KEYWORDS
Clindamycin, adverse drug reaction, acute generalised exanthematous pustulosis (AGEP), spontaneous reporting system, reporting odds ratio
INTRODUCTION
Besides lincomycin, clindamycin is the only marketed antibiotic of the lincosamide group. Primarily, it has a bacteriostatic action against Gram-positive aerobic and a wide range of anaerobic bacteria. It binds to the 50S rRNA subunit of the bacterial ribosome, similarly to macrolides such as erythromycin, and inhibits the early stages of protein synthesis. However, it is not chemically related to the macrolides.1 The adverse drug reaction (ADR) profile of clindamycin is similar to that of most antibiotic drugs regarding frequently occurring diarrhoea, nausea/vomiting and rash.
Acute generalised exanthematous pustulosis (AGEP) is a rare but serious acute pustular reaction pattern characterised by pin-point, sterile, non-follicular pustules on a bright erythematous, oedematous background and a distinctive histopathology (figures 1 and 2).2,3 Mild, non-erosive mucous membrane involvement (mostly oral) may occur in about 20% of cases. Other skin symptoms, such as marked oedema of the face, purpura, ‘atypical target-like lesions’ and blisters have been described but are not typical for AGEP. In most cases, the course of AGEP is characterised by fever (≥ 38 °C) and peripheral neutrophilia (≥ 7.0 x 109/l); mild eosinophilia may be present in about one-third of the patients. Visceral internal organ involvement may occur and is generally restricted to mild and transient liver and/or kidney involvement. After withdrawal of the culprit, pustules resolve spontaneously within a few days, typically followed by post-pustular desquamation, while total recovery is usually within 15 days. The overall prognosis in AGEP is good although high fever and superinfection of skin lesions can sometimes lead to life-threatening situations in patients of old age or in a poor general condition.2 The reported mortality is 1-5%. More than 90% of cases of AGEP are drug-induced, with antibiotics being the most frequent triggers. A high proportion of these cases have been attributed to beta-lactams or macrolides, but interestingly not to sulphonamides which have a high potential for causing serious cutaneous ADRs. AGEP has also been ascribed to a wide variety of other drugs, including antimycotics, calcium channel blockers, carbamazepine and acetaminophen.2,4,5 In a minority of cases other causes, in particular viral infections, have been suspected to trigger AGEP.2
Clindamycin has been associated with serious cutaneous ADRs such as Stevens-Johnson syndrome, toxic epidermal necrolysis and drug reaction with eosinophilia and systemic symptoms. Notwithstanding emerging evidence of a link between clindamycin and AGEP, knowledge about this association is, however, still limited.6-14
The five case reports received by the Netherlands Pharmacovigilance Centre Lareb add to the current knowledge on this relationship. Additionally, to strengthen this association we summarise the cases in the database of the WHO Collaborating Centre for International Drug Monitoring, the Uppsala Monitoring Centre (Vigibase™), and the database of the European Medicine Agency (Eudravigilance). Furthermore, we performed a literature review of the cases of AGEP, associated with clindamycin.
METHODS AND MATERIALS
Lareb maintains the spontaneous ADR reporting system in the Netherlands. The reports associated with clindamycin and AGEP submitted to Lareb until October 2015 are described. Extensive narratives with additional clinical information for the cases of interest were obtained from the reporters. The reports from Vigibase™ and Eudravigilance until September 2015 and 26 October 2015, respectively, are summarised. Subsequently, the reports submitted by Lareb, Vigibase™ and Eudravigilance are analysed for disproportional reporting. ADRs are coded according to the Medical Dictionary for Regulatory Activities (MedDRA®; version 17.0) and the suspected drugs are classified according to the WHO Anatomical Therapeutic Chemical classification system. Cases were defined as reports mentioning the MedDRA® Preferred Term acute generalised exanthematous pustulosis associated with clindamycin. The control group consisted of all other reports in the databases.
The strength of the association between AGEP and the use of clindamycin is calculated using the reporting odds ratio (ROR), with corresponding 95% confidence intervals (CI), as a measure of disproportionality. In instances where the ROR is statistically significant, AGEP is more frequently reported than could be expected. In order to compare the data of Lareb and Vigibase™ more easily, the measure of disproportionality of Vigibase™ (Bayesian Confidence Propagation Neural Network) was converted to ROR.
Finally a PubMed search was conducted in October 2015 using the keywords “clindamycin”, “AGEP”, “acute generalised/generalised exanthematous pustulosis”. Relevant English-language case reports were included and references of retrieved publications were screened for relevant literature. Cases with a possible or lower rate of causality for clindamycin were excluded.
