KEYWORDS
Decision-making, dialysis, ESRD, regret, treatment satisfaction
INTRODUCTION
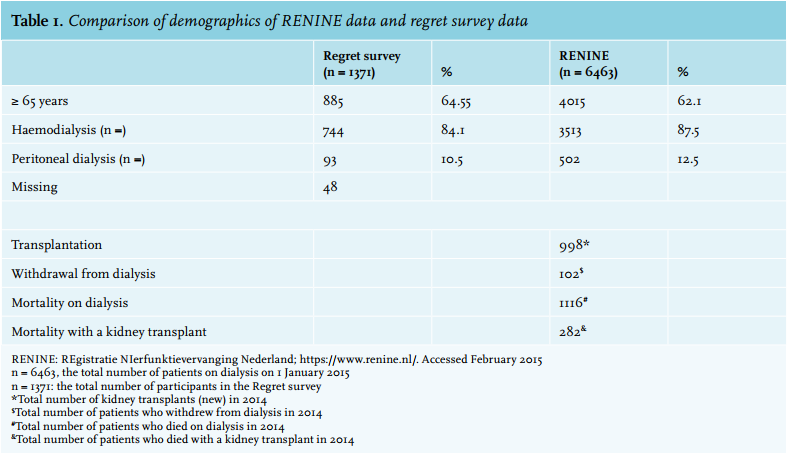
Worldwide the number of older patients with end-stage renal disease (ESRD) starting dialysis is rising. In the Netherlands, 6463 patients were on dialysis in January 2015, 62% of whom were ≥ 65 years and within this group 37% were ≥ 75 years (for details see Appendix, table 1). Dialysis is associated with a high physical and psychosocial burden and limited survival, particularly for older patients with multi-morbidity.1-3 Because of this many older patients prefer treatments that focus on quality of life (QOL) rather than primarily extending life with patient’s personal values and perceptions playing an important role in the decision-making process.4,5
In the Netherlands multidisciplinary pre-dialysis care is formally established and its implementation monitored by certification.6 Information on treatment options for ESRD encompasses a conservative care treatment option with a significant percentage of patients choosing not to undergo dialysis.7 Early referral,8-10 comprehensive pre-dialysis education, a planned start to dialysis and shared decision-making are cornerstones of pre-dialysis treatment and are in alignment with recommendations made by the Renal Physicians Association and the ‘Choosing Wisely’ campaign in the US.11 Some studies have shown that an unplanned or sudden start to dialysis negated the benefits of early referral12,13 whilst QOL improved and depression decreased when dialysis initiation was planned.14 A number of surveys have shown that patients on dialysis felt they did not receive enough information to be able to make an informed decision.15-21
In a Canadian study, 61% of 584 dialysis patients regretted their decision to start dialysis over conservative care.5 In their study the decision-making process reflected preferences of physicians and family members rather than the patient’s personal choice, which could be one of the reasons for this alarmingly high regret rate. In contrast, in a recent survey of 128 US haemodialysis patients it was found that only 7% of participants regretted the decision to start dialysis even though 50% of patients reported that their nephrology provider was the person who most influenced their decision.22
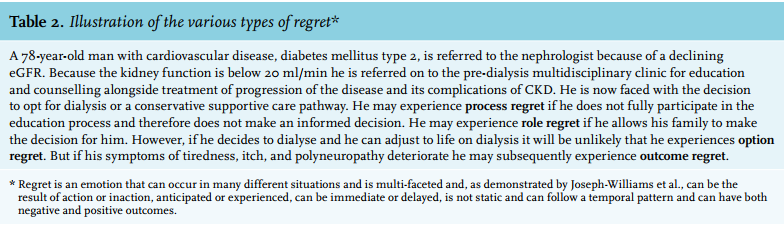
Regret about decisions is a complex emotion which occurs in many different situations, is multifaceted (see Appendix, table 2, for an explanation on regret) and the second most frequently cited emotion after anxiety.23 Shared decision-making has the potential to limit decisional regret and is defined as ‘an approach where clinicians and patients share the best available evidence when faced with the task of making decisions, and where patients are supported to consider options, to achieve informed preferences’. 24 This begs the question how to ensure that treatment choice is a true reflection of the patient’s personal preferences and values so that patients experience less regret and more satisfaction with the choices they have made.
