KEYWORDS
Acute dialyser reaction, anaphylaxis, haemodialysis, polysulfone membrane, polyethersulfone membrane
INTRODUCTION
In the last decades of the previous century, acute dialysis reactions were common in patients treated by haemodialysis. They were related to the use of bio-incompatible, complement-activating dialyser membranes (often combined with hypoxia-inducing acetate-containing dialysate), ethylene-oxide (EtO) sterilisation of dialysers that caused IgE-mediated hypersensitivity or exposure to polyacrylonitrile (PAN) membranes that stimulated the production of bradykinin.1 However, even in the current era, in which biocompatible dialysers are being used, bicarbonate has replaced acetate as a dialysate buffer and EtO sterilisation has been abandoned, occasional cases of acute dialyser reactions continue to be reported, also recently.2,3
We describe recent acute dialyser reactions in two patients treated by a polysulfone, steam sterilised dialyser. These cases prompted us to review the literature on acute dialyser reactions in the last decade to define their clinical characteristics, develop a management strategy and increase awareness of this potentially serious adverse event.
Patient 1
A 74-year-old male (diabetic nephropathy) was treated with haemodialysis with an F8-HPS polysulfone dialyser (Fresenius®). He was on an ACE inhibitor and aspirin. In February 2012, after seven months of stable treatment, he complained of dyspnoea immediately after starting dialysis. A week later he reported similar symptoms and abdominal pain four minutes after starting dialysis. His blood pressure dropped from 177/89 mmHg to 112/52 mmHg and the oxygen saturation was 91%. An ECG showed no arrhythmias or ischaemia. The ACE inhibitor was stopped. Thirty minutes into the next dialysis, dyspnoea and abdominal pain developed abruptly. The blood pressure was 180/100 mmHg and arterial pO2 was 50 mmHg. Blood chemistry did not show haemolysis or infection and a chest X-ray was normal. During one of the episodes, the eosinophil count was elevated (1.29 x 109/l, normal < 0.40 x 109/l), but values of 0.68 and 0.87 x 109/l were measured during two other episodes, when platelet counts (245 and 290 x 109/l, respectively) were also within the normal range. We considered an allergic reaction to dalteparin (Fragmin®, Pfizer), the only drug given prior to the dialysis sessions. Despite switching to danaparoid (Orgaran®, Merck Sharp & Dohme), the dyspnoea occurred 30 minutes into the next dialysis. The blood pressure dropped abruptly from 132/60 mmHg to 98/54 mmHg and the pO2 fell from a predialysis value of 88 mmHg to 55 mmHg (changes in O2 saturation and pCO2 from 97% to 87% and from 37 mmHg to 40 mmHg, respectively). Suspecting an allergic reaction to the F8-HPS dialyser, we switched to a dialyser with a different membrane, the Sureflux 150-L (Nipro®, cellulose triacetate) for the next dialysis. During this session, the patient remained asymptomatic and blood pressure, pO2 and O2 saturation remained stable within the normal range. The patient agreed to a rechallenge with the F8-HPS dialyser, which resulted in direct recurrence of dyspnoea. We interrupted the session immediately and restarted dialysis using the Sureflux 150-L dialyser, after which the symptoms abated. Dialysis sessions with the cellulose triacetate (CTA) dialyser were uneventful with a follow-up extending to December 2015.
