KEYWORDS
Health status, Chronic Obstructive Pulmonary Disease (COPD), COPD assessment test, normative values
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is a lung disease characterised by persistent respiratory symptoms and chronic airflow limitation.1 In addition to the pulmonary manifestations, COPD often provokes symptoms of anxiety and depression and causes limitations in daily life. In addition, a recent international patient survey revealed that 6% to 52% of working age patients are completely prevented from working due to their COPD.2 The impact of these restrictions is often underestimated.3,4 The COPD Assessment Test (CAT) is a simple patientcompleted questionnaire developed to quantify the impact of COPD on health status, focusing on daily symptoms and activities.5 Patients with an impaired health status experience a high burden of symptoms.6
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) strategy describes an impaired health status as a CAT total score of ≥ 10 points, which is derived from the St. George Respiratory Questionnaire (SGRQ) cut-point of ≥ 25 points.1 Previous studies determined normative values for other health-related measurements, e.g. echocardiographic measurements, according to the 95th percentile in a reference population.7,8 Defining abnormalities based on percentile values will account for an asymmetric distribution and the range of abnormality present within a population.9 With the current GOLD CAT cut-point of ≥ 10 points, only a minority of primary care COPD patients have a normal health status.6,10 Moreover, previous research showed that an impaired health status, derived from the current GOLD CAT cut-point, already occurs in half of the current or former smokers without airway obstruction.11 This highlights the importance of understanding what an abnormal CAT value is, as it consequently also influences treatment choices in these patients. The large proportion of patients with an impaired health status resulting from the current GOLD CAT cut-point raises the question as to whether deriving abnormal values from the 95th percentile of CAT in a non-COPD population would give a better representation of reality, as suggested for several countries.12-14
While the societal burden of COPD is considerable, the impact of sociodemographic characteristics, such as work status on health status, is largely unknown. Less ability to participate in society and not being able to work are important concepts in an impaired health status.15 Previous research showed comparable CAT scores between a working COPD population and a working non-COPD population.12
The primary aim of this study was to investigate which cut-off value represents an abnormal CAT score for non-COPD subjects in a Dutch population. The secondary aim was to measure the impact of COPD on health status in a Dutch population, after stratification for work status.
METHODS
Current data are collected from a subsample of the Longitudinal Aging Study Amsterdam (LASA), a large population-based study.16 The study was initiated by the Dutch Ministry of Welfare, Health and Culture to determine consequences and predictors of ageing, focusing on physical, emotional, cognitive and social functioning in late life. Ethical approval for the LASA study was given by the Medical Ethics Committee of the VU University Medical Center Amsterdam (METC number 2012/361).
Population
Subjects aged between 55-65 years were randomly sampled from 11 municipalities of three culturally different geographic regions (Amsterdam, Zwolle and Oss) in the Netherlands. Subjects were drawn from the population registers and subsequently interviewed by trained persons in their homes. To make up the original sample, no inclusion or exclusion criteria were outlined in the LASA study. However, individuals who did not complete the medical interview and/or did not perform a spirometry were not included in the analyses.
Measurements
Between November 2012 and November 2013, subjects received a baseline interview assessing demographics, smoking history, work status, self-reported diseases and post-bronchodilator spirometry (forced expiratory volume in the first second, FEV1, and forced vital capacity, FVC). The spirometry was conducted with a Vmax Vyntus SPIRO – USB PC Spirometer from CareFusion (Höchberg, Germany), 15 minutes after inhalation of 200 μg salbutamol (Airomir autohaler, Teva). Global Lung Function Initiative (GLI) reference values were applied. Instead of managing the GOLD suggested fixed cut-off point for obstruction (FEV1 /FVC ratio < 0.7), an FEV1 /FVC ratio after bronchodilator lower than the 5th percentile (from reference values) was applied to define airway obstruction.17 Patients with COPD were divided into four groups: spirometric grade 1 (FEV1 ≥ 80%), spirometric grade 2 (FEV1 50-79%), spirometric grade 3 (FEV1 30-49%), and spirometric grade 4 (FEV1 <30%), based on the GOLD strategy 2017.1 Additionally, health status was assessed with the CAT. The CAT is an eight-item patient-completed questionnaire, designed to measure health status in patients with COPD. Item scores range from 0 to 5 points, whereby the total score varies between 0 (best health status) and 40 points (worst health status).5 An impaired health status was defined with the CAT ≥ 10 cut-point and 95th percentile of the non-COPD population.