Given the structured information trajectory on ESRD treatment options in the Netherlands, which annihilates large differences between healthcare providers, we explored patient experience on treatment choice. Our aim was to measure the percentage of patients in the Netherlands who regretted their decision to start dialysis and to establish whether factors such as satisfaction with the treatment, whose opinion was crucial in the decision-making process, acute dialysis initiation, age and gender, were related to regret.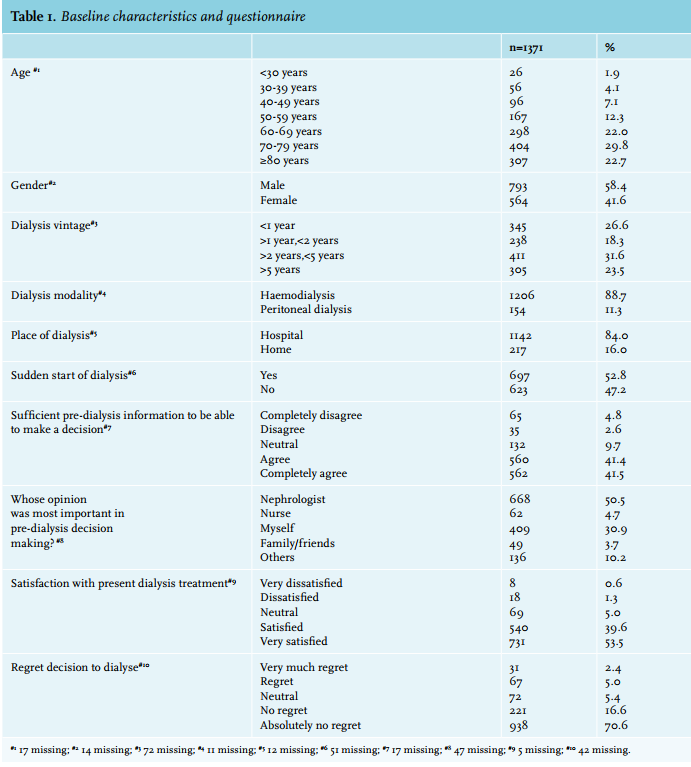
METHOD
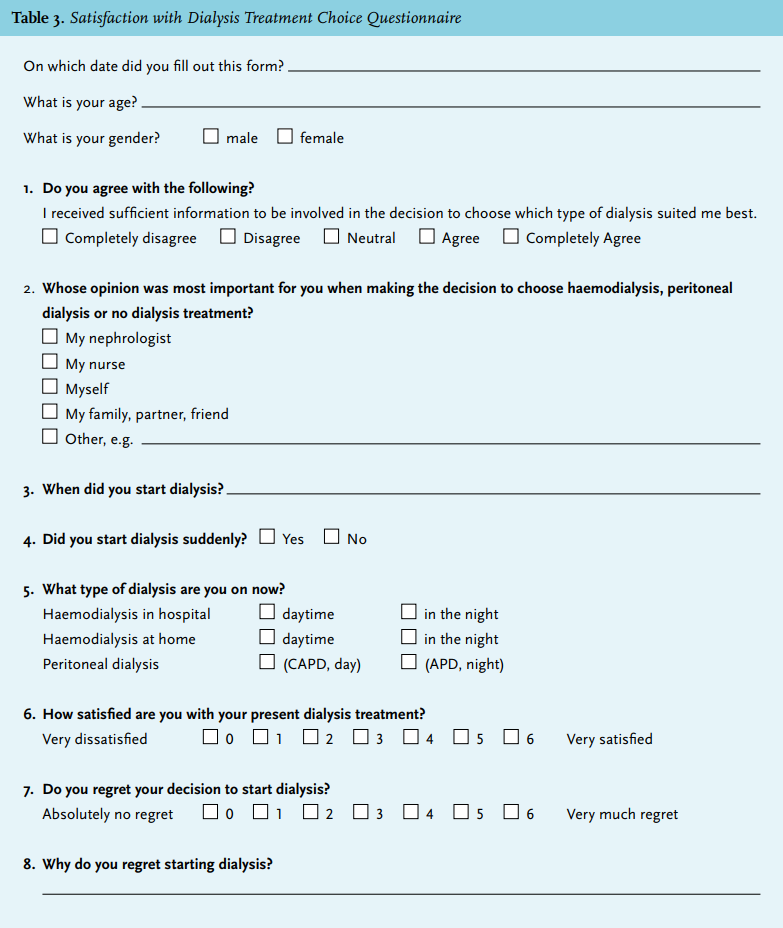
As part of a quality of care initiative a short questionnaire was developed and included characteristics such as age, gender, dialysis vintage, satisfaction with pre-dialysis education, dialysis modality, planned or acute dialysis initiation (for questionnaire see Appendix, table 3).