Patient 2
A 69-year-old male (diabetic nephropathy) started haemodialysis in November 2015 using an F8-HPS polysulfone dialyser (Fresenius®). He was not on an ACE inhibitor, β-blocker or aspirin. The first two sessions were uneventful, the patient tolerating 1.8 litres of ultrafiltration and a 12% reduction in relative blood volume. During the 3rd dialysis, he started vomiting and briefly lost consciousness after 40 minutes. The blood pressure, which was 150/60 mmHg at the start of dialysis, was 129/65 mmHg shortly after the incident. Ultrafiltration had been 0.3 litres up to the incident, but there was no reduction in relative blood volume (change + 0.4%). An ECG showed no arrhythmias, the plasma troponin was normal. Dialysis was stopped. The next dialysis, performed without ultrafiltration, was uneventful. During the 5th dialysis, the patient became unwell after 50 minutes. His blood pressure, which was 155/76 mmHg at the start of dialysis, had fallen to 66/26 mmHg, despite zero ultrafiltration. During the 6th dialysis, the patient became unwell after 45 minutes and the blood pressure fell to 86/39 mmHg, although the ultrafiltration rate had been set to zero from the start of dialysis. After two uneventful sessions, he became hypotensive (blood pressure 70/40 mmHg) with severe nausea and vomiting after 30 minutes during the 9th dialysis. Up to this point, no volume had been removed by ultrafiltration. The tentative diagnosis of acute dialyser reaction was made and the patient was switched to a Sureflux 150-L dialyser (Nipro®, cellulose triacetate). The remainder of the dialysis sessions went without incident. After 20 uneventful dialysis sessions using the Sureflux dialyser, the patient was accidentally treated with an F8-HPS dialyser, and he became unwell and hypotensive (blood pressure 94/46 mmHg) 50 minutes into dialysis. The total follow-up after switching to the CTA dialyser is three months, in which the patient has remained asymptomatic. Unfortunately, no eosinophil or platelet counts were obtained during any of the acute dialyser reactions.
SUMMARY OFRECENT CASE REPORTS ON ACUTE DIALYSER REACTIONS
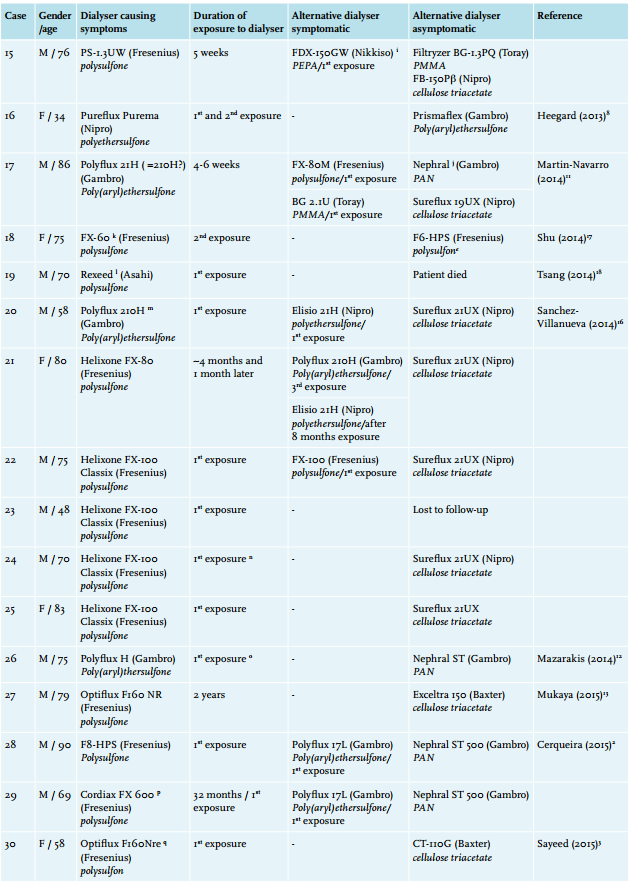
We found 30 cases of acute dialyser reactions in the literature since the beginning of the current century,2-19 bringing the total to 32 cases (table 1). The mean patient age was 68.7 years (range 34-90 years), and 56.3% were males. In 17/32 cases (53.1%), reactions occurred in the first week after starting exposure to the offending dialyser, most often after the first contact. In the remaining 15 cases, however, the interval between first exposure to the dialyser and occurrence of symptoms was considerably longer (mean 11 months, range 1 to 36 months). In 24/32 cases (75.0%), the reactions occurred within the first 30 minutes of dialysis. In the remaining cases, symptoms occurred between 45 and 120 minutes after starting dialysis or became manifest very gradually. Reported manifestations were dyspnoea (69%), hypotension (66%), hypoxia (44%), bronchospasm (25%), chest pain (22%), pruritus and/or urticaria (22%) and abdominal symptoms (22%). Severe laryngeal oedema or stridor occurred twice. Cardiorespiratory arrest occurred six times (19%), and two patients (6%) died.
