KEYWORDS
Ascites, leukocyte count, liver cirrhosis, peritonitis, reagent strips
INTRODUCTION
Spontaneous bacterial peritonitis (SBP) is a life-threatening complication in cirrhotic patients with ascites.1 Late or misdiagnosed SBP can lead to increased mortality due to consequences such as gastrointestinal bleeding, development of hepatorenal syndrome and progressive liver failure. Therefore, the threshold for performing diagnostic paracentesis and ascitic analysis should be low.2
The reported prevalence of SBP in cirrhotic patients differs from 0-2.8% in outpatients to 10-30% in hospitalised patients.3-9
The gold standard test to diagnose SBP is a polymorphonuclear neutrophil count of ≥ 250/µl in ascites using a manual counting chamber, regardless of the outcome of the culture of ascitic fluid.2 This analysis is laborious, time-consuming and expensive. Automated cell counting has been proposed to be a reasonable alternative with a high diagnostic accuracy.10
In the past two decades several studies have examined the use of leukocyte esterase reagent strips for the bedside diagnosis of SBP.8,11-25 These strips are widely used for rapid urinary analysis and the principle is based on the detection of leukocyte esterase activity of granulocytes.
Varying levels of diagnostic accuracy to diagnose SBP with reagent strips have been reported, with a sensitivity ranging from 45-100%, a specificity from 90-100%, a positive predictive value from 42-100% and a negative predictive value from 93-100%.8,9,11-31 These inconsistent results could be related to variability in reagent strips, patient populations, different cut-off values and the subjective interpretation of the reagent strip result. However, the consistent high negative predictive value could make the reagent strips a very useful rule-out tool.
This study was performed to 1) assess the diagnostic accuracy of reagent strips in comparison with the current gold standard test for diagnosing SBP in a mixed population of low-risk and high-risk patients, and 2) investigate the possible advantage of automated analysis of the reagent strips over visual non-automated reading.
MATERIALS AND METHODS
Study design
This prospective cohort study was carried out at the Department of Gastroenterology and Hepatology in a referral centre for liver disease in the Netherlands. The study was designed and carried out in accordance with the principles of the Helsinki Declaration and approval was given by the local medical ethics committee of the hospital.
Patients
Consecutive patients with cirrhosis undergoing diagnostic or therapeutic paracentesis were prospectively enrolled from July 2006 up to and including July 2007. The total study population was subdivided into a low-risk and high-risk population for the development of SBP. The low-risk population was defined as patients undergoing therapeutic, large volume paracentesis or outpatients undergoing diagnostic paracentesis.4,5,9 The high-risk population was defined as hospitalised patients undergoing a standard diagnostic paracentesis at admission or because of clinical deterioration.2 Patients with ascites secondary to causes other than liver disease were excluded.
Methods
Paracentesis was performed under strict sterile conditions. Ascitic fluid was routinely analysed in the central clinical laboratory with automated determination of the white blood cell count with differential. Ten millilitres of fluid was inoculated at the bedside in aerobic and anaerobic blood culture bottles (Bactec®). Fluid was collected in a sterile tube and assessed by two leukocyte esterase reagent strips (Combur10 strips, Roche Diagnostics). Both strips were read out after 60 seconds, one strip visually and one with a photospectrometer (Urisys 1100®, Roche Diagnostics). The observer was unaware of the results of the spectrometer. The observer could differentiate between four different colour shades corresponding to 0, 25, 100 or 500 leukocytes/µl.
Statistical analysis
Data analysis was performed using IBM SPSS Statistics for Windows, Version 21.0 (Armonk, NY: IBM Corp.).
A mean and standard deviation was computed for continuous variables and compared with the Student’s t-tests if normally distributed. A two-sided p-value < 0.05 was considered significant. Sensitivity, specificity, positive and negative predictive values with confidence intervals of 95% were calculated. Receiver operating characteristic (ROC) curves were computed and the optimal categorical cut-off point was analysed. Diagnostic performance between photospectrometer reading and visual interpretation was statistically compared using a McNemar test.32
RESULTS
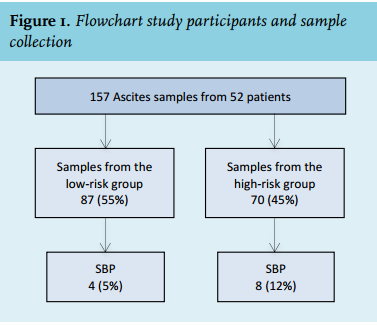
A total of 157 ascitic fluid samples were collected from 52 patients (range 1-14 samples per patient); 87 samples (55%) were obtained in the low-risk population and 70 (45%) in the high-risk population (table 1). The prevalence of SBP according to analysis of the polymorphonuclear neutrophil count was 4 (4.5%) in the low-risk group and 8 (11.6%) in the high-risk group (figure 1).
In the low-risk population, one culture (25%) was positive, identifying an Enterococcus faecium, whereas three cultures (37.5%) were positive in the high-risk population, identifying Enterococcus coli, Haemophilus parainfluenzae and Pseudomonas aeruginosa in one case each. 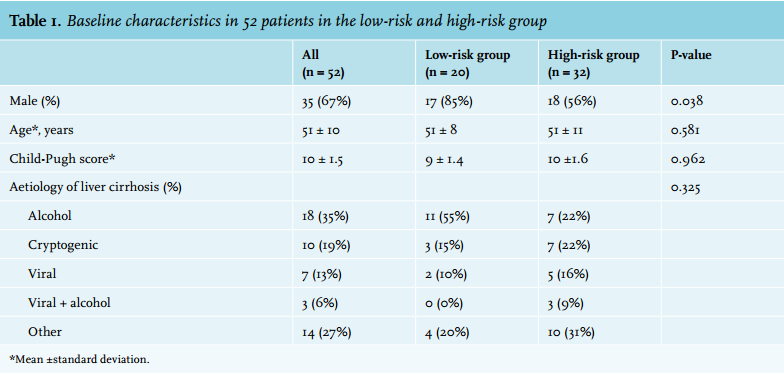
Photospectrometer versus visual reading
Of the total of 12 (25%) cases of SBP, three were not detected by optical reading of the strip but correctly diagnosed with the photospectrometer.
