KEYWORDS
Complex regional pain syndrome, pamidronate, steroid, stroke
INTRODUCTION
Complex regional pain syndrome (CRPS) is a neuropathic pain syndrome related to vasomotor and sudomotor nerve dysfunction. Some stroke patients subsequently develop dysesthesia, severe pain, hyperalgesia, temperature asymmetry, skin colour asymmetry, oedema, diaphoresis, decreased range of motion and trophic changes in their upper extremities. Although the pathophysiology of these findings, referred to as CRPS 1, is unclear, the incidence is significant.1,2 The incidence of CRPS type I after brain lesion is as high as 1.5-61%.3-6 Early therapeutic intervention is recommended for a better outcome since dystrophic changes in the skin, pain, and joint contractures in the affected limb might induce functional dysfunction and lengthen the hospital stay for rehabilitation.7
There are various invasive and non-invasive treatment options for CRPS, such as systemic and topical analgesics and steroids, neuropathic agents, physiotherapy and sympathetic nerve blocks.8,9 A systemic steroid therapy for a short period of time is effective and commonly used.10,11
However, clinicians frequently face difficulties in using steroids for CRPS patients with stroke, who often have comorbidities such as diabetes mellitus, hypertension and osteoporosis. Therefore, a safer and more effective therapeutic method is imperative for these patients.
Recently, a possible role for bisphosphonate in the treatment of CRPS was proposed.12-14 Bisphosphonate has an effect on pain control in bone-related diseases such as Paget’s disease, metastatic bone disease, myeloma and spinal fracture,15-17 and might therefore have a therapeutic effect on pain in CRPS where hyperactivity of osteoclasts is one of the conceivable pathogeneses.14 In addition, bisphosphonate is a strong inhibitor of bone resorption and might prevent osteoporosis that is induced by hyperactive osteoclast and immobilisation in CRPS.18 However, there is limited evidence for the therapeutic effect of bisphosphonate in CRPS type I after stroke. Therefore, the aim of the current study was to determine the therapeutic effect of pamidronate, a second-generation bisphosphonate, in the treatment of CRPS type I patients after stroke and to compare its effect with conventional steroid therapy.
MATERIALS AND METHODS
Subjects
This study was conducted in the rehabilitation ward of a university hospital from October 2010 to March 2012. Among 65 stroke patients, 39 patients who did not meet inclusion criteria were excluded and five patients declined to participate in the current study. Finally, 21 first-ever stroke patients with CRPS type I within six months of stroke onset were included in the present study. All patients were admitted to our rehabilitation centre for comprehensive rehabilitation therapy for stroke.
The diagnosis of CRPS type I was based on the ‘Budapest’ criteria.19 Clinical diagnosis for CRPS was confirmed when the patient had continuing pain which was disproportionate to any inciting event and the patient had at least one sign in two or more of the categories: sensory, vasomotor, sudomotor/oedema, and motor/trophic, and at least one symptom in three or more of these categories. Once diagnosed, patients underwent three-phase bone scintigraphy and musculoskeletal ultrasonography for differential diagnosis. The musculoskeletal ultrasonography was performed by one physiatrist. All images of three-phase bone scintigraphy were interpreted by one nuclear radiologist. Patients were classified as CRPS positive when the images of blood flow, blood pool and delayed phases showed diffuse asymmetric uptake.
Exclusion criteria were as follows: 1) disease or trauma history other than stroke that might cause CRPS in the upper extremities; 2) past history of shoulder pain or limitation of motion on the hemiplegic side; 3) history of diabetes mellitus, hyperthyroidism, renal and liver dysfunction or peripheral neuropathy; 4) a score of less than 23 on the Korean version of Mini-Mental State Examination (K-MMSE); 5) history of treatment for CRPS; and 6) medical treatment with bisphosphonate for osteoporosis or with other drugs that may have an effect on bone metabolism within six months.
Written informed consent was obtained from each participant in the study, and approval for the study was obtained from the institutional review board. The study was performed in accordance with the amended Declaration of Helsinki and was approved by the appropriate local ethics and drug committees.
Protocol
All 21 patients completed informed consent and medical history forms, and were randomly assigned to either the intravenous bisphosphonate group or the oral steroid group. Patients underwent three-phase bone scintigraphy and a physical examination by one physiatrist who was blind to the study information. Throughout the study period, patients were encouraged to participate in their inpatient rehabilitation program.
