KEYWORDS
Day care surgery, hemithyroidectomy, patient safety, surgical outcomes
INTRODUCTION
Hemithyroidectomy is the most common endocrine surgical procedure performed in daily practice and indicated mainly due to mechanical and/or cosmetic complaints of a multinodular goitre or a solitary thyroid nodule. Furthermore, it is performed for diagnostic purposes in case of indeterminate cytology. Despite the increased rate of day care surgical procedures, thyroid surgery in the Netherlands is currently solely performed with overnight stays. It is assumed that the potential risk of life-threatening respiratory problems caused by postoperative bleeding, laryngeal nerve injuries or hypocalcaemia warranting (intravenous) supplementation are reasons for which thyroid surgery is not performed in the day care setting. Recently, Segel et al.1 published their results regarding over 1000 thyroidectomies in the outpatient setting. The most feared complication, acute postoperative haemorrhage with a potentially life-threatening airway obstruction, did not occur. In general, the incidence of postoperative bleeding varies between 0.1-1.1%, and seldom causes acute airway problems or need for reinterventions.2 In addition, laryngeal nerve injury after hemithyroidectomy is uncommon and the literature reports incidence rates of up to 3.7% of patients, with 0.4% permanent injuries to the laryngeal nerve.3-7 Temporary hypocalcaemia occurred in about 3% of the outpatient patients treated in Segel’s study.1 Wound infection occurs in less than 1% of the patients, but is a late complication and poses no threat in the day care setting.4,6
Worldwide, the number of outpatient thyroidectomies has increased by 39% over the last ten years.8 Technological advancements in anaesthesia care and the widespread introduction of minimally invasive surgical techniques have fuelled this trend. The first report regarding thyroid surgery in the day care setting by Steckler dates back to 1986.9 Since then, multiple studies have shown that day care thyroid surgery is safe and feasible with regard to hemithyroidectomy and even total or completion thyroidectomy.1,2,4-7,10-13 The American Thyroid Association published a statement regarding outpatient thyroid surgery describing important safety criteria for selecting eligible patients.14
Given all the encouraging reports it is peculiar why day care thyroid surgery is not yet implemented in the Netherlands. One can only assume that the risk, albeit utterly small, of losing a patient due to respiratory distress caused by massive bleeding after discharge is the main reason. Therefore our first aim was to assess the safety of thyroid surgery in our institution by means of a retrospective risk analysis of all patients who underwent hemithyroidectomy in a five-year period from 2010 to 2014. Then we present the initial results of implementing day care thyroid surgery in our daily practice, strictly adhering to the international guidelines.14
METHODS
All patients were operated in the ‘Reinier de Graaf Gasthuis’ in Delft, a non-academic teaching hospital in the Netherlands, by one of two dedicated endocrine surgeons (P.C.S and F.M.G.). The retrospective cohort (part A) consists of all consecutive patients who underwent primary hemithyroidectomy between January 2010 and December 2014. These patients were identified by means of surgical codes from the hospital software system. All electronic patient charts were reviewed and baseline characteristics, medical history, indication for surgery, postoperative complications and hypothetical eligibility for day care surgery were noted. Complications were retrieved by manually checking the charts in conjunction with checking our prospective database where all operations and complications are prospectively recorded. The data were analysed and an overall judgement was made regarding the safety of day care thyroid surgery in our hospital. All patients in the retrospective cohort who were eligible for day care surgery14 but received necessary in-hospital interventions from six hours to 24 hours postoperatively are considered ‘day care safety failures’. As no ‘day care safety failures’ occurred, we proceeded to part B of the study: implementation of day care surgery.
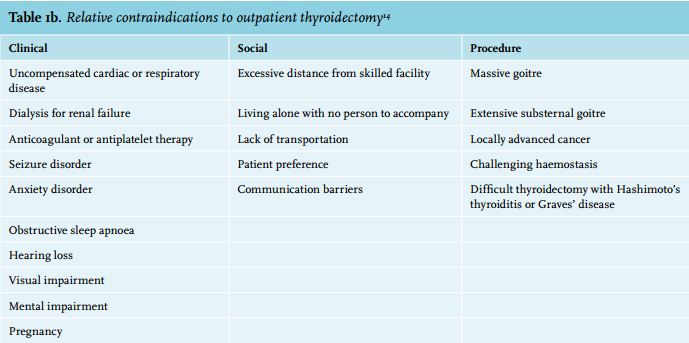
All patients scheduled for their first hemithyroidectomy in 2015 were included in the prospective cohort (part B). Baseline characteristics, medical history, indication for surgery and postoperative complications were prospectively collected. All patients were assessed for eligibility for day care surgery according to the criteria published by the American Thyroid Association,14 as listed in table 1.
