KEYWORDS
Aetiology, ascites, ascitic fluid analysis, diagnosis, liver cirrhosis 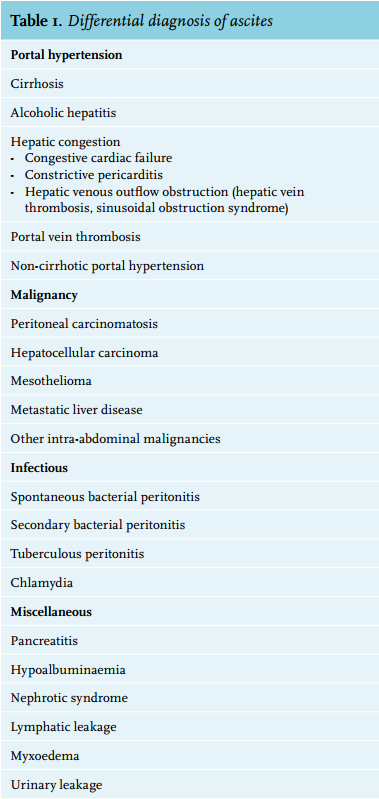
INTRODUCTION
Ascites is a pathological accumulation of fluid in the peritoneal cavity. It is a symptom of numerous medical conditions and has a broad differential diagnosis (table 1). Ascites can be classified by the underlying pathophysiological mechanism: portal hypertension, peritoneal disease, hypoalbuminaemia and miscellaneous disorders. Liver cirrhosis (75%) is the most common cause in adults in the Western world, followed by malignancy (10%), heart failure (3%), tuberculosis (2%), and pancreatitis (1%).1 An adequate diagnosis is necessary for successful treatment. Ascites can be classified as: mild ascites only detectable by ultrasound (grade 1), moderate ascites evident by moderate symmetrical distension of the abdomen (grade 2), and large or gross ascites with marked abdominal distension (grade 3).
Ascites is a common problem and patients present to a broad range of medical specialties. This review aims to provide a comprehensive overview of the current diagnostic approach to ascites and also discusses recent developments in ascites research.
DIAGNOSIS
History
Patients with ascites should be questioned about the pattern of body weight gain, change in abdominal girth, and ankle oedema. Information about the medical history, medication use, lifestyle, risk factors for liver disease, and infectious disease risk (e.g. migration) are relevant to discover the underlying aetiology.
Physical examination
A screening physical exam should be carried out in every patient, with awareness of signs of liver disease (erythema palmare, spider naevi, splenomegaly), heart failure (peripheral oedema, jugular venous distension, third heart sound, pulmonary rales) and malignancy (lymphadenopathy).2
The abdomen should be inspected for the presence of bulging flanks and percussion can reveal flank dullness. Flank dullness is found when approximately 1500 ml of ascites is present. These combined findings have a sensitivity of 75% and a specificity of 57%.3 Shifting dullness, determined by a 3 cm flank dullness shift when the patient changes from a supine to a lateral decubitus position has a sensitivity of 69% and a specificity of 69%.
Detection of a fluid wave or puddle sign is less reliable.3,4
Complications accompanying ascites such as umbilical, inguinal and other hernias and pleural fluid (hepatic hydrothorax) are particularly common in cirrhotic patients.
Blood tests
It is recommended to assess serum levels of creatinine, urea, electrolytes, prothrombin time and liver function tests and to order a complete blood cell count.5
Abdominal ultrasound
Abdominal ultrasound is the first-line imaging method to confirm the presence and quantity of ascites.5-7 Additionally, ultrasound can provide crucial information about the cause of ascites, detect signs of portal hypertension (splenomegaly and portosystemic collaterals), and offer guidance during paracentesis.