Measurements of subjective pain and quantitative evaluation of hand oedema were performed at baseline and at one, two and four weeks after the end of each treatment. Subjective pain was measured using a visual analogue scale (VAS) that consisted of a horizontal line, 100 mm long, anchored at the left by the descriptor ‘no pain’ and at the right by the descriptor ‘unbearable pain’.
Quantitative evaluation of hand oedema was performed by measuring the circumference of the middle (third) finger (CMF) and the wrist (CW) on the affected side.20 We used this method because it is easy to perform and cost-effective. Before initiation of the current study, an intra- and inter-rater reliability test of this method (CMF and CW measurement) with healthy 25 subjects was performed. The interclass correlations for intra-rater and for inter-rater reliability were higher than 0.9. CMF was measured using a finger circumference gauge at the midpoint between the proximal finger crease and the middle finger crease and CW was measured using Roylan’s flexible tape at the level of radial styloid process. Each circumference was measured in triplicate, and the median value was used as an estimate of hand oedema. Measurements of hand oedema were always conducted at 10.00 hours to avoid the influence of circadian variations.
Intervention
The steroid group received oral steroid therapy, prednisolone (Solondo®; Yuhanmedica Co., Cheongwon, Korea), at an initial dose of 1 mg per kg of body weight. The dose was tapered over two weeks. Therefore, the total duration of the steroid therapy was two weeks. The bisphosphonate group received pamidronate (Panorin®; Hanlim Pharm. Co., Seoul, Korea) infusion intravenously. Each infusion with 60 mg of pamidronate mixed with 500 ml of normal saline was delivered to the unaffected upper extremity and lasted for more than four hours. The total dose of pamidronate was 180 mg, delivered via three infusions every other day. Therefore, the total duration of the pamidronate therapy was six days. Measurements of study parameters were performed at baseline and at one, two and four weeks after the end of each treatment.
Statistics
Statistical analysis was performed with IBM SPSS version 20.0 software for Windows (SPSS Inc., Chicago, IL, USA). The chi square and Mann-Whitney tests were used to compare the baseline characteristics of the two groups. In cases where the anticipated frequency was lower than 5, a Fisher exact test was applied. Repeated measures analysis of variance (ANOVA) was used for the comparison of all parameters of pain and hand swelling according to the time period and type of therapy until four weeks of follow-up. The interactions between clinical response and time were examined to determine if changes differed in the bisphosphonate and steroid groups. All data are presented as mean ± standard deviation; p < 0.05 was considered statistically significant.
RESULTS
General characteristics of patients
Of the 21 recruited patients, 10 were randomised to the steroid group and 11 to the bisphosphonate group. The mean age of participants was 65.19±9.07 years (range 44-77 years), with 11 males and 10 females. Onset duration since stroke occurrence was 51.57±26.60 days. There was no significant difference between the two groups in terms of age, sex, side of the affected hand, type of stroke, K-MMSE scores or onset duration since stroke occurrence (table 1). In addition, baseline subjective pain VAS, CMF and CW were not significantly different between the two groups. All patients in both groups completed the four-week study period after the end of each treatment (table 1).
Change in clinical parameters after treatment
Subjective pain
Both groups showed significant improvement in subjective pain VAS scores at 1-week follow-up and this effect was maintained until 4-week follow-up (table 2). Time-by-group interactions for VAS score were found until 2-week follow-up. However, this was not significant at 4-week follow-up (table 2).
Circumference of the middle finger
CMF of the affected hand was significantly reduced at 1-week follow-up in both groups, and this effect was maintained until 4-week follow-up in the steroid group, however only until 2-week follow-up in the pamidronate group (table 3). Time-by-group interactions for CMF change were non-significant (table 3).