Statistics
Descriptive statistics, including means (standard deviation, SD) and medians (interquartile range, IQR), were applied. Categorical variables were described as frequencies. CAT normative values were described by percentiles using mean (SD), median and range. First, the calculation of normative values was performed in the whole non-COPD population. All variables were tested for normality with the Kolmogorov-Smirnov test. Differences between non-COPD subjects and COPD patients were assessed by performing an independent Student’s t-test, when normally distributed. Otherwise, a Mann-Whitney U test and two-independent-samples tests were done to compare the two groups. When appropriate, a post hoc least significance difference multiple comparison was performed. A Kruskal-Wallis test was assessed for not normally distributed variables and a Chi-square test was applied for categorical variables. Similar analyses were performed to compare working and non-working groups. A p-value of less than 0.05 was considered statistically significant. All statistics were done using SPSS V.20.0.
RESULTS
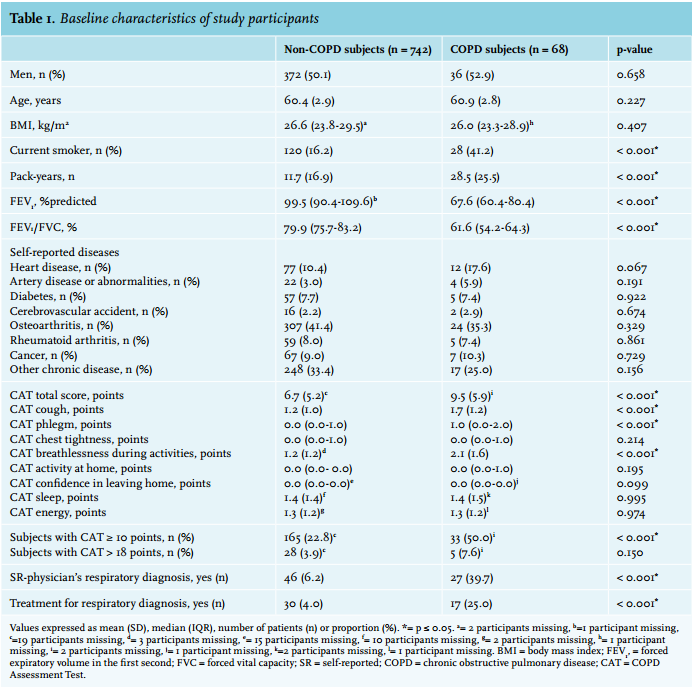
In total, 810 subjects (50.4% male, mean age 60.5 (2.9) years) were included, 68 (8.4%) of which had a chronic airflow limitation: 18 GOLD spirometric grade 1, 43 GOLD spirometric grade 2, 5 GOLD spirometric grade 3, and 2 GOLD spirometric grade 4 (see figure 1 for flowchart). Twenty-seven of the COPD subjects (40%) were previously diagnosed with a respiratory disease; 10 (37%) received COPD treatment from a general practitioner, 7 (26%) received COPD treatment from a specialist and 10 (37%) received no treatment. The non-COPD and COPD groups were similar regarding age, gender, BMI and comorbidities. Non-COPD subjects were less often current smokers and had a higher FEV1% predicted than subjects with COPD (table 1).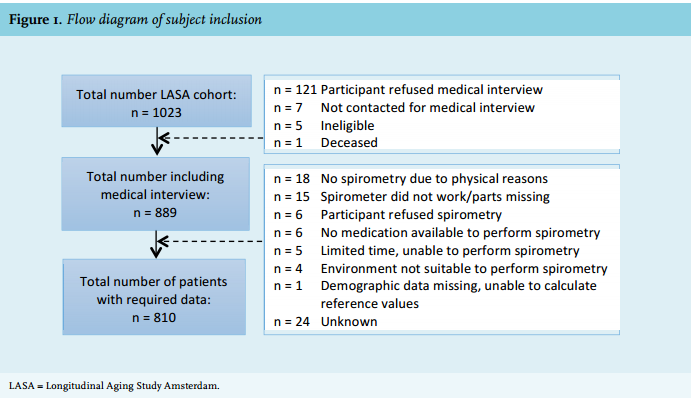
COPD versus non-COPD
CAT total scores were significantly lower in non-COPD subjects than in COPD subjects. COPD subjects had significantly higher scores on CAT questions related to cough, phlegm and breathlessness during activities (table 1). CAT values of non-COPD subjects ranged from 0 to 29 points, with the 95th percentile at 18 points (table 2). When applying the CAT ≥ 10 cut-point, 50.0% of COPD subjects had an impaired health status and when using a CAT > 18 cut-point 7.6% of COPD subjects had an impaired health status (table 2).
