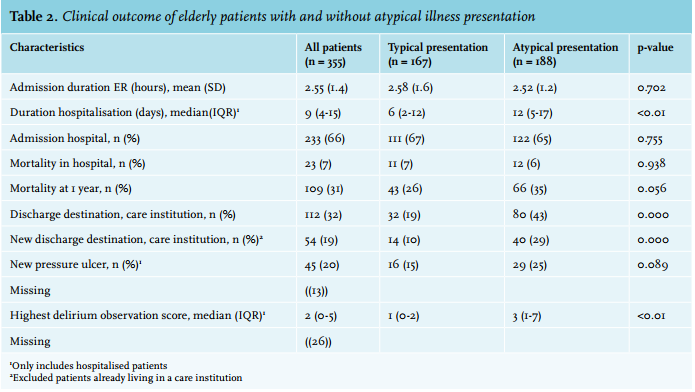
Compared with patients with a typical illness presentation, patients with an atypical presentation were more likely to have a longer stay in hospital (p < 0.001), to be discharged to a care institution (p = 0.000), and to have a higher delirium observation score (p < 0.001) (table 2).
The overall mortality rate one year after hospital admission was 31%. There was no significant difference in one-year survival for the type of illness presentation (p = 0.056) (table 2). If we excluded the fit elderly patients who had a fall by deselecting patients with a fall merged with a Charlson comorbidity index of 0 and 1, the group with atypical presentations was significantly associated with a lower one-year survival (27% versus 42%, p = 0.009).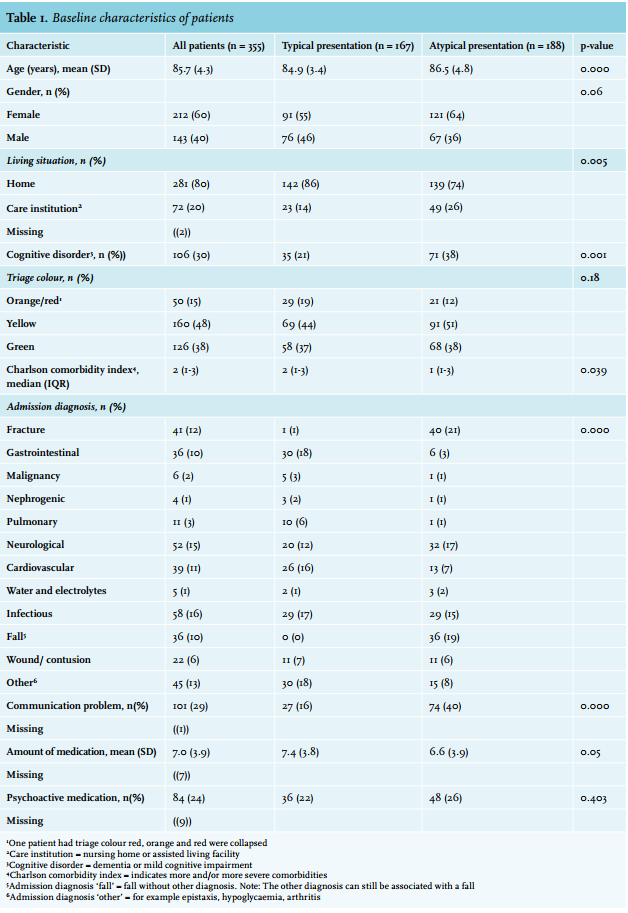
DISCUSSION
This is one of the few studies to report on the prevalence of atypical illness presentations in elderly patients in the emergency department. The prevalence data indicate that a great proportion of patients aged 80 and older have an atypical illness presentation. Apart from Limpawattana et al., who found that approximately one-third of older patients present with atypical illness presentation, we found no other sources of prevalence data about atypical illness presentation in the emergency department for elderly patients, nor a univocal definition for atypical illness presentation. Much research has been done on geriatric syndromes or atypical illness presentation for single diseases. Furthermore, geriatric syndromes seem to be highly prevalent in the emergency department.13,14
Lack of standardised terminology certainly indicates that proper research on this topic is difficult and an appropriate diagnostic approach and medical treatment is therefore difficult too. We know that physicians in the emergency department often lack geriatric training and are not confident in seeing elderly patients.4 They are used to the classic medical model of diagnostic thinking, in which presenting symptoms and signs are aggregated into a diagnosis of a single pathological condition.15 This approach does not sufficiently consider the complexity of older patients.16 Therefore adequate training of emergency staff is essential.