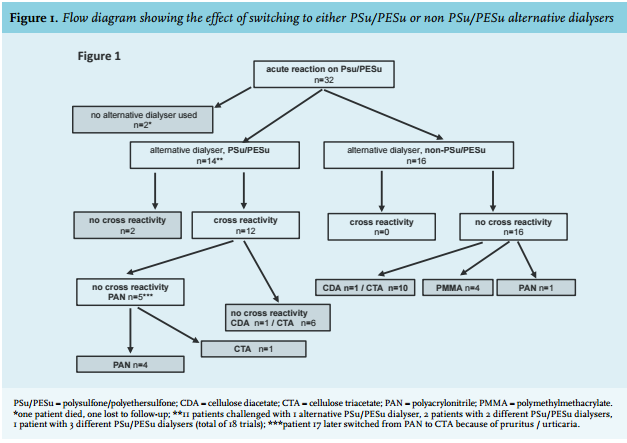
Table 1 shows that all dialysers that induced acute reactions contained membranes of the polyarylsulfonate family,20 which includes polysulfone (PSu, 28 cases, 87.5%) and poly(aryl)ethersulfone (PESu, 4 cases, 12.5%). Fourteen patients were subjected to a different PSu/PESu containing dialyser at some point with a total of 18 trials (figure 1). In 16/18 (88.9%) of these trials (in 12/14 patients, 85.7%), acute dialyser reactions occurred, virtually always during the first exposure. Only two patients (case 16 & 18) could be treated successfully with an alternative PSu/PESu containing dialyser.8,17 Cross-reactivity between PSu/ PESu dialysers was extensive, both within membrane type (PSu vs. PSu or PESu vs. PESu, respectively), between membrane types (PSu vs. PESu) and within and between brands (table 1).
Figure 1 shows that of the 12 patients that showed cross-reactivity to a PSu/PESu dialyser, eight (66.7%) were eventually treated without problems with a dialyser containing modified cellulose, and four switched successfully to a PAN dialyser. Of the 16 patients that were not rechallenged with an alternative PSu/PESu dialyser, 11 reacted favourably to substituted cellulose, four to a dialyser containing a polymethylmethacrylate (PMMA) membrane and one patient returned to the PAN containing dialyser he had used previously.
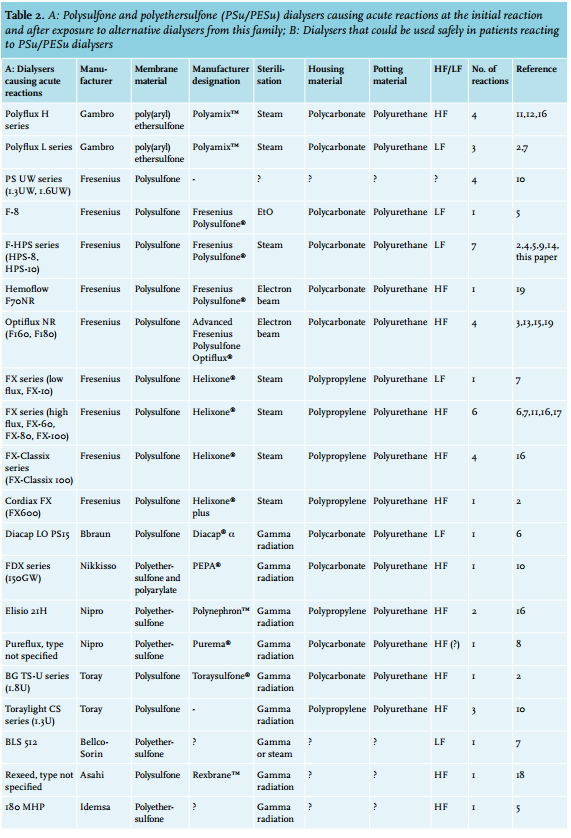
Table 2A summarises the PSu/PESu containing dialysers (n = 20) that caused the initial acute dialyser reactions (n = 32) as well as the cross-reactions (n = 16). They differed in sterilisation method, housing material and hydraulic permeability. For instance, steam (35%), gamma radiation (45%) and electron beam sterilisation (10%) were all applied. Polycarbonate and polypropylene were used as housing materials, and both high flux (13/20, 65%) and low flux (6/20, 30%) dialysers are listed. All dialysers contained polyurethane as a potting substance, but this material was also used in all non-PSu/PESu dialysers that did not cause acute dialyser reactions in patients reacting to PSu/PESu (table 2B).