Other key elements incorporated into the questionnaire included satisfaction with treatment, regretting the decision to start dialysis and participants taking part in the decision-making process. The questionnaire was pilot-tested on a convenience sample of dialysis patients (face validity). After revision, re-testing the questionnaire was carried out to ensure ease of completion, clarity of questions and response options. Content validity assessment was established by a panel of experts (nephrologists, geriatricians, nurse practitioners, dialysis nurses). An assessment of appropriateness of wording and clarity was also requested. In general the questionnaire took 10 minutes to complete.
Dialysis patients ≥ 18 years of age, who were cognitively able to complete the questionnaire in Dutch, could participate. An e-mail was sent to all Dutch dialysis units inviting them to participate. Each participating centre approached their dialysis patients. The anonymous questionnaire was distributed between 25 May and 1 October 2014. The medical ethics committee of Leiden University Medical Centre exempted the study from the need for approval. The fact that patients completed and sent back the questionnaire, after being informed of the purpose and scope of the survey, was considered equivalent to informed consent. Following analysis each centre received a report with their results.
The eight-item questionnaire contained topics that are an integral part of the pre-dialysis decision-making process. Satisfaction with pre-dialysis information was measured using a five-point scale where ‘1’ means ‘completely disagree’ and ‘5’ means ‘completely agree’. For the question about whose opinion was most influential in the decision-making process, five options were given: the nephrologist, nursing staff, myself, my family or friends, others. Satisfaction with the present dialysis treatment was measured using a six-point scale where ‘0’ means ‘very satisfied’ and ‘6’ means ‘very dissatisfied’. Regret about the decision to start dialysis treatment was measured using a six-point scale where ‘0’ means ‘absolutely no regret’ and ‘6’ means ‘very much regret’.
The qualitative data, transcripts of 206 remarks, were analysed systematically by thematic analysis. Two nephrology nurse practitioners, a nephrologist and two psychologists with experience in the field of nephrology were asked, via an open coding method, to code and categorise the remarks. Then main themes and sub-themes were identified, after which consensus was reached about the themes. In this qualitative analysis the patient comments took priority over the actual score on regret and therefore the reason for regret cannot be directly linked one to one to the score.
Statistical analysis
