KEYWORDS
Blood pressure, cardiovascular disease, hypertension, kidney function, renal denervation
INTRODUCTION
Renal denervation
Percutaneous renal sympathetic denervation (RDN) is currently being used as a potential treatment for therapyresistant hypertension and other conditions associated with increased sympathetic activity. The treatment aims to disrupt afferent and efferent nerves travelling around the renal artery with the intention to lower systemic sympathetic activity.
At the beginning of the initiative for the current registry in 2010, RDN was an upcoming therapy for resistant hypertension. The initial report in The Lancet showing the results from the first 50 patients, was followed by great enthusiasm for RDN.1 Because of many uncertainties at that time and still, we initiated a national registry.
Since 2009, a range of studies has been conducted including many cohort studies (uncontrolled) and some randomised controlled trials. Almost all studies reported a significant decrease in blood pressure, six to twelve months after the procedure.1-5 However, not all trials showed superiority of RDN when compared with a control group.6,7 The largest, the Simplicity HTN-3 trial, a randomised, blinded trial, showed no statistically significant effect of RDN compared with a sham procedure and so the RDN landscape changed in 2014.7 A recently published meta-analysis acknowledged the safety of the procedure and argued for the identification of responders in future trials.8
Effects
Not only blood pressure effects have been studied; various cohort studies showed positive results on other aspects, such as an improvement in glucose metabolism and cardiac function.9,10 Although these studies were not properly controlled, the findings are in line with the pathophysiology.11,12 Since nerve ablation is non-selective, one can imagine that sensory nerves will also be affected. Case reports have been published in which patients with kidney-related pain syndromes were successfully treated by RDN.13,14
Predictors
Effort has been made to identify characteristics, both patient and procedure related, that seem to predict a better outcome after RDN. For example, the use of aldosterone antagonists, the number and location of ablations, office systolic blood pressure at baseline, the estimated glomerular filtration rate (eGFR) and the presence of diabetes mellitus have been mentioned as predictors for efficacy of RDN.15-19 Most of these possible predictors could not be confirmed in other studies or even contradicting relations were suggested.15,17,18,20 These conflicting data underscore the need for more extended research.
Safety
Overall, the intervention appeared to be safe. Some cases of renal artery stenosis during follow-up were reported. The reported rates of vascular complications range from 0.3% to 4.3%.4,7,20-23 Time between procedure and renal artery imaging varied from six months to three years. Three years is the longest follow-up after RDN that has been described in literature, for both efficacy and complication rate.21,24 To date, there are no reports on the effects of RDN on the cardiovascular event rate or mortality.
Registration
It is clear that there are still many uncertainties with regard to patient selection, effectiveness and complications, especially long-term outcomes. Available information is predominantly based on small and strictly selected patient groups. Follow-up details are scarce and reports on the comparison of different devices, or on consistently shown predictors for success, are lacking. The Dutch RDN registry initiative is designed to combine all Dutch data on RDN from routine clinical practice in order to contribute to clarifying the effects of this treatment.
OBJECTIVES
The main goal is to collect data concerning three important issues: safety, predictors for success and the long-term effects of RDN.
Safety
1. What are the short- and long-term procedural-related complications?
Predictors
2. What are the predictors for a beneficial effect on blood pressure, in particular patient-related factors and procedural-related factors?
3. Is the effectiveness of the currently available RDN devices comparable?
Long-term effects
4. What is the effect on blood pressure at various time points, up to at least five years after RDN?
5. What is the effect on kidney function at various time points, up to at least five years after RDN?
6. What are the cardiovascular event rates, in strata of achieved blood pressure level?
MATERIALS AND METHODS
Design and population
The Dutch RDN registry is an ongoing investigatorinitiated, prospective, multicentre cohort study. Twenty-six Dutch hospitals agreed to participate in this registry (Appendix A). This is approximately 28% of all hospitals in the Netherlands and includes, to our knowledge, all hospitals in which RDN is being performed. Despite willingness to share data on RDN, not all participating centres have entered data at the time of writing. All patients who underwent RDN, regardless of indication for RDN or the device that was used, are to be included in the registry. Patients must be at least 18 years of age, but there are no other specific inclusion or exclusion criteria. The indication for RDN is left to the discretion of the treating physician. Endpoint analyses will be stratified according to indication for treatment, and analyses on safety and long-term effects will be performed based on the total cohort. The registry was originally initiated to include 1000 patients within 36 months, with a minimal duration of five years. Given the current enrolment rate, this period is being extended.
Sample size considerations
At the start of the registry, several sample size considerations were discussed, based on addressing the research questions. With 1000 participants we estimated to detect a procedural complication rate of at least 1% with sufficient precision (between 0.38% and 1.6%). Based on the reports by Esler et al., 8% of the participants who underwent RDN actually increased usage of blood pressure lowering drugs.2 In the same study, 10% of the patients who underwent RDN had a systolic arterial pressure drop < 10 mmHg. If these findings are consistent, we expect that 80-100 patients in our cohort of 1000 patients can be considered to be ‘failures’ or ‘non-responders’. This would allow for the evaluation of 8-12 factors for the development of a prediction rule to estimate the risk of failure based on baseline characteristics.25-28 Importantly, to be able to identify responders, we believe that blood pressure change after RDN should be adjusted for the change in blood pressure lowering medication.