Abdominal paracentesis
Abdominal paracentesis is the most important step in the diagnostic work-up. It is indicated in every patient with new-onset ascites, patients with known ascites and clinical deterioration or a new presentation to an emergency department. Paracentesis is usually performed in the left lower quadrant, 3 cm cranially and 3 cm medially from the anterior superior iliac spine. Other sites include the right lower quadrant and the midline linea alba between the umbilicus and the pubic bone.7 Paracentesis should be performed under sterile conditions. Complications occur infrequently and include abdominal wall haematoma (1%), haemoperitoneum (< 0.1%), bowel perforation (< 0.1%), and infection (< 0.1%).7,8
Ascitic fluid analysis
Visual inspection
Visual inspection of the ascitic fluid can show a milky, cloudy, bloody, straw coloured or clear appearance (figure 1). Milky ascites suggests the presence of chylomicrons, containing predominantly triglycerides, and is therefore called chylous ascites. Chylous ascites can result from malignancy, trauma, liver cirrhosis, infection, pancreatitis, congenital disease and more uncommon causes.9 Cloudy ascites, also known as pseudochylous ascites, may indicate peritonitis, pancreatitis or a perforated bowel. Bloody ascites is often associated with malignancies or results from traumatic paracentesis, whereas straw coloured or clear ascites is common in liver cirrhosis.10 The first impression of the appearance of ascites is non-specific, but can steer the direction of diagnosis.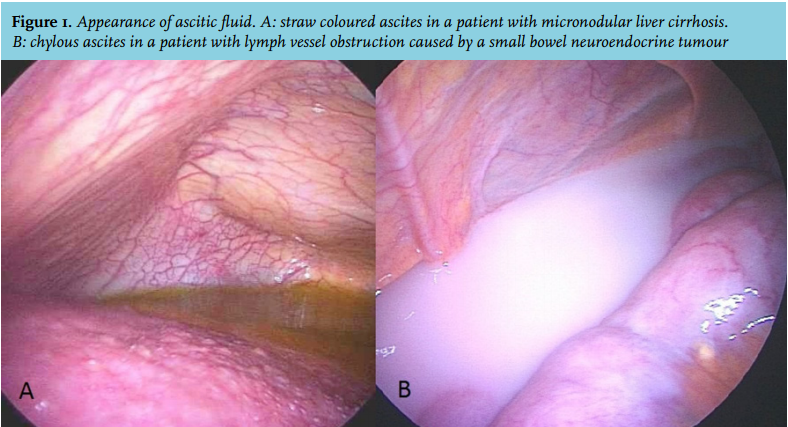
Biochemical testing
Serum-ascites albumin gradient
The serum-ascites albumin gradient (SAAG) is the most sensitive marker to distinguish between ascites due to portal hypertension/hepatic congestion and other causes, with an accuracy of 97%.11 The SAAG is obtained by subtracting the level of albumin in the ascitic fluid from that in the serum, both measured at the same time. A value ≥ 1.1 g/dl (or 11 g/l) indicates underlying portal hypertension or hepatic congestion; a value < 1.1 g/dl indicates aetiologies not due to portal hypertension, such as malignancy, pancreatitis or infection.6,11
Total protein
Current international guidelines still recommend measuring the total protein concentration in ascites.5-7 Traditionally, this was thought to indicate the aetiology of ascites according to the transudate-exudate concept, but this approach is now generally considered inferior. The total protein concentration does have prognostic value as concentrations lower than 15 g/l are associated with an increased risk for spontaneous bacterial peritonitis (SBP) in cirrhotic patients.
Amylase
The amylase concentration in ascitic fluid should be measured in particular when pancreatic disease is considered. Pancreatic ascites can be caused by leakage from pancreatic pseudocysts or due to pancreatic duct rupture. An amylase ascitic fluid/blood serum concentration ratio of 6.0 is indicative for pancreatic disease, considering that a ratio of 0.4 is normal in non-pancreatic ascites.12 However, high levels of amylase have also been detected in patients with malignancy and other conditions making it a rather non-specific finding. Still it can be of significant value in patients with comorbidities such as alcoholic cirrhosis and pancreatitis.13
Triglycerides
A concentration of triglycerides in the ascitic fluid that exceeds the blood serum level (2.2 mmol/l) indicates chylous ascites. Previous abdominal surgery, pancreatitis, trauma and retro-peritoneal lymphoma are among the main causes.9 Malignancy is diagnosed in 80% of patients with chylous ascites; however, it must be noted that ascites in up to 6% of cirrhotic patients has a chylous character.14
Adenosine deaminase activity
The activity of adenosine deaminase (ADA), an enzyme of purine metabolism, is a reliable marker to differentiate tuberculous ascites from other aetiologies. An ADA cut-off value between 36 to 40 IU/l has a high sensitivity (100%) and specificity (97%) for diagnosing abdominal tuberculosis.15 In the Netherlands, the ADA activity assay is available in a limited number of centres.