Circumference of the wrist
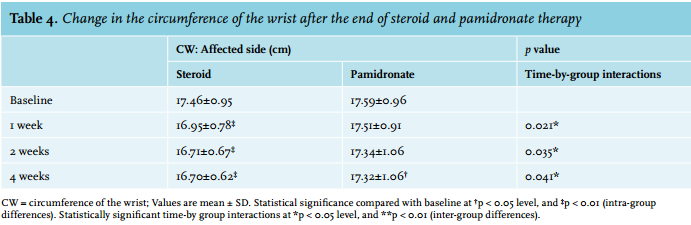
CW of the affected side was significantly reduced at 1-week follow-up in the steroid group, and this effect was maintained until 4-week follow-up. In the pamidronate group, a significant change of CW was observed at 4-week follow-up (table 4). Time-by-group interactions for CW change were significant during the whole period of follow-up (table 4).
Adverse effects
In the intravenous bisphosphonate group, two patients (18.2%) had a fever higher than 38.0°C, which resolved within 6-24 hours after administration of acetaminophen. One patient (9.1%) reported general myalgia and another patient (9.1%) presented with a minor infusion site reaction, which improved without any intervention. In the steroid group, no steroid-induced side effects were observed.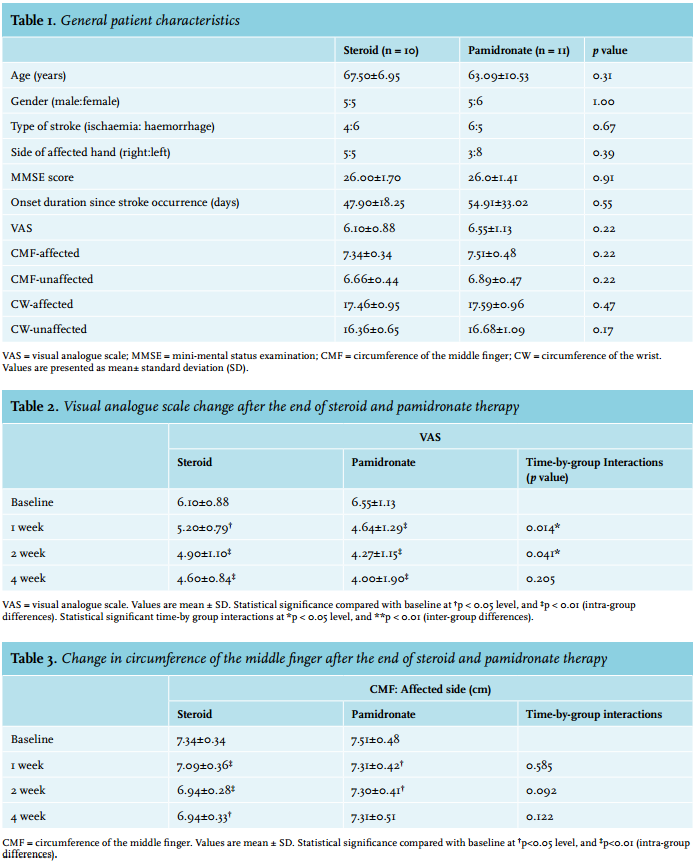
DISCUSSION
Our results revealed that pamidronate was as effective as a steroid for pain control in CRPS type I after stroke, but less effective than a steroid for hand swelling. Post-stroke CRPS is usually observed in the paralysed upper extremity with pain, warmness and oedema involving the shoulder and hand. Inflammatory processes and sympatheticafferent coupling contribute to the peripheral sensitisation of nociceptive fibres. The affected limb presents increased blood flow and vascular permeability and low norepinephrine concentrations from the venous effluent above the painful area, compared with contralateral one.21 These inflammatory and vasomotor responses also play an important role in oedema.22 Early and effective control of the inflammatory process is important to prevent disability and improve rehabilitation outcomes.23,24
Until now, steroids have been the main treatment option for CRPS in stroke patients. Oral steroids control the inflammatory processes of the patients with CRPS whose oedema, warmness and reddening of skin are clinically detectable.25 However, steroids can cause serious side effects such as endocrine system disruption including adrenal insufficiency, deteriorating diabetes mellitus, deteriorating osteoporosis, high blood pressure and ulcerative change in the digestive system. Thus, physicians must pay close attention to the use of steroids in these patients.