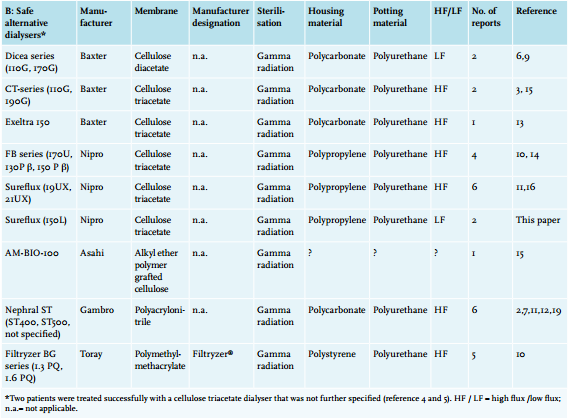
Table 2B lists the non-PSu/PESu dialysers that could be used safely in patients reacting to PSu/PESu membranes. With regard to the sterilisation method, housing and potting material and hydraulic permeability characteristics, they overlap with the PSu/PESu dialysers in table 2A. The only conspicuous distinguishing feature is the difference in membrane materials.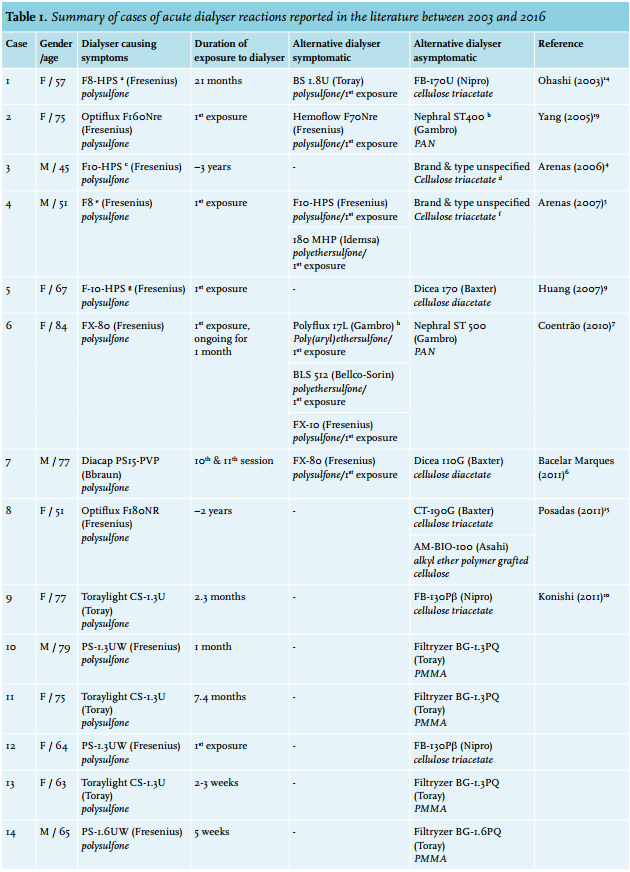
DISCUSSION
We report two patients with acute dialyser reactions that occurred when using a PSu dialyser. They became asymptomatic after switching to a CTA dialyser. Supporting the notion that the dialyser reactions were caused by the PSu membrane, both patients immediately developed symptoms after intentional (patient 1) and accidental (patient 2) rechallenge with the PSu dialyser.