With regard to the long-term effects, we assume to have sufficient precision to estimate treatment effects on blood pressure and renal function overall and for various subgroups (age, sex, baseline blood pressure, renal function). Furthermore, event rates observed in the registry will be compared with unpublished estimates of cardiovascular event risks in patients with therapyresistant hypertension, obtained from existing Dutch cohorts (approximately 8% (95% CI 6.3, 9.6)) within three years.29,30 Potential confounding factors will be taken into account. We will be able to detect an event rate of 5% (95% CI 3.6, 6.4) or lower in the RDN cohort, which means a statistically significant reduction in cardiovascular risk.
Baseline, procedure and follow-up
Information from the first visit to the outpatient clinic and subsequently the investigations to determine eligibility will be collected (table 1). 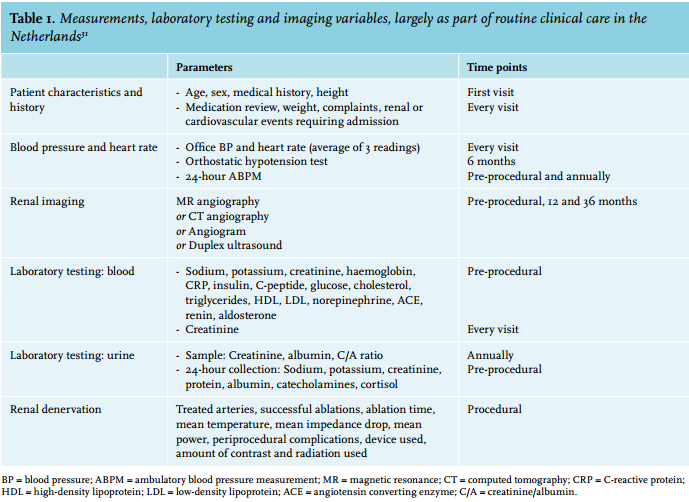
Recommended follow-up visits are at 3, 6, 9, 12, 18, 24, 30, 36, 48 and 60 months after RDN. We aim to continue annual follow-up of the patients after these 60 months as well. Table 1 shows a list of proposed pre-procedural, procedural and follow-up variables that are recommended to be registered. All participating centres received the list of variables at the start of the study. This can be used as a guideline and is not mandatory. Nevertheless, some data are specifically recommended and part of the standard care in most hospitals following the Dutch guideline on RDN:31 office blood pressure and heart rate (both as a mean of three measurements), serum creatinine, weight and data on medication use, events and complications. Moreover, 24-hour ambulatory blood pressure measurement data are collected, as is annual measurement of urine creatinine and protein levels and imaging of the kidneys (and renal arteries) at 12 and 36 months. For follow-up imaging, the same modality as during screening for eligibility is preferably used.
As stated before, most objectives and therefore most information will be gathered from patients who suffer from therapy-resistant hypertension and we expect this to be the predominant indication for RDN. Event follow-up (defined below) is obtained in two ways. Firstly, information is collected through the data entry in the database by the individual investigator. Secondly, the dataset is linked with the Dutch Hospital Discharge Register (HDR) (the LMR) and with Statistics Netherlands (the CBS) to obtain information on hospital discharge diagnoses and causes of death, respectively.
Outcome parameters, definitions and data analysis
Outcome of the stated objectives will be based on the following parameters.
Short-term procedural complications: haematoma, bleeding, false aneurysm, renal artery perforation or dissection, renal failure, adverse contrast effects, infection, and death. This will be presented as percentages by age and sex with corresponding 95% confidence limits. Additional analyses will be performed to relate patient characteristics to the risk of short-term complications. For these analyses, multilevel multivariable (logistic) regression models will be used.
Long-term procedural and effect complications: renal artery stenosis or other vascular complications, decline in kidney function, (orthostatic) hypotension. Data will be presented as incidence rates (per person-years of follow-up) by age and sex with 95% confidence limits. Additional analyses will be performed to relate patient characteristics and procedural aspects to the risk of short- and long-term complications using multilevel multivariable regression models. Results will be reported as hazard ratios with corresponding 95% confidence limits.
Change in blood pressure and kidney function at various time points: change over time will be analysed by use of linear mixed-effects models. Factors that contribute to the initial effects and to the long-term effects will be assessed. (‘Responder’ has already been defined). Multilevel multivariable regression models will be used to explore the relation between responders and non-responders and baseline characteristics /procedural characteristics. Results will be presented as hazard ratios with corresponding 95% confidence limits. Stratified analyses will be performed in strata of ‘blood pressure measurement with and without being on medication’. The results from the regression model will be used to make a prediction rule with which the absolute probability of success or failure will be estimated from baseline characteristics.