Scale (continuous) variables are given as mean ± standard deviation (SD). Categorical (nominal and ordinal) characteristics are shown as numbers and percentages. Association between discrete ordinal variables with less than five categories was analysed using cross-tables with Pearson’s chi-square or Fisher’s exact test, when appropriate. In case of correlation between ordinal variables with more than four categories and/or discrete scale variables Kendall’s tau-b was calculated. Differences of means between multiple groups were analysed using one-way analysis of variance (ANOVA) and post-hoc testing according to Tukey’s honest significance test. To predict the association of the impact of whose opinion was important for the occurrence of regret, binary logistic regression was used. In a multivariate model we adjusted for possible confounding effects for age and gender on this association. The same procedure was used for the analysis of the relationship between occurrence of regret and sufficient pre-dialysis information, and separately between regret and satisfaction with dialysis treatment. Probabilities for each decision-making category and age group were calculated and plotted. P-values < 0.05 were considered statistically significant. All analyses were performed using IBM SPSS Statistics package, version 20.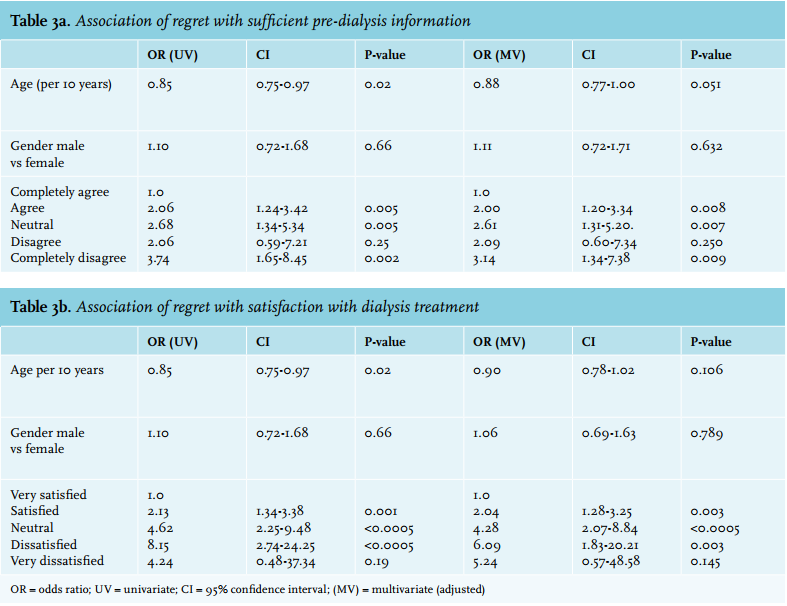
RESULTS
We approached all 66 national dialysis units and 28 of these Dutch dialysis units (42%) participated in the survey. In total 2624 questionnaires were sent by post to the different dialysis units and 1371 were returned for the final analysis (52% response).
All participants in this survey were on haemodialysis or peritoneal dialysis, 64.5% of whom were ≥ 65 years. In-centre haemodialysis was the dominant form of dialysis (88.7%) (table 1). The results were representative for the Netherlands and compared well with those from the RENINE registry (Registratie nierfunctievervanging Nederland) (for details see Appendix, table 1).
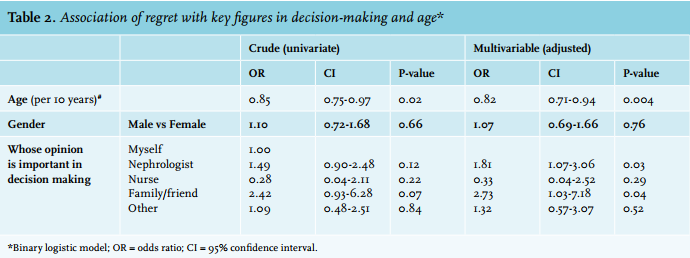
Of 1329 respondents (42 missing), 7.4% reported regretting their decision to start dialysis (table 1, Appendix table 3). Older age was associated with less regret (Kendall’s tau-b: -0.06, p = 0.011) and higher treatment satisfaction (Kendall’s tau-b: 0.12, p < 0.001). In comparison with the very old patients (> 80 years), younger patients (< 30 years) had a higher risk for regret and the odds ratio for regret with the decision to dialyse decreased (on average) by 18% with the increase of age per decade (odds ratio: OR: 0.82, [confidence interval: 95% CI, 0.71 to 0.94]) (table 2, figure 1) and, moreover, the younger the patient the more regret experienced (< 50 years versus 50-69 years: OR: 1.66, [95% CI, 0.89 to 3.09], p = 0.108; < 50 years versus > 70 years: OR: 2.05, [95% CI, 1.13 to 3.72], p = 0.019; 50-69 years versus > 70 years: OR: 1.23, [95% CI, 0.76 to 2.00], p = 0.399).
Overall 50.5% of the patients reported the nephrologist’s opinion to be crucial in the decision-making process (table 1). When the role of the nephrologist was the most important in decision-making, patients experienced more regret compared with patients who reported that they had made the decision themselves (adjusted for age and gender, OR: 1.81, [95% CI, 1.07 to 3.06]) (table 2, figure 1).