Thirty additional cases of acute dialyser reactions were found in the literature dating from the beginning of the current century,2-19 an era in which the use of biocompatible, non-EtO sterilised dialysers has become standard practice. The reactions usually occur within the first 30 minutes of dialysis, are characterised by severe cardiopulmonary symptoms and fit the diagnostic criteria of anaphylaxis.21 Interestingly, acute dialyser reactions occurred shortly after the initial exposure to the offending dialyser in only half of the reports, the average delay being almost a year in the remaining cases.
All reactions were caused by dialysers that contained a polyarylsulfonate membrane, which includes PSu and polyethersulfone (PESu).20 About half of the patients were re-exposed to a PSu/PESu dialyser that differed from the original offending PSu/PESu dialyser. Repeat acute reactions occurred in 85% of them, forcing a switch to a non-PSu/PESu dialyser. The remainder of the patients were not exposed to a different PSu/PESu dialyser but switched directly to a non-PSu/PESu dialyser. Overall, of the patients reacting to PSu/PESu dialysers that had follow-up (n = 30), two were continued on an alternative PSu/PESu dialyser. The vast majority were switched to non-PSu/PESu dialysers, including modified cellulose dialysers (n = 19, mainly CTA), a PAN dialyser (n = 5) or a PMMA dialyser (n = 4).
PSu/PESu dialysers that provoked acute reactions differed in hydraulic permeability, sterilisation method and housing material. All contained polyurethane as potting material, but this was also the case for the non-PSu/PESu dialysers shown to be safe in patients reacting to PSu/ PESu. This leaves the membrane material as the only recognisable common factor (table 2A). In the patients that were rechallenged with an alternative PSu/PESu dialyser, cross-reactivity was extensive, within membrane type (PSu vs. PSu or PESu vs. PESu), between membrane types (PSu vs. PESu) and within and between brands (table 1). Neither the various PSu nor the different PESu containing dialysers are identical products, as the capillary walls may differ in thickness, geometry, layering and luminal smoothness as well as in pore size and pore size distribution.22 This suggests that an essential determinant of the basic PSu and PESu polymers causes the acute reactions.
One explanation for the finding that PSu/PESu dialysers caused all reported initial dialyser reactions could be that approximately 93% of dialysers currently used contain PSu/PESu,23 leading to exposure of many more patients to these dialysers than to those containing CTA, PAN or PMMA. However, recent research also suggests that PSu and CTA dialysers differ in biocompatibility. Dialyser protein adsorption patterns differ in asymptomatic dialysis patients exposed to a PSu and CTA dialyser in that the former, but not the latter, adsorbed ficolin-2, a substance that may directly activate the complement system via the lectin pathway.24 A similar study suggested that CTA was more biocompatible than PSu in terms of activation of the coagulation cascade.25 In agreement with this, a PSu membrane, but not a CTA membrane, caused a substantial increase in indicators of platelet activation in asymptomatic dialysis patients26 or patients with acute renal failure treated by continuous venovenous haemofiltration.27 Consistent with this, dialysis-induced thrombocytopenia provoked by a PSu dialyser resolves after switching to a CTA (or PAN) dialyser.28,29 These observations suggest that PSu dialysers confer an increased risk of acute reactions compared with those containing CTA. Unfortunately, PAN and PMMA dialysers have not been compared directly with those containing PSu or CTA using the same analytical methods.