Atypical disease presentation is more common in the frail elderly (59%) than in non-frail elderly (25%).7 We perceived this in our study as well, as patients with atypical illness presentations appeared to be more vulnerable. They were older, more often resided in a care institution, experienced higher rates of cognitive disorders and had more problems with communication in the emergency department. In emergency departments, impaired higher functions related to dementia or delirium are present in 25% of patients aged over 75 years.4,17 These conditions can decrease the accuracy of the diagnosis of the main symptoms and mask potentially serious diseases.
The low Charlson comorbidity score in the group with atypical illness presentation seems to be contradictive. There are a couple of reasons for this: the Charlson comorbidity score18 was not corrected for age and the underlying disease at time of admission was not included in the score. Furthermore, the group with an atypical illness presentation contains a considerable number of fit elderly patients with an isolated fall. This is likely because fit and active elderly patients have a higher probability of falling.
In nearly all cases an atypical illness presentation coincided with a geriatric syndrome, in which falling was the most frequently mentioned reason of admission. A previous study showed that 80% of the geriatric syndromes in the emergency department were caused by falls or confusion.19 In our study falling accounted for 71% of patients with an atypical presentation. This is not surprising as falling is one of the main reasons for elderly patients to visit the emergency department (15-30%).
In our patients with atypical presentations, the most frequent diagnoses were fractures, and neurological and infectious diseases. In one-third the underlying disease of the atypical illness presentation was not determined. Unexplained falls accounted for the majority of undetermined atypical presentations. Elderly patients often cannot recall the fall because of syncope with memory loss or existing cognitive disorder.
Patients with an atypical illness presentation seem to have a worse clinical outcome.3,4,9,11,14,17 We affirmed this in our study; they have a longer stay in hospital. However, we do not know whether atypical presentation is an independent risk factor. Possible causes for poor outcomes include comorbidity and frailty, a longer diagnostic process and missed diagnosis, less accurate or a delay in treatment,20,21 illness severity, and more complications such as delirium. We found a high delirium observation score in this group, which must be interpreted cautiously because a high score can also be explained by the high degree of cognitive impairment in this group. Furthermore patients with atypical illness presentation are more often discharged to a care institution, which implies a decline in their health status.
The mortality rate one year after hospital admission was 31%. This is in line with a study from the Rooij et al. which showed a mortality rate of 35% after one year.14 Although this study provides useful information on the prevalence of atypical illness presentations and the characteristics of these patients, we found no significant difference in one-year mortality. This is likely due to the high number of non-frail elderly who presented with an isolated fall without other complications. We found that if we excluded these patients, the group with atypical illness presentation is significantly associated with a lower one-year survival. However, the higher Charlson comorbidity index in this subgroup could be the reason for this association as well, as it implies more or more severe comorbidity.
A few important limitations need to be acknowledged. First, the retrospective nature of the study restricted data to those routinely collected. Important unmeasured factors include socioeconomic status, social support, education level, delay before admission and substance abuse. Furthermore the reporting rate of geriatric conditions in emergency department summaries was low. A former study showed that older patients present with an average of six geriatric conditions,14 and often acquire new syndromes during hospital admission.13 The underreporting of geriatric conditions actually reflects the under recognition of geriatric conditions during a hospital stay.3,14 Second, potential recording bias may exist on retrospective analysis of medical records. However the study sought to minimise recording bias by incorporating the mutual review of the manner of presentation by two independent observers. Thirdly, this study focused on patients’ leading symptom, which may underestimate the true prevalence of atypical presentation of other co-existing diseases, as we did not include the absence of physical signs at examination in our definition of atypical presentation. Fourth, co-existence of different components of atypical illness presentation (e.g. fall and delirium), was considered a single entity, which may overlook the cumulative effect of all elements of atypical illness presentation. Fifth, because this hospital is the only hospital in Amsterdam with an acute geriatric ward, patients with atypical illness presentation may preferably be referred to this hospital by general physicians. This may lead to an overestimation of the prevalence of atypical presentation.
In conclusion, atypical illness presentation, mainly falls, account for more than half of the elderly patients in the emergency department and this group seems to be vulnerable to adverse outcome. In 15% of these patients typical symptoms of an underlying disease are absent in the (hetero) anamnesis. Emergency department staff should be trained to recognise this group of patients to ensure proper clinical monitoring and timely treatment. Since atypical illness presentation is the result of multifactorial health conditions that occur when impairments in multiple systems accumulate, the diagnostic workup for this group of patients should be a thorough diagnostic approach, such as a geriatric assessment.22
Finally, more research should be devoted to atypical illness presentation in the elderly patients by prospective multicentre survey.
DISCLOSURES
All authors declare that they have no conflict of interest. No financial support was received for the conduct of this study or preparation of this manuscript.
REFERENCES