A small number of patients (3.7%) reported that family or friends played an important role in decision-making and when the role of the family was important, the OR for regret was found to be higher (OR: 2.73, [95% CI, 1.03 to 7.18]) (table 2, figure 1) and significance was reached (p = 0.04).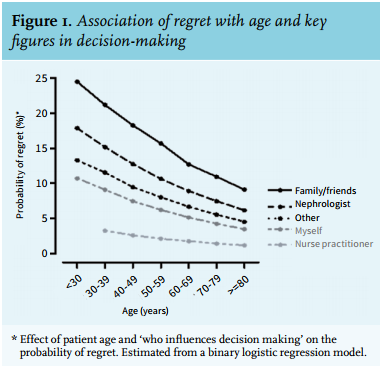
Overall 30.9% of the participants reported that they themselves were most important in the decision to start dialysis (table 1). Patients who reported that it was primarily their own decision to start dialysis were younger particularly in comparison to those whose decision was influenced by the nephrologist (63.8 ± 16.65 versus 70.0 ± 13.05, p < 0.001). When making the decision to choose haemodialysis, peritoneal dialysis or no dialysis treatment, 4.7% of participants reported that their nurse was important and 10.2% reported others as key figures in decision-making (family, doctor, peers etc.) (tables 1 and 2, figure 1).
There seemed to be a strong relationship between both sufficient pre-dialysis information to be able to partake in the decision-making process and satisfaction with dialysis treatment and regret. Participants who did not receive sufficient information had a higher risk for regret (complete disagreement, OR: 3.14, [95% CI, 1.34 to 7.38]), p = 0.009 (table 3a). Likewise participants who were dissatisfied with dialysis treatment had a higher risk for regret (dissatisfied, OR: 6.09, [95% CI, 1.83 to 20.21]), p = 0.003, (table 3b).
Overall 52.8% of the participants described dialysis initiation as sudden with the lowest reported percentage of sudden starts at 36.5% and the highest at 81.8% (table 1). This high percentage of sudden starts warranted further investigation. Of the 28 centres, 12 returned information about their percentages of medical urgent starts in 2014.
These returned figures were below the 52.8% reported by participants in our survey with the lowest medical urgent start rate reported by participating centres at 7.40% and the highest at 39.4%.
No association was found between regret and dialysis modality (p = 0.68), regret and place of dialysis (home versus in-centre) (p = 0.83), or regret and acute start of dialysis (p = 0.19). No differences were found in gender and dialysis vintage between patients who regretted their decision to be treated with dialysis compared with those who did not regret their decision.
Patient comments about regret
Of the 1371 returned surveys, 1329 patients answered the question about regret (42 missing). Of this group 139 patients (10.5%) commented on their answer and reported regret due to a limited choice/no choice (55%), lack of information (11%), unfavourable side effects of dialysis (20 %), or other reasons, for example, no other alternative (14%). A further 67 patients (32.5%) reported no regret but did, however, comment on this question (table 4).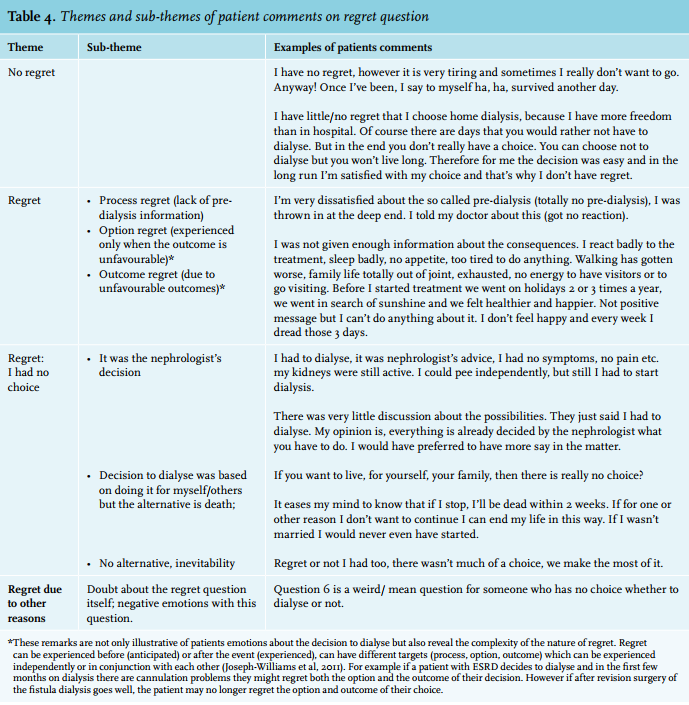
DISCUSSION
The main result of this survey was that of all the dialysis patients, 7.4% regretted the decision to start dialysis while the very old experienced less regret than younger patients. The results revealed that the nephrologist’s and family’s influence on decision-making was associated with more regret, particularly in younger patients and over 50% of patients reported dialysis initiation as being sudden. Furthermore, the results uncovered a number of reasons why patients experience regret. These findings highlight important factors in decision-making in the pre-dialysis phase and may add to limitation of decisional regret.