Our observations suggest that the dialysers containing modified cellulose, PAN and PMMA shown in table 2B can be used unreservedly in patients reacting to PSu/ PESu dialysers. However, this protective effect may not be complete and acute reactions are not restricted entirely to PSu/PESu dialysers. Patient 3 reacted to a PSu dialyser and switched successfully to a CTA dialyser, only to develop acute reactions several weeks later. Patient 17 reacted to a PESu and a PSu dialyser, but also to a PMMA dialyser. A PAN dialyser caused urticaria and eosinophilia necessitating a switch to a CTA membrane. Hanada et al. reported a patient reacting from his first dialysis to dialysers containing CTA, PSu, vitamin E coated PSu, PMMA, polyester polymer alloy and ethylene vinyl alcohol copolymer (EVAL) who could only be dialysed using a CTA dialyser combined with temporary corticosteroids.30 Quinones et al. reported a patient having acute reactions to both a PSu dialyser and one containing EVAL.31 Consequently, some patients also appear to be prone to anaphylactic reactions to dialyser membranes other than PSu/PESu, suggesting an important interaction between membrane biocompatibility and patient-related factors. Indeed, the severity of anaphylactic reactions can be affected by co-factors, both patient specific and non-specific.32 The latter include infections, common in patients on dialysis, and drugs often used by dialysis patients such as acetylsalicylic acid, β-blockers and ACE inhibitors.33 Interestingly, although the detrimental effects of ACE inhibitors were specifically linked to PAN membranes,34 the patient described by Quinones et al. only had acute reactions to both the PSu and the EVAL dialyser during ACE inhibition.31 Consequently, it is worthwhile to pay attention to potential modifiable factors in patients reacting to dialysers.
It is of note that eight cases of acute reactions to surface-treated PAN dialysers (Nephral-ST) have been reported in patients on ACE inhibitors.35-38 Reactions to dialysers containing the original PAN membranes with their very negatively charged, bradykinin-inducing surface have been reported in patients on ACE inhibitors.34 Membrane surface treatment with polyethyleneimine was used to reduce membrane electronegativity and prevent this complication.39 However, no cases of a reaction to a Nephral-ST dialyser, attributed to incomplete PEI coating, have been reported after 2007.38
The number of patients on haemodialysis throughout the world has increased from approximately 1.5 to 2.5 million in the past decade.40 Consequently, hundreds of millions of dialysers are being used annually, the vast majority of which contain PSu/PESu. With only 32 contemporaneous reported cases of acute reactions to PSu/PESu dialysers, their verified incidence is extremely low, although underreporting is likely. Interestingly, 85% of the cases summarised in this paper were reported in or beyond 2010, suggesting an increasing trend. This rise could be related to increased awareness or reflect the increasing number of patients being treated. However, it is also possible that ongoing modifications to the original PSu membrane developed in the early 1980s,41 aimed at enhancing dialyser performance, may also negatively affect dialyser biocompatibility. In this context, the Urgent Field Safety Notice issued by Fresenius in 2015 for the new line of FX CorDiax High-Flux dialysers and haemodiafilters (PSu, Helixone®) may be relevant,42 as this notice was spurred by ‘an increased number of cases of hypersensitivity and hypersensitivity-like reactions with the application of the FX CorDiax dialysers, including life-threatening events during continuous post market surveillance’.
Although rare, acute dialyser reactions are not a thing of the past and dialysis staff should be aware of them as the incidence may be increasing. They should be considered in patients on haemodialysis using PSu/PESu dialysers who develop cardiopulmonary signs and symptoms in the early phase of dialysis sessions for which no alternative explanation is readily available. These include cardiac failure or ischaemia, arrhythmia, ultrafiltration-related dialysis hypotension or allergic reactions to drugs that are given intravenously prior to dialysis. As ~85% of patients reacting to a PSu/PESu containing dialyser will also react to other dialysers of the same family, we suggest that they should not be challenged with alternative PSu/PESu dialysers if the diagnosis is suspected. It seems advisable to switch them directly to a non-PSu/PESu dialyser, which should immediately and consistently lead to disappearance of symptoms. Most experience is available with CTA dialysers, but alternatives include those containing PAN or PMMA.
DISCLOSURES
The authors have no conflicts of interest to disclose.
REFERENCES