RESULTS
Lareb reports
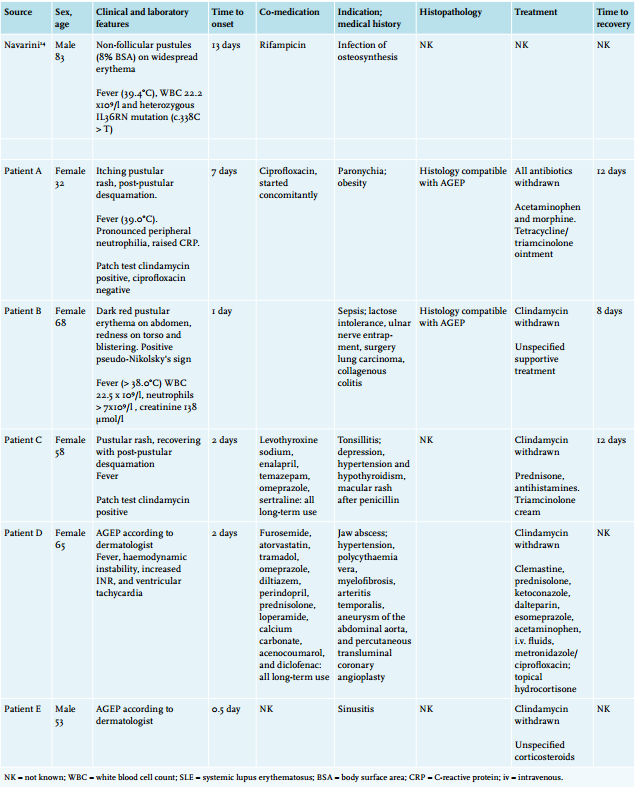
Until October 2015, Lareb received 165,000 reports, including five of AGEP associated with the use of clindamycin. The details of the latter are described below. Patient A (2015), reported by a dermatologist, concerns a 32-year-old female with AGEP after seven days use of clindamycin for paronychia. Due to high fever (39.0°C), painful toes, itching pustular rash, raised C-reactive protein (CRP) and pronounced peripheral neutrophilia, the patient was hospitalised for seven days. The patient was treated with topical tetracycline, triamcinolone ointment, paracetamol and morphine. Clindamycin was withdrawn and the patient recovered 12 days later with post-pustular desquamation. The only concomitant medication was ciprofloxacin, which was started and withdrawn at the same time as clindamycin. Histology was typical for AGEP, while epicutaneous testing was positive for clindamycin and negative for ciprofloxacin.
Patient B (2015), reported by a dermatologist, concerns a 68-year-old female with AGEP with some toxic epidermal necrolysis-like features after one day of clindamycin for sepsis. A dark red pustular erythema on the abdomen, redness on the torso, blistering on the back, and a positive pseudo-Nikolsky’s sign were observed. Histopathology was compatible with AGEP. The patient experienced high fever (> 38°C) and laboratory examination revealed a white blood cell count of 22.5 x 109/l, neutrophilia, a raised creatinine of 138 µmol/l and normal transaminases. The lesions had almost recovered eight days after withdrawal of clindamycin and unspecified supportive treatment. Total recovery took 4-6 weeks, due to concomitant disease. The patient’s medical history indicated lactose intolerance, ulnar nerve entrapment, lung carcinoma surgery and collagenous colitis.
Patient C (2013), reported by a dermatologist, concerns a 58-year-old female with a history of hypothyroidism, hypertension and depression, for which she used levothyroxine sodium, enalapril, temazepam, omeprazole, and sertraline, all long term and without adverse reaction. Several years previously, she had experienced a macular rash after penicillin; two days after a clindamycin infusion, followed by oral clindamycin for tonsillitis she was hospitalised for a pustular rash and fever, treated with prednisone, antihistamines, and triamcinolone cream. Twelve days after withdrawal of clindamycin, the patient had recovered with post-pustular desquamation. Three months later, the patient had a positive skin patch test for clindamycin.
Patient D (2012), reported by a physician of internal medicine, concerns a 65-year-old-female with a history of hypertension, polycythaemia vera, myelofibrosis, arteritis temporalis, aneurysm of the abdominal aorta, and percutaneous transluminal coronary angioplasty. Two days after the start of clindamycin for a jaw abscess she experienced AGEP with haemodynamic instability, fever, increased INR, and ventricular tachycardia. The diagnosis of AGEP was confirmed by a dermatologist. The patient was admitted to the hospital and recovered after withdrawal of clindamycin, and treatment with clemastine, prednisolone, intravenous fluids, intravenous metronidazole/ciprofloxacin, topical hydrocortisone acetate, ketoconazole, dalteparin, esomeprazole and paracetamol. Concomitant medications at the time of the event, all used long term and without adverse reaction, were furosemide, atorvastatin, tramadol, omeprazole, diltiazem, perindopril, prednisolone, loperamide, calcium carbonate, acenocoumarol and diclofenac.