Glucose and lactate dehydrogenase
Traditionally, determining glucose and lactate dehydrogenase concentrations in ascites constituted part of the diagnostic work-up. A lower glucose concentration in ascitic fluid than in blood serum can indicate the presence of bacteria, white blood cells or cancer cells.16,17 A low level of lactate dehydrogenase is associated with non-malignant ascites, high levels suggest a malignant aetiology.18 Unfortunately both measurements are influenced by the SAAG, are non-specific and are no longer recommended.19
Urea and creatinine
A very uncommon cause of ascites is urinary leakage into the peritoneal cavity. Urinary ascites is associated with pathological bladder changes and outlet obstruction.20,21 Normally the ascites/plasma creatinine ratio is approximately one, whereas a ratio of five is reported in case of urinary ascites. Importantly, urinary ascites can be accompanied by pseudo-renal failure due to peritoneal absorption of urea.20
Non-biochemical testing
Polymorphonuclear leukocyte count
A polymorphonuclear neutrophil (PMN) count should be performed in the ascitic fluid of all patients with ascites admitted to the hospital or showing clinical signs suggestive of SBP. A PMN count ≥ 250 cells/mm3 (0.25 x 109 cells/l) confirms the diagnosis of SBP in the absence of an evident intra-abdominal source of infection.22 A PMN count repeated after 48 hours of antibiotic administration can distinguish between SBP and secondary bacterial peritonitis, a decrease suggests SBP and a sustained increase secondary bacterial peritonitis. A repeated PMN count 48 hours after starting antibiotic therapy is recommended to document the efficacy of antibiotic therapy for SBP.7,16 Although SBP is mainly a complication of ascites due to portal hypertension, it may also develop in patients with ascites of other aetiologies.
Bacterial cultures
Ascitic fluid should be cultured if SBP is clinically suspected. Bedside inoculation of 10 ml under sterile conditions using blood culture bottles, containing aerobic and anaerobic media, leads to identification of an organism in ~80% of patients with SBP.7,23,24 Ascitic fluid cultures should be carried out before antibiotic treatment is initiated.
PCR bacterial DNA Mycobacterium tuberculosis
Bacterial DNA of Mycobacterium tuberculosis in ascitic fluid can be detected using polymerase chain reaction (PCR) and can be performed when tuberculous ascites is suspected. This method has a high sensitivity (94%) compared with microscopic acid-fast bacilli smears (~0%) and mycobacterial culture (~50%).25,26 Alongside a higher diagnostic accuracy, PCR offers a timesaving method in contrast to current Mycobacterium culture techniques. PCR is a widely available biomolecular technique, however, PCR specific for the genus of Mycobacterium may not be available in all centres. Furthermore, culturing Mycobacterium from ascitic fluid or peritoneal biopsy remains the gold standard test according to national and international guidelines, also allowing antibiotic susceptibility testing.7
Cytology
Ascitic fluid cytology should be performed in case of suspicion of malignant ascites or when the underlying aetiology is in doubt (e.g. no decrease in PMN count after 48 hours of antibiotic treatment). Clearly, positive cytology is highly indicative for peritoneal carcinomatosis. The sensitivity of cytology is 83%, but can be as high as 97% if three samples from separate paracenteses are analysed.27 Crucial factors are avoiding any time delay between obtaining the ascitic fluid and cytology processing as well as obtaining at least 50 ml ascitic fluid, or even 1000 ml if the first test was negative.27 The sensitivity of cytology in patients with hepatocellular carcinoma and ascites is low (~27%).28
Diagnostic laparoscopy
If the conventional work-up fails to disclose the cause of ascites, laparoscopy should be considered. Laparoscopy offers the advantages of visual inspection of the peritoneal cavity in combination with the ability to obtain targeted biopsies for histological and microbiological studies. The procedure may be particularly helpful to diagnose peritoneal carcinomatosis, tuberculous peritonitis and other peritoneal or omental diseases such as mesothelioma and sclerosing peritonitis.29,30
Figure 2 shows schematically the diagnostic approach to the patient with ascites.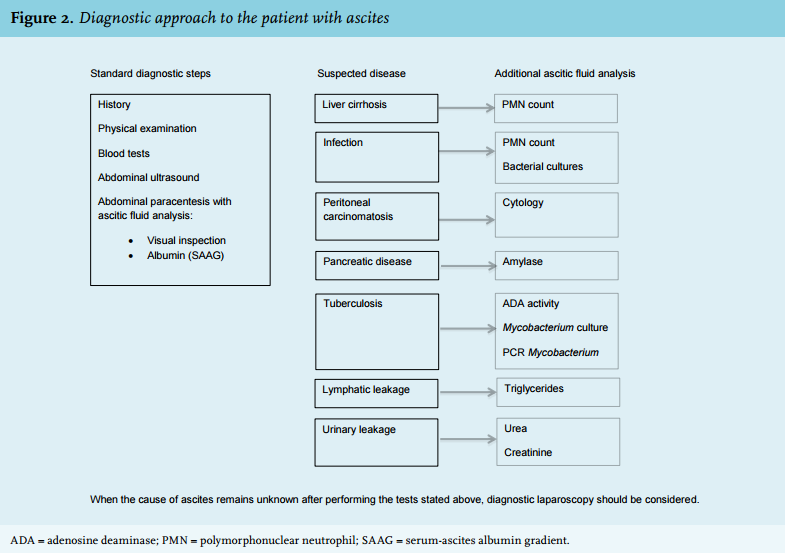
DIAGNOSTIC DEVELOPMENTS
Novel markers in ascitic fluid analysis have been proposed for the initial differential diagnosis as well as for predicting prognosis in specific diseases. Most discoveries either target on simplifying, accelerating or reducing the costs of the diagnostic process or they result from advancing biochemical laboratory techniques.