Work status
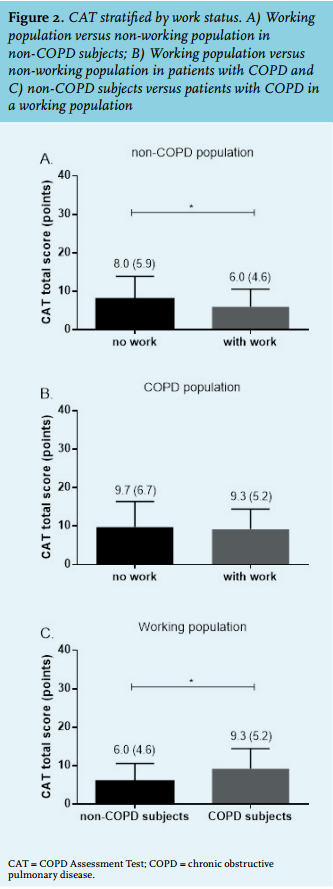
As shown in figure 2, CAT total scores were significantly lower in non-COPD subjects with a job, compared with non-COPD subjects without a job, p < 0.001. No significant differences were observed between a working and non-working COPD population, p < 0.741. Moreover, significantly higher CAT scores were observed in a working population with COPD in comparison with a working population without COPD, p < 0.001.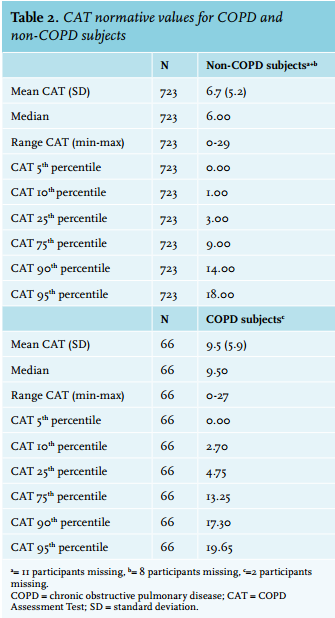
DISCUSSION
This is the first study examining normative values for CAT performed in a Dutch population. It shows that approximately 20% of the non-COPD subjects had an impaired health status according to the current cut-point suggested by GOLD (CAT ≥ 10 points). Based on the 95th percentile of the CAT in a non-COPD population, a new CAT cut-point of > 18 points was suggested to indicate an impaired health status. No significant differences in CAT score were found between a working and non-working COPD population. Normative values should be taken into account when applying the refined GOLD assessment to Dutch COPD patients in clinical practice.