Patient E (2005) was reported by a 53-year-old male consumer who was a health professional himself and had a history of mastocytosis. The patient experienced AGEP, 12 hours after starting clindamycin because of sinusitis. The diagnosis of AGEP was confirmed by a dermatologist. He recovered quickly after withdrawal of the clindamycin and treatment with corticosteroids. Concomitant medication was not reported. 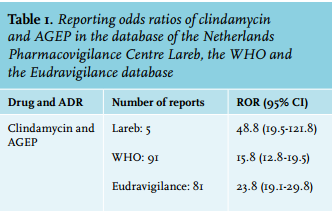
Disproportionality analysis
On 1 October 2015, the Lareb database contained 165,000 reports, including 235 reports of ADRs associated with clindamycin, among which five reports associated with AGEP as described above. Vigibase™ contained a total of 11.8 million reports of ADRs, including 25,659 cases associated with clindamycin. Among these cases, 91 cases concerned AGEP, including 26 males, 62 females and three cases of unknown gender. Ages varied from 2 to over 75 years. Positive dechallenge and rechallenge were reported in 54 cases and 1 case, respectively. On 26 October 2015, Eudravigilance contained 4.2 million reports, including 5518 reports of ADRs associated with clindamycin among which 81 reports of AGEP. As shown in table 1, the association of clindamycin with AGEP was significant in all databases.
Literature review
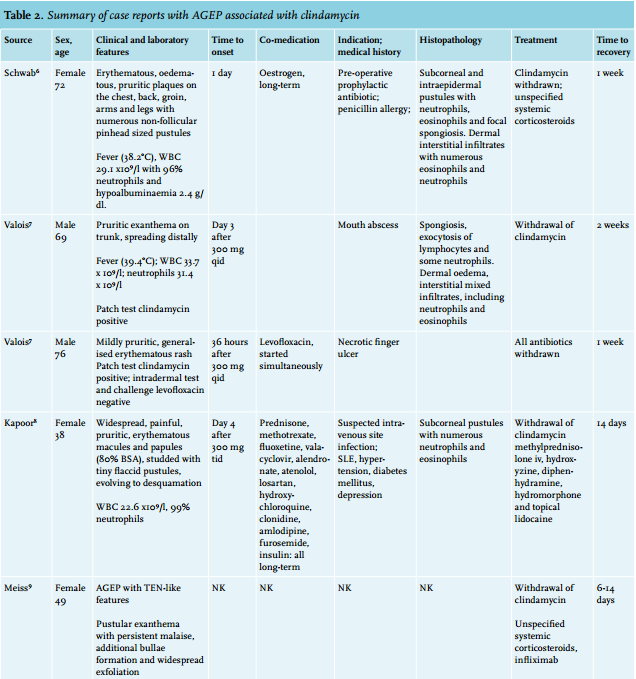
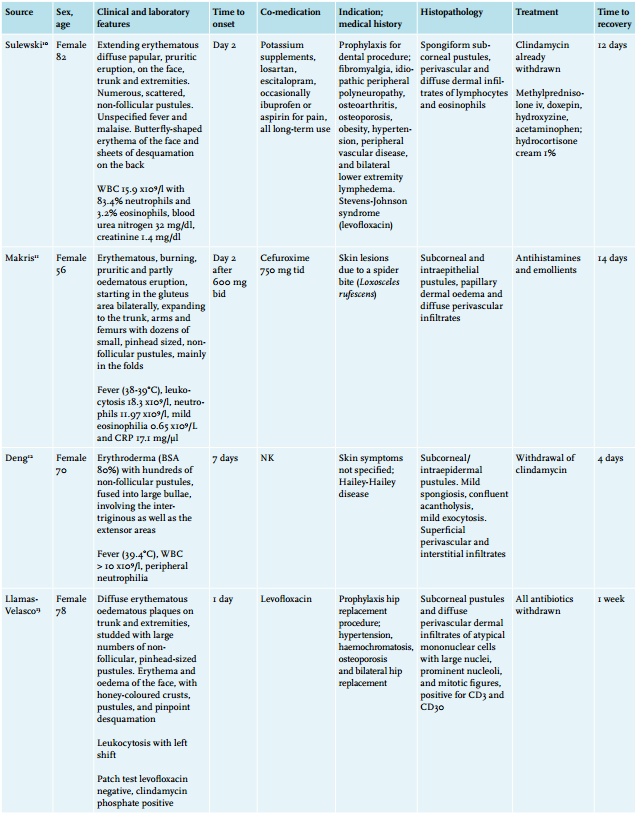
Up until now, nine reports with ten cases of AGEP, probably induced by clindamycin, have been published in the English language literature.6-14 These cases concerned seven females (age 72, 38, 49, 82, 56, 70, and 78 years) and three males (age 69, 76 and 83 years). The latency time between the start of clindamycin and onset of the symptoms of AGEP in most cases was within a few days. Only in the cases from Deng et al. and Navarini et al. was time to onset longer: 7 and 13 days, respectively. All cases showed resolution of the pustules in less than 15 days; in three the relation between AGEP and clindamycin was supported by a patch test.7,13 Histopathological findings were concordant with AGEP. Clinical findings including patient details, laboratory features, time of onset, treatment and recovery of AGEP are summarised in table 2.