A limited number of participants regretted dialysis initiation and our results complement those of a recent survey in the US where 7% of patients regretted starting dialysis.22 Results from both our study and the US study are in stark contrast to the high regret rate (61%) found in the Canadian study.5 In our survey older age was found to be associated with less regret and higher treatment satisfaction, which is surprising as many elderly patients are burdened by multiple comorbidities and are frail and because of this, are willing to trade a longer life expectancy for maintenance of QOL.4,5 However, this relatively low level of regret could have been an underestimation as elderly patients (particularly those with cognitive impairment, frailty and multi-morbidity) might already have withdrawn from dialysis, indeed might not even have started dialysis.25
The majority of participants reported being satisfied with the present dialysis treatment. Taken together with the majority of patients who reported having received enough information to be able to participate in the decision-making process, the low regret rate suggests that pre-dialysis education in the Netherlands is indeed well and truly established. These findings are consistent with the results of a European survey carried out in 36 countries where patients reported being overall satisfied with information they received.19 Similarly, in the US study 58% of patients described their quality of life as ‘good’ or ‘very good’ and 68% agreed they were prepared for dialysis.22
Although over 50% of the respondents reported the nephrologist as being important in decision-making, particularly older patients were satisfied and experienced less regret in this situation. Foote et al. demonstrated that older patients preferred their healthcare team to make decisions for them with patients regarding physician preferences as important.26 Likewise in the US study, 50% of patients reported their nephrology care provider as the most influential person in their decision to start dialysis.22 The prominent role played by physicians in dialysis decision-making has been widely recognised,17,27-29 with age, comorbidities, cognition, functional status, perceptions of QOL and patient or family request governing recommendations.20,25,26,30 Therefore, the low rate of regret found in this survey, juxtaposed with the high influence of the nephrologist, begs the question whether physician influence should always necessarily be seen as undesired, particularly when the patient’s subsequent satisfaction with dialysis is not negatively affected. On the basis of our results we advocate firstly the importance of recognising the different factors which influence individual decision-making where patient values and preferences are given prominence of place. Secondly the role of the nephrologist to be double-barrelled, not merely delivering information but importantly to follow through in facilitating a decision in the role, coined by Kurella as choice architects21 hereby supporting and guiding each patient to a decision which befits their personal situation.
In contrast to older patients, it was found that younger patients had a higher risk for regret, especially when the nephrologist influenced decision-making. This result may suggest decisional conflict between younger patients and the nephrologist and importantly an unresolved decisional conflict is associated with experiencing regret and blaming providers.31,32 Factors influencing patient involvement in shared decision-making include younger age, level of education, employment status and use of internet28,33 with younger patients choosing options which increase the opportunity to find work or to remain employed.29,33-36 Furthermore the higher regret rate in younger participants could be explained by disappointment regarding lack of transplantation options. These factors are therefore relevant and should be considered in the decision-making process.
Contrary to expectations, family members played only a minor role in the decision-making process (3.7%) which differs from a number of other studies,5,29,36 but importantly when family were involved the chance of regret was found to be higher. Traditionally family members are seen as important participants in renal replacement therapy (RRT) modality choice37 because of the profound impact on their own lives4 and are therefore included in shared decision-making. Further research is needed to evaluate why ‘doctor dominant’ and ‘family dominant’ decisions rather than personal patient decisions are determinants of decisional regret.