Leucocyte esterase reagent strips
Leukocyte esterase reagent strips are widely used for urinary analysis with the advantages of a simple, inexpensive and rapid bedside test. Several studies have examined the usefulness of this method for diagnosing SBP and found this test had a sensitivity and specificity ranging from 80-93% and 93-98%, respectively.31 The negative predictive value is remarkably high ranging from 97-99%, which makes it an ideal tool to rule out SBP.31 Together with the other advantages, the reagent strip could gain a place in routine practice. Recently, an asciticspecific reagent strip with a cut-off value of 250 cells/mm3 was introduced, which could further improve diagnostic accuracy.32
Viscosity
A few studies have reported the potential usefulness of viscosity measurement of ascitic fluid. Measuring viscosity was found to be able to discriminate between portal hypertension and non-portal hypertension related aetiology and showed a high correlation with the SAAG.33 These preliminary results await confirmation by additional studies.
Vascular endothelial growth factor
Vascular endothelial growth factor (VEGF) is a protein which is fundamental in the process of vasculogenesis and angiogenesis. High concentrations of vascular endothelial growth have been associated with malignant ascites.34 Additional research is necessary to define the diagnostic value of this test.
Bacterial DNA, cytokines and other proteins
Bacterial DNA was studied in two series of 30 patients with ascites due to liver cirrhosis. The presence of bacterial DNA in ascites was regularly found documenting bacterial translocation, which could indicate a worse clinical prognosis in this patient group, without implicating a diagnosis of SBP. Markers, such as endotoxin and peptidoglycan/β-glucan, could predict a poor clinical outcome.35,36 Another study, including 52 patients with SBP and 27 control patients with cirrhotic ascites, found that blood serum concentrations of procalcitonin and an ascitic fluid concentration of calprotectin were significantly higher in SBP patients. Both serum and ascitic levels of TNF-α and IL-6 were significantly higher in SBP patients than in non-SBP patients.37 These findings need to be confirmed in larger series of patients.
Platelet indices
Increased platelet indices, e.g. mean platelet volume and platelet distribution width, have been reported in the blood of cirrhotic patients with SBP. The diagnostic accuracy was not sufficient in this study, however, these indices can be considered as a potential diagnostic tool.38
Tumour markers
Several studies have addressed the diagnostic value of tumour markers in ascitic fluid including α-fetoprotein, des-gamma-carboxy prothrombin, carcinoembryonic antigen, cancer antigen 19-9 and cancer antigen 125. Increased concentrations have been associated with underlying malignancies but are also found in medical conditions such as gastritis, diverticulitis, cirrhosis and pancreatitis.33
CONCLUSION
The differential diagnosis of ascites is broad and includes a large number of benign and malignant causes. A structured diagnostic approach will likely reveal the aetiology in the large majority of cases and is based on the following elements: history, physical examination, blood tests, abdominal ultrasound and diagnostic paracentesis. Standard ascitic fluid analysis includes visual inspection and determination of the SAAG. In patients with suspected infection or underlying liver disease a PMN count and bacterial cultures are standard. According to clinical circumstances other established diagnostic studies are ascites cytology and determination of levels of amylase and triglycerides. In exceptional cases measuring urea and creatinine levels may be crucial. ADA activity measurements, Mycobacterium cultures and PCR for Mycobacterium DNA are indicated when tuberculosis is considered. Leucocyte esterase reagent strips are useful, in particular to rule out SBP in patients with a low a priori risk. New diagnostic markers such as viscosity, VEGF, bacterial DNA, cytokines and platelet indices have been proposed, but further research is needed to validate the value of these markers.
DISCLOSURES
All authors declare no conflicts of interest. The authors did not receive grant support to conduct this study. The study was sponsored by the Foundation for Liver and Gastrointestinal Research Rotterdam (SLO).
REFERENCES