DIAGNOSIS
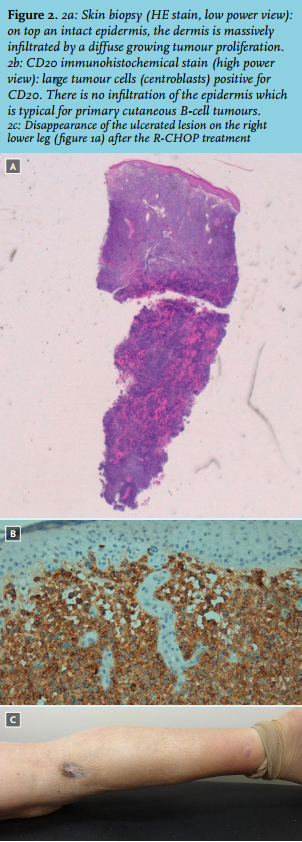
Histopathological examination showed a diffuse proliferation of polymorphic centroblasts infiltrating the whole dermis. There was no infiltration of the epidermis, and no angiocentric or intravascular growth pattern. On immunohistochemistry, the cells were positive for CD20, CD79a, CD5, MUM-1, BCL2 and BCL6 and negative for CD3 and CD10. The diagnosis of primary cutaneous diffuse large-B-cell lymphoma, leg type (PCDLBCL-LT), T1bN1M0,1 was clinically, histologically, and immunohistochemistry confirmed (figure 2a and 2b). Additional bone marrow aspiration and biopsy were normal. This patient was in a good physical condition (Karnofsky score 90%), therefore full-dose rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone were given, once every 21 days for six cycles (R-CHOP21). No complications were observed. The skin lesions on both legs of our patient disappeared rapidly after initiation of the R-CHOP treatment (figure 2c). After one year of follow-up the patient is in complete remission and no recurrence of the skin lesions has appeared.
PCDLBCL-LT is one of the three main types of primary cutaneous B-cell lymphomas (PCBCL). PCBCLs are lymphomas with a B-cell phenotype that present in the skin without any evidence of systemic of extracutaneous disease at first appearance. In a study of 1905 patients with primary cutaneous lymphoma, PCDLBCL-LT corresponds to 4.5% of all cutaneous lymphomas. PCDLBCL-LT accounted for 20% of all PCBCLs.2
As the name suggests, PCDLBCL-LT mainly involves the lower legs of predominantly older women (female:male ratio is 2-4:1) with a median age of 70-75 years. The rest of the body is involved in 10-20% of the cases. Patients characteristically present with one or multiple rapidly growing bluish-reddish nodules or tumours on one or both legs. Some of these nodules/tumours can be ulcerated. By definition, these lymphomas are limited to the skin at initial presentation; however, they can spread to extracutaneous sites too.3 These sites can include the lymph nodes, bone marrow, and the central nervous system. Several studies report a five-year survival rate of 20-60% with a median of 50%. Presence of multiple skin lesions at first presentation is a negative prognostic factor. A recent retrospective multicentre study in France reported an improvement in the survival of PCDLBCL-LT with three-year survival of 74% and five-year survival of 66%. These rates were 80% and 74% respectively in those patients who received immunochemotherapy with rituximab.4
PCBCLs with predominantly large cells are either PCDLBCL-LT or primary cutaneous follicle centre lymphomas (PCFCL). It is important to distinguish these two types of B-cell cutaneous lymphomas since epidemiology, histopathology, treatment, and prognosis are completely different. Histologically PCDLBCL-LT consists mainly of centroblast, large B-cells and immunoblasts while the follicle centre lymphoma consists mainly centrocyte cells. In PCDLBCL-LT, BCL-2 FOXP1, IgM and MUM-1 are specifically positive whereas they are negative in the primary cutaneous follicle centre lymphomas. In PCFCL there are networks of follicular dendritic cells; these are lacking in PCDLBCL-LT.3,5
It is important to recognise and systemically treat PCDLBCL-LT since in general these types of diffuse large-B-cell lymphoma will have an aggressive biological behaviour in contrast to the PCFCL. Guidelines recommend to treat PCDLBCL-LT with systemic immunochemotherapy, consisting of six cycles of R-CHOP with or without radiation therapy.3-5 As there are no randomised controlled trials available in the literature, treatment recommendations for PCDLBCL-LT are mainly based on retrospective and anecdotal studies and on institutional experience.
REFERENCES