In accordance with previous research,18 the current study showed that patients with COPD had significantly more symptoms of cough, phlegm and breathlessness during activities. Reported mean CAT total scores in COPD subjects vary between 7.3 points (± 5.2 [n = 67, Japan]), 16.6 points (95% CI = 15.5-16.8 [n = 806, Arabic countries]) and 20.9 points (95% CI = 16.9-22.2 [n = 229, Turkey]).12-14 A mean CAT of 9.5 points was observed in the current study. Moreover, a value of 18 points was found as the 95th percentile of CAT total scores in non-COPD subjects, resulting in 7.6% of the COPD patients with an impaired health status. Previous studies showed that the 95th percentile of CAT total scores in non-COPD subjects varies from 14 points (n = 1266, Japan), 16 points (n = 500, Canada), 21 points (n = 2863, Arabic countries) and 28 points (n = 872, Turkey).12-14 Differences in disease severity, demographics, comorbidities, care setting, religion, culture and socio-economic factors may account for the observed variation.19-22 When comparing disease severity between studies, airflow obstruction was equivalent.12-14 Furthermore, not all previously performed studies measured comorbidities, and if they did, often other diseases were assessed, making a comparison difficult. Indeed, Nishimura and colleagues showed that a working population is often more active during the day,12 resulting in a better health status and less symptoms.23 Moreover, the use of a CAT cut-point of > 18 points is supported by the study of Casanova and colleagues, stating that a CAT cut-point of > 18 points more comprehensively categorises patients with COPD according to the GOLD classification and more adequately predicts all-cause mortality.24
While the current study found differences in CAT scores between a working and non-working non-COPD population, no significant differences were found between a working and non-working COPD population. In addition, COPD patients with a job still had significantly higher CAT scores than non-COPD subjects with a job. So, it is possible that solely having a job improves heath status (to a certain extent) in a general population, but this does not apply for COPD patients. Previous research indicates that variation between multiple populations can also be explained by differences in quality of life between countries.25 Defining influences of the other variables (demographics, care setting, religion, culture and socio-economic factors) goes beyond the scope of this study.
Another important factor to consider when describing normative values is the impact of comorbidities. In the current study, approximately 10% of the non-COPD subjects reported heart disease, presumably leading to a higher CAT total score. However, there are several reasons for not excluding comorbidities in the non-COPD group. First, a study by Gupta and colleagues indicated that only depression, myocardial infarction, angina and/or pneumonia influence CAT score.26 Another study showed that solely gastro-oesophageal reflux disease and depression have an impact on CAT.27 However, not all these comorbidities were assessed. Therefore, we were not able to determine these influences. Also, comorbidities in the current study were self-reported. The study by Triest and colleagues showed a poor agreement between objectively identified and chart-based comorbidities in patients with COPD,28 resulting in unreliable outcomes. Finally, as patients with COPD also experience many comorbidities,29 it would be unrealistic to compare patients with completely healthy individuals. Subsequently, the current results showed no differences in comorbidities between subjects with or without COPD. This indicates that comorbidities are not specifically related to COPD, making them valuable for normative values of the CAT.
Limitations
There are some limitations to this study. First, selection bias could have occurred, indicating that people who lack motivation or with a worse health condition are less willing to participate. These people may also be less willing to perform a lung function test, leading to more favourable outcomes. However, we tried to minimise selection bias by randomly selecting the participants. Second, participants were between the age of 55-65 years. Despite the limited variance in age, results are in accordance with previous research in other countries. Therefore, it is expected that the results are representative, though one should be careful in generalising to other age groups. Third, comorbidities and a former diagnosis of COPD were self-reported. Also, COPD was defined as a self-reported diagnosis of chronic bronchitis, asthma, emphysema, or COPD. Initially, it is a disadvantage that the diagnosis is self-reported as it is less accurate than the original diagnosis of the doctor. Besides that, no distinction was made between the various respiratory diseases. This makes it impossible to specify whether the participant was diagnosed with chronic bronchitis, asthma, emphysema or COPD.
CONCLUSION
A new CAT cut-point of > 18 points is suggested to indicate an impaired health status in patients with COPD, as approximately one in five non-COPD subjects have abnormal CAT scores according to current international standards. These normative values should be taken into account when applying the updated GOLD assessment to Dutch COPD patients in clinical practice.
ACKNOWLEDGEMENTS
We are grateful to all the respondents who were willing to participate in the current study. Subsequently, the authors would like to thank M. Akkermans and J. Oosterbaan for helping with collecting and converting the spirometry data. The Longitudinal Aging Study Amsterdam was financially supported by the Ministry of Health, Welfare and Sports (to the VU University for the The Longitudinal Aging Study Amsterdam). DES was financially supported by GlaxoSmithKline (SCO115406). The funding sources had no involvement in the study design, data collection, analysis and interpretation of data, writing of the report, and/or decision to submit the article for publication.
DISCLOSURES
The authors have nothing to disclose.
REFERENCES