DISCUSSION
AGEP is a rare, most often drug-induced, serious pustular reaction pattern, characterised by an acute onset and typical clinical picture and course. In 2001, a standardised validation score system was proposed, taking into account the morphology of the lesions, the course of the disease, and laboratory and histopathological features.2 AGEP is considered to be a subtype of a delayed hypersensitivity type IV reaction with a role for both CD4+ (helper) and CD8+ (cytotoxic) T cells.15,16 The latency period between the administration of drugs and onset of AGEP is typically short, most often within 1-3 weeks after starting the causative drug. Yet in the group of anti-infective drugs the time to onset may be as short as a few hours to three days.2 The culprit drug in AGEP can regularly be confirmed by a positive patch and/or lymphocyte transformation test with the suspected drug.17
We describe five further cases of clindamycin-induced AGEP. Moreover, we show that the association between clindamycin and AGEP is statistically supported by the Lareb database, Vigibase™, and Eudravigilance by a significantly raised ROR. Of note is that the cases from the Lareb database are included in Vigibase™ and Eudravigilance. A reporting disproportionality for a specific drug-ADR combination, detected by spontaneous reporting of ADRs, plays an important role in providing early signals for detecting new ADRs in the post-marketing phase. The statistical relevance of a raised ROR will be more reliable if the number of cases on which it is calculated is higher. However, the clinical relevance of these reporting systems is limited to the assumed existence of a certain association, although they can contribute to more knowledge of the nature and incidence of ADRs in daily practice. The quality of information and causality of the reported drug-ADR association of an individual report in spontaneous reporting systems can vary substantially. Disproportionality analysis is hypothesis generating and can indicate where harm might be, but to confirm and/or quantify harm, one has to rely on case reports or series or use other pharmacoepidemiological methods.
Our cases, all confirmed by a dermatologist, provide further support for the association of clindamycin with AGEP. The relatively short time to onset is consistent with drug-induced AGEP. Median latencies for the Lareb and the published cases were 2 days (0.5-7 days) and 2 days (1-13 days), respectively. In all cases the patients recovered without reported sequelae after withdrawal of clindamycin. In addition, all the described cases met the criteria for full recovery of AGEP within 15 days. Lareb case B describes a patient with AGEP associated with some toxic epidermal necrolysis-like features, with a prolonged recovery time of 4-6 weeks due to other disease. Toxic epidermal necrolysis-like features in AGEP, resulting from coalescence of pustules, sometimes accompanied by more severe visceral organ involvement and haemodynamic instability, have been reported before.18 It should be noted that patient D concomitantly used diltiazem, which is strongly associated with AGEP.19 However, since it was used long-term, causality was unlikely. Although AGEP has rarely been associated with infectious diseases, particularly of viral aetiology, it is unlikely that underlying diseases were causative in our cases. No association between mastocytosis and AGEP could be found in the literature. As the cases described by Valois et al. and Llamas-Velasco et al., Lareb case A and C were confirmed by a positive patch test. Information extracted from the Lareb cases and the published case reports in the literature shows that different kinds of treatments are being applied. However, as AGEP is a self-limited disease, the mainstay of treatment is withdrawal of the suspected culprit and supportive therapy such as topical and/or systemic corticosteroids, antihistamines and sometimes antibacterial agents. Use of systemic steroids, however, has not yet been sufficiently evidenced in the literature.
In conclusion, we report five cases of AGEP associated with the use of clindamycin. We reviewed the literature on similar case reports and performed a case/non-case analysis in Vigibase™, the Eudravigilance database and the Lareb database. AGEP should be considered a rare, but possible, serious cutaneous adverse drug reaction of clindamycin.
DISCLOSURES
All authors declare that they have no conflict of interest. No financial support was received for the conduct of this study or preparation of this manuscript.
REFERENCES