Patients eligible for day care surgery and willing to participate were discharged the same day at least six hours after skin closure with the permission of the surgeon and consent from the patient. All patients received information about the surgical procedure, a letter addressed to the general practitioner and standardised discharge instructions when discharged. These instructions provided information regarding pain and pain medication, wound dressings and signs of infection. Patients were instructed to contact the hospital in case of, but not limited to, voice changes, stridor, swelling of the wound and/or problems swallowing. All patients were contacted by telephone one day after discharge. Two weeks after surgery all patients were seen at the outpatient clinic for their first postoperative check-up. Hereafter, patients were referred back to their treating endocrinologist.
Statistical analysis was done using IBM SPSS software (version 21). Descriptive analysis is performed, where categorical data are expressed as frequency with percentage, and nominal data are expressed as mean with standard deviation. Group differences were analysed with the Chi-square test for categorical data, and the unpaired t-test for nominal data. Significant differences are defined as p < 0.05. 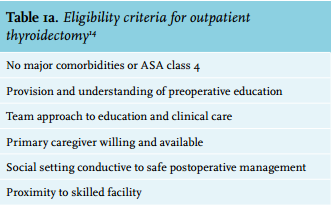
RESULTS
Retrospective cohort
A total of 210 patients were included in our retrospective risk analysis cohort, of which 149 patients (71.0%) were eligible for day care surgery. Baseline characteristics and complication rates are summarised in table 2. Patients eligible for day care surgery were significantly younger (48 vs 55 years, p = 0.001) and had lower American Society of Anesthesiologists (ASA) classifications. The overall complication rate is 4.4% and in the hypothetical day care group this was 2.0%.
Five patients experienced transient hoarseness or vocal changes, one developed an anaphylactic reaction of unknown aetiology, and one patient experienced recurrence of a spontaneous tachycardia for which she required medical treatment. In the group not eligible for day care surgery, one patient required a re-operation due to a wound infection (0.5%) and one postoperative haematoma occurred (0.5%), which was managed conservatively. There were no complications in the ‘eligible day care group’ comprising patients safety in the hypothetical outpatient setting.
Since this retrospective analysis showed low complication rates, we concluded that hemithyroidectomy can be performed safely in a day care setting in our institution, and proceeded to implement this new strategy (part B). 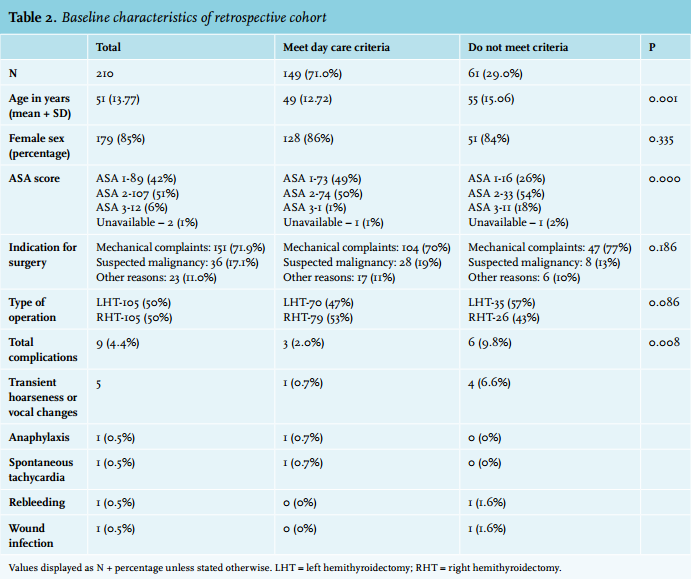
Prospective cohort
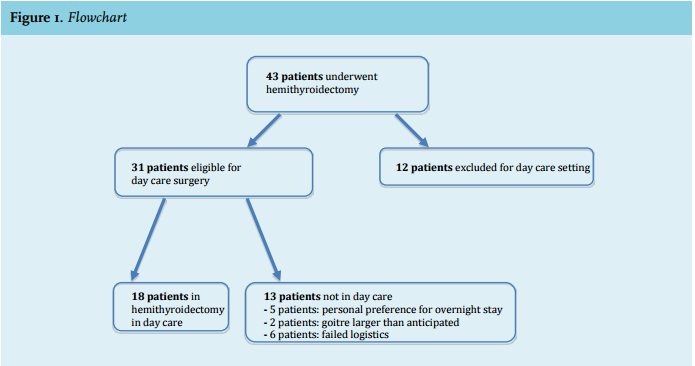
In 2015 a total of 43 patients underwent primary hemithyroidectomy and were included in the prospective cohort. A total of 31 (72%) patients met the international guidelines for day care thyroid surgery published by the American Thyroid Association, of which 58% (n = 18) were eventually treated by means of day care surgery. Twenty-five (58%) patients stayed overnight after surgery. A flowchart of patients undergoing hemithyroidectomy is illustrated in figure 1. Baseline characteristics and complication rates for the prospective cohort are summarised in table 3. The day care group was younger than the clinical group (median 50 and 61 years, respectively). Indication for surgery in the day care group was mechanical complaints in 89% and suspected malignancy in 11%; in the clinical group the indication was mechanical complaints in 56% and suspected malignancy in 32%.
