DIAGNOSIS
Computed tomography (CT) was performed, demonstrating extensive pneumomediastinum extending into the lower neck and bilateral supraclavicular and subscapular regions (figure 2A and B), followed by contrast oesophagram, which was negative for perforation (figure 2C). The patient was diagnosed with diabetic ketoacidosis complicated by spontaneous pneumomediastinum and admitted to the intensive care unit for aggressive intravenous fluid resuscitation and glucose control. He recovered uneventfully following medical therapy and was discharged home four days later.
Spontaneous pneumomediastinum complicating diabetic ketoacidosis is a rare, but well-described entity first described by McNicholl in 1968.1 Although the precise pathophysiology remains elusive, some have postulated that it relates to the abnormal pattern of ketotic hyperventilation (Kussmaul respiration), which induces transalveolar pressure swings sufficient to cause alveolar rupture into the lung interstitium. This results in the dissection of air along the peribronchial and perivascular planes with extravasation into the mediastinum.2
Substernal chest pain with radiation to the back, dyspnoea and subcutaneous emphysema are the classic indicators of spontaneous pneumomediastinum, although it is not uncommon for patients in diabetic ketoacidosis to be ‘asymptomatic’ due to their symptoms being attributed to metabolic acidosis. The differential diagnosis in these patients includes spontaneous oesophageal perforation (Boerhaave’s syndrome), pneumothorax, pneumonia, pulmonary embolism, and cardiovascular events such as ischaemia, arrhythmia, pericarditis, or aortic dissection.3 Therefore, initial evaluation of spontaneous pneumomediastinum should always include chest X-ray and ECG. Given the gravity of a missed or delayed diagnosis of oesophageal perforation, any patient with spontaneous pneumomediastinum and a history of chest pain, vomiting, fever, leucocytosis, haemodynamic instability or pleural effusion on chest X-ray should undergo immediate oesophagram or CT of the neck and chest with a water soluble oral contrast.4
Negative imaging warrants a 24-hour period of observation, analgesia, oxygen therapy, and bed rest. A clear liquid diet can be initiated once the patient is able tolerate oral intake, and advanced accordingly.2 Antibiotics and repeat swallow studies are not necessary, although daily chest X-ray can be followed for 1-2 days to ensure that there is no radiographic progression.3-4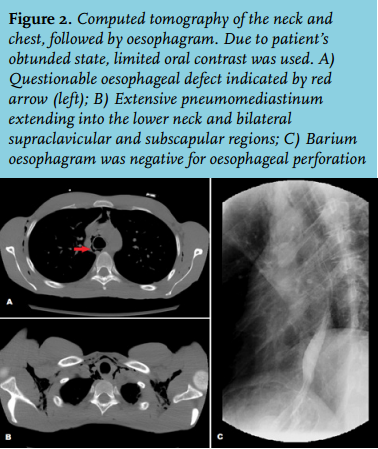
DISCLOSURES
The authors have no conflicts of interest to declare. No financial sponsorship was accepted in producing this manuscript and there are no material contributions or third-party sources of funding to acknowledge.
REFERENCES