In light of the need for an alternative safe treatment option, the current study was conducted to quantify the effectiveness of a bisphosphonate alternative to steroid therapy on the treatment of post-stroke CRPS. In this study, both the steroid and the intravenous bisphosphonate groups showed significant improvement in pain at one week after drug administration, and this effect lasted until four weeks of follow-up. The effectiveness of pamidronate for pain control was not inferior to the steroid. There were no serious adverse effects during and after pamidronate administration. In addition, pamidronate is easy to administrate for stroke patients, who often have difficulty in taking lots of pills due to dysphagia. Therefore, we conclude that pamidronate infusions are well tolerated and easy to administrate, and are also as effective as steroid therapy for pain control in post-stroke CRPS. Furthermore, administration of pamidronate may help the disabled stroke patients who are at risk of osteoporosis in terms of preventing bone loss.
The mechanism of the analgesic effect of bisphosphonates remains undetermined. Bisphosphonates have antinociceptive properties in a variety of bone and joint disorders,26,27 as well as in pain unrelated to bone and joint diseases.28 Peripheral mechanisms predominate in the early phase of CRPS and central mechanisms dominate in the later phase.29 The pain relief properties might be induced by inhibiting the production of either proinflammatory cytokines such as interleukin-1, prostaglandins, lactic acid and/or various neuropeptides and neuromodulators, all of which are possibly involved in the sensitisation of afferent nerve fibres and pain modulation.28,30 Highly water-soluble bisphosphonates might also have a central antinociceptive action, possibly through mechanisms involving ionised calcium31 by inhibiting the influx of calcium that is crucial for the release of neurotransmitters and other substances implicated in nociception and inflammation.32,33
The results of most studies on this topic show that bisphosphonates may be effective in the early phases of the disease,34 when scintigraphic bone scan more frequently shows a local radiotracer accumulation that possibly means a high local concentration of the drug. These features probably represent the required conditions by which bisphosphonates might modulate various inflammatory mediators that are upregulated in CRPS-I.35 In the current study, we included only stroke patients in the acute and subacute phases, and treatment was started as soon as possible after they were diagnosed as CRPS. This could have had a favourable effect on the outcomes of pamidronate treatment.
Few studies on the use of bisphosphonate to treat CRPS have achieved consistently positive results in a randomised, double-blinded, placebo-controlled setting.8 Adami et al.18 reported that after two weeks of treatment, patients receiving a three-day course of intravenous alendronate presented significant improvement in pain, swelling and range of motion compared with the control group. In the study by Manicourt et al.14 participants receiving alendronate displayed better pain control and range of motion compared with controls at four, eight and 12 weeks. Moreover, oedema was also improved with alendronate at four and eight weeks. In 2000, Varenna et al.36 reported that 40 days after treatment, subjects receiving clodronate displayed significantly greater improvement on pain, clinical global assessment and efficacy verbal scores compared with controls. In 2004, Robinson et al.12 reported that at the three-month evaluation, subjects who had received bisphosphonate reported lower pain scores and higher functional assessment scores pertaining to physical function. However, these studies were in the placebocontrolled setting. To the best of our knowledge, no study has compared the effectiveness of bisphosphonate with steroids.
Pamidronate showed a therapeutic effect on hand oedema; however, its effectiveness was inferior to that of the steroid. From this result, we propose pamidronate as an alternative to steroid in the case of post-stroke CRPS where pain is a dominant symptom. Even with both pain and severe swelling, we could use a pamidronate first and add a steroid later if there is no improvement to the swelling after pamidronate therapy.
The current study has some limitations as it was only conducted in a small number of patients. In addition, hormones related to bone metabolism or bone densitometry, which may help to identify the mechanism by which of bisphosphonate works, were not evaluated. However, the current study showed important findings and has several advantages over previous studies. First, this study involved a homogeneous patient group, i.e., post-stroke CRPS patients. Second, this is the first randomised controlled trial to compare bisphosphonate with a steroid in stroke patients with CRPS for four weeks after the administration of bisphosphonate, and the first to make serial quantitative measures of hand swelling.
CONCLUSION
In this study we observed that intravenous pamidronate therapy was safe, well tolerated and appeared as effective as steroid for pain control of post-stroke CRPS. However, this result should be interpreted with caution, since it included a relatively small number of patients. Further larger controlled studies followed over a longer period are needed to validate these findings and to determine clinical treatment standards, i.e., the optimum dose and duration of administration when using bisphosphonate to treat CRPS after stroke.
DISCLOSURES
This work was supported by a grant from the Jeju National University Hospital Research Fund (2010).
REFERENCES