With visual reading, the sensitivity for diagnosing SBP was 75% (95% CI 43-93), the specificity 99% (95% CI 95-100), the positive predictive value 82% (95% CI 48-97) and the negative predictive value 98% (95% CI 94-100). The diagnostic accuracy for automated reading was slightly superior (p = 0.007 McNemar test): sensitivity 100% (95% CI 70-100), specificity 93% (95% CI 87-97), positive predictive value 55% (95% CI 33-75) and negative predictive value 100% (95% CI 97-100) (table 2). ROC curve analysis indicated that the diagnostic accuracy of the strips was optimal at a cut-off of 100 leukocytes/µl. 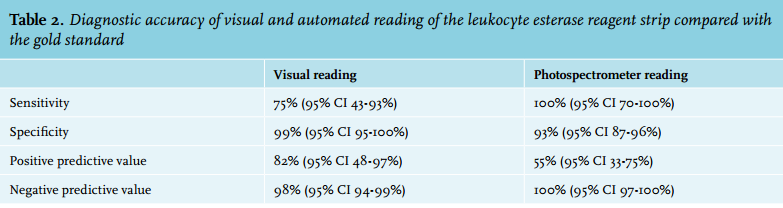
Low- and high-risk group analysis
The diagnostic performance of the strip with automated reading in the low- and high-risk populations was similar: the negative predictive value was 100% (95% CI 92 -100%) and the specificity was 93% (95% CI 83 -98%).
DISCUSSION
The results of the present study support the diagnosing value of leukocyte esterase reagent strips in ascitic fluid analysis in patients with cirrhosis. In particular, this simple, quick and inexpensive method could reliably rule out SBP, with a 100% negative predictive value in populations at low- and high-risk for SBP. Automated reading of the reagent strip was superior to visual interpreting and prevented false-negative results.
The diagnostic accuracy of the Combur10 strip in ascitic fluid analysis has been studied previously by several groups.13,18,26-28,30 The results of these studies were comparable with our results in terms of a high negative predictive value of reagent strip testing. The cumulative data suggest that the sensitivity of strips for diagnosing SBP is variable and may not be optimal. A negative test result, however, strongly predicts absence of SBP. Thus, in patients undergoing diagnostic paracentesis, a negative reagent strip result may imply that further diagnostic studies – polymorphonuclear neutrophil count and bacterial cultures – are not useful and can be omitted. Obviously, preventing unnecessary diagnostic studies in a substantial proportion of patients presenting with ascites may lead to a marked reduction in costs.
Although an automated reader has been used in previous studies,7,15 this study is, to our knowledge, the first to compare visual and automated reading of reagent strips in ascitic fluid analysis. Our results suggest that automated reading is superior and may be the preferred method in clinical practice. Additional studies would be useful to confirm this finding.
One of the limitations of our study may be that the reagent strips we used are not specifically designed for ascitic fluid analysis. The cut-off levels are not based on the polymorphonuclear neutrophil count of 250 leukocytes/ µl, the gold standard for SBP. It has been suggested that protein could interfere with the test and has a negative effect on the accuracy. One study found a significantly higher mean ascitic protein content in patients with false-negative results than in patients with true-positive results.29 Furthermore, little is known regarding the effects of the different composition of ascites as compared with urine, for example with respect to bilirubin or pH level, on reagent strip diagnostic accuracy. Remarkable results – a 100% sensitivity and negative predictive value – have been reported with the Periscreen strip, a strip with specific characteristics for ascitic fluid analysis.31 These results await confirmation in a large cohort, which is currently being investigated in the Per-DRISLA study.33In conclusion, this study adds to already available data suggesting that Combur reagent strips are useful for ascitic fluid analysis in cirrhotic patients. Cumulative evidence clearly indicates that a negative test result reliably rules out SBP. We found reagent strips an inexpensive, timeand money-saving tool, which is available both during and after regular working hours. Reading the strips with a photospectrometer may be superior to visual reading. 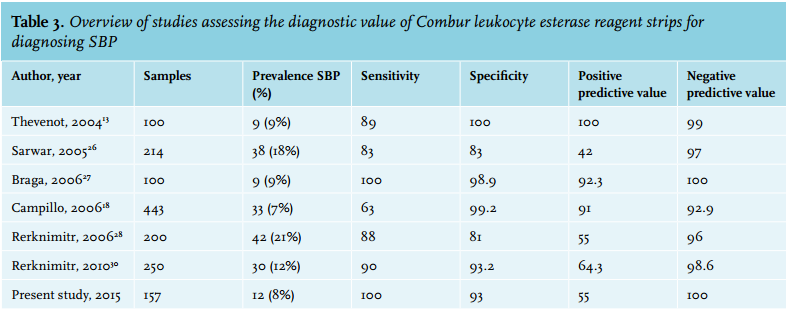
ACKNOWLEDGEMENTS
We thank Roche Diagnostics (Almere, the Netherlands) for providing the Urisys 1100 analyser.
Funding
Sponsor of the study was the Foundation for Liver and Gastrointestinal Research Rotterdam (SLO).
Disclosures
The authors did not receive a grant support to conduct this study. The authors declare no conflict of interest.
REFERENCES