Unravelling the reasons for regret and understanding its complexity is essential for improving shared decisionmaking. In this survey patients reported feeling regret because of lack of information, a limited or even no choice in the pre-dialysis phase, or because of unfavourable side effects of dialysis, which could be a form of delayed regret as the treatment gains its insidious grip on everyday life. Clearly some patients felt there was no other alternative, it was dialysis or death. The themes identified fit the model of regret proposed by Joseph-Williams et al.23 and as such are modifiable. Information and education deficits prior to decision-making can be remitted by honest explanation of all the options including possible unfavourable consequences of dialysis for QOL. Actively encouraging patient involvement in decisions pertaining to RRT has the potential to limit decisional regret. Ambiguity was found between the reported experience of regret and the score on the regret scale, which indicates that all is not black and white and that many shades of grey surround the complex emotion of regret. Future research could help differentiate the source of experienced regret and interventions could be designed to minimise the risk of experiencing regret.
A major finding in this survey was the high percentage of participants who reported dialysis initiation as sudden (52.8%), which is remarkable given the high rate of satisfaction found alongside the reported high rate of information received prior to modality choice suggesting established pre-dialysis care and a planned start to dialysis. Our findings are in accordance with the results of the US study where 51% of patients reported starting dialysis in an acute hospital setting in spite of being prepared for dialysis.22 Possible explanations include an unavoidable rapid decline of kidney function, late referral for education and counselling, patients own reluctance to start dialysis, delayed creation of vascular access and age discrimination in older patients with multi-morbid conditions. In the Netherlands, ‘sudden’ or ‘urgent’ start to dialysis is defined as dialysis initiation with less than six months of pre-dialysis care, with a catheter or as an inpatient. Planned dialysis initiation with vascular access is a marker of good practice. However, uncertainty about the course of each individual’s illness trajectory and planning dialysis initiation is often difficult, even in early referred patients.12 Furthermore, when care in the immediate months prior to RRT is inadequate the benefit of early referral can be lost if dialysis initiation is unplanned.13 The high number of patients reporting a sudden start suggests that the transition period from pre-dialysis to actual RRT was perceived by patients as unexpected and in spite of adequate pre-dialysis care, patients can never truly be ready for such an invasive treatment.4,28,38,39
This survey set out primarily to inquire about the percentage of the Dutch dialysis population who regretted starting dialysis. There were several limitations to this survey, some of which are intrinsic to the use of questionnaires. Possible confounding could have taken place by the questionnaire being completed in different places and in consultation with others. The findings were based on recollection and particulars in the pre-dialysis decision-making process and information about patients who declined to complete the survey or about economic status and education cannot be retained. The low rate of regret could have been due to healthier older patients choosing dialysis above conservative management or possibly non-motivated patients and those with additional physical and mental disabilities may have refused to participate in the survey or may not have been approached by the nurses. Despite these limitations, this was the first multicentre survey in Europe which measured the percentage of regret with the decision to dialyse, in spite of dialysis being a very disabling and invasive therapy. The return rate was high and because university hospitals, local community hospitals and satellite dialysis units participated, with diverse ethnic populations, results may be considered as representative for the Dutch dialysis population.
In conclusion, in this survey 7.4% regretted the decision to start dialysis and the very old experienced less regret than younger patients. More regret was experienced when the nephrologist and family were reported to play an important role in decision-making, particularly in younger patients and a number of reasons why patients experience regret were uncovered. A high percentage of respondents reported a sudden start to dialysis despite comprehensive pre-dialysis care. Our findings highlight the importance of decision-making being attuned to values and preferences of individual patients with specific attention being given to age related factors and significant others influencing shared decision-making.
ACKNOWLEDGEMENTS
Céline van Lint and Yvette Meuleman (psychologists) and Mieke Moses (nurse practitioner) who coded and categorised patients remarks on regret and who contributed intellectual input to formulating the sub-section on patients remarks about regret. The nursing staff and secretaries of the 28 dialysis units who approached their patients and distributed and retrieved the surveys. Shantily Lourens and Daniel Bimmel for their help building the database.
DISCLOSURES
The first author was awarded The Maria Ter Welle Prize for innovation and quality of care in 2014 which is funded by the Dutch Kidney association and the Willem Kolff Foundation. A small part of the prize was used to aid data retrieval. The Institute for Evidence-based Medicine (IEMO) is funded by the Dutch Ministry of Health and Welfare and supported by ZonMw (project number 62700.3002)
The results presented in this paper have not been published previously in whole or part, except in abstract format.
The authors declare that they have no other relevant financial interests.
REFERENCES
![]()