Two minor complications (transient vocal changes, n = 2) occurred in the clinical group and there was one minor complication (transient vocal change) in the day care group. There were no emergency department visits or readmissions following surgery. No wound infections, haematomas or laryngeal nerve damage occurred.
Thirteen patients (30%) were eligible for day care surgery, but were not treated as such. Five patients (12%) chose to stay overnight, two patients had a retrosternal goitre which was larger than anticipated, and in the remaining six (14%) patients our logistics failed for example as these patients were scheduled for surgery late in the afternoon.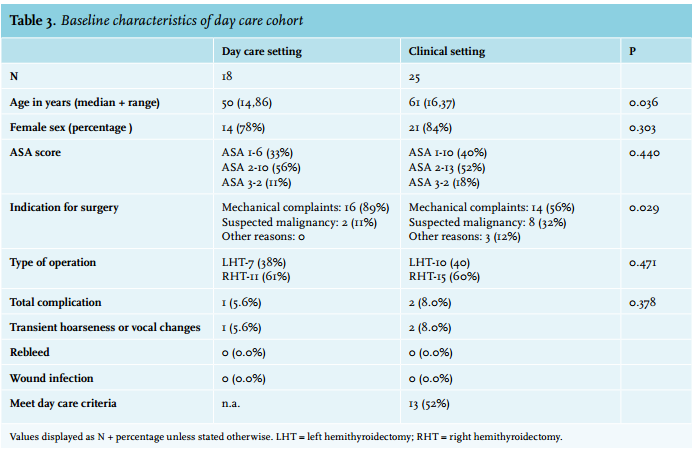
DISCUSSION
The retrospective analysis shows that day care surgery could be safely implemented in our institution. Thereafter, day care thyroid surgery was implemented and 58% of the eligible patients were treated as such. This is the first cohort in the Netherlands where thyroid surgery is performed in the day care setting. Patient safety is of paramount importance when installing a new regimen. Only one patient in the day care group experienced a complication, namely temporary hoarseness. No postoperative haematomas necessitating urgent interventions occurred. However, even though day care thyroid surgery was already reported in 1986,9 it remains a delicate topic as airway compromise due to haematoma formation is a feared complication. This complication did not occur in either our retrospective or our prospective cohort. We do have to acknowledge the fact that our low number of patients is prone to be biased with respect to complication rates. In the literature, Snyder et al.7 published the largest series of outpatient thyroidectomies, with over 1000 procedures in their cohort. Postoperative haematoma requiring reoperation was present in only one patient undergoing hemithyroidectomy.
A total of 31 patients met the international guidelines for day care thyroid surgery; however, only 18 were treated in day care surgery. In six patients our own logistics failed, so this is a major item to improve with this new strategy. Furthermore, it is important to interview patients to determine factors for which they chose to stay overnight, after which preoperative information can be adapted to address these factors.
Patients expressed their satisfaction when contacted by telephone the next day; however, no objective measurement of patient satisfaction was performed. Measurement and documentation of patient satisfaction is important to improve patient selection and improve preoperative information.
Despite the logistical hurdles and the low number of patients in this study, we advocate the introduction of day care thyroid surgery in the Netherlands.
However, although complications rates are supposedly very low, it is important to stay vigilant and carefully select patients suitable for day care surgery adhering to international guidelines.
CONCLUSION
Hemithyroidectomy performed in day care is feasible and safe with low complication rates provided that adequate patient selection is performed.
DISCLOSURES
The authors declare no conflict of interest. No funding or financial support was received.
REFERENCES