Safety analyses and effectiveness endpoints stratified per device: the different devices will be related to the magnitude of the blood pressure change using univariable and multivariable regression models. Multilevel multivariable regression models will be used to adjust for potential confounding (by indication) variables.
Rate of events requiring admission: acute coronary syndrome, transient ischaemic attack, ischaemic or haemorrhagic cerebrovascular accident, peripheral arterial ischaemia, congestive heart failure, renal failure and mortality. Analyses with regard to risk of events, in strata of baseline and/or follow-up characteristics, will be performed using multilevel multivariable regression models.
Furthermore, as a general approach, in all analyses differences across centres will be explored.
Ethical considerations
The registry is being conducted according to the principles of the Declaration of Helsinki and in accordance with the Medical Research Involving Human Subjects Act (the WMO). Patients are informed about the procedure by their treating physician. This registry is approved by the Medical Research Ethics Committee of the University Medical Centre Utrecht and registered at ClinicalTrials. gov: NCT02482103.
Data management
All data are entered into a web-based electronic Case Report Form. Data management is performed by the Julius Center for Health Sciences and Primary Care at the University Medical Centre Utrecht, Utrecht, the Netherlands.
Sponsoring
This study is initiated and supported by the University Medical Center Utrecht in the Netherlands. Funding is in part obtained from the Dutch Kidney Foundation (Nierstichting), project number CPI12.02.
RESULTS
General description
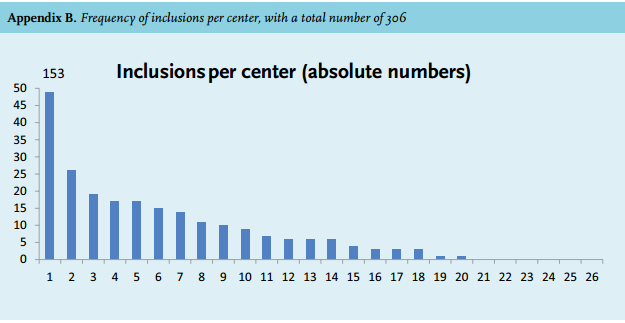
On 23 March 2015, data of 306 patients had been entered into the database (inclusions per centre are shown in Appendix B). Procedures have been performed since August 2010. Table 2 shows the available baseline characteristics of these patients, enrolled by 20 hospitals. In 302 patients, the indication for RDN was hypertension. Four patients were treated because of kidney-related pain syndromes.
Blood pressure
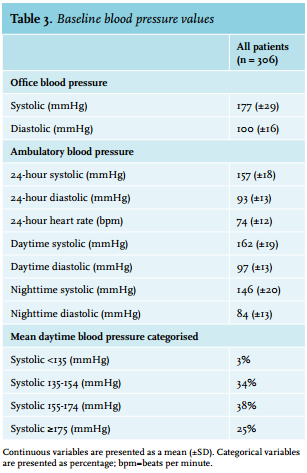
Blood pressure is shown as office measurements and as 24-hour measurements when available (table 3). In almost half of the patients, the 24-hour measurement was performed during a period of partial or complete medication stop, due to centre-specific investigations.32 The overall mean systolic 24-hour blood pressure was 157±18 mmHg. Approximately 25% of the patients had a mean daytime systolic blood pressure of more than 175 mmHg. Mean office blood pressure was 177±29 mmHg.
Medication
In table 2 the medication details are presented. The prescribed medications of the patients who temporarily stopped their treatment are taken into account in this table. Therefore, medication use corresponds with office blood pressure values but not with 24-hour values. The most commonly used drugs were renin-angiotensinaldosterone system (RAAS) inhibitors (79%), diuretics (70%), calcium-channel blockers (64%), beta-blockers (61%) and alpha-blockers (23%). The use of other blood pressure lowering drugs (centrally-acting sympatholytic agents, direct-acting vasodilating drugs and nitrates) was low (11%). Aldosterone antagonists (mainly spironolactone) were used by 25% of the individuals. The median number of prescribed antihypertensive drugs was three, ranging from 0-8, with a mean daily use of 5.4±3.7 units. Interestingly, 14 patients did not use any blood pressure lowering drugs at all. Five of these patients were intolerant to many different drugs. Another five of these patients have never used any antihypertensive drugs, due to borderline hypertension. Of the remaining four patients, it was unknown why no antihypertensive drugs were prescribed.
Device
The most frequently used device for RDN was the Symplicity™ catheter (Medtronic, Santa Rosa, CA, USA) (88%). Apart from the Simplicity™ catheter, four other devices were used in more than 10% of the cases.
Comorbidities
The presented comorbidities in table 2 are based on the medical history (not on medication use). Dyslipidaemia was present in 42% of the cases and approximately 21% of the patients were diagnosed with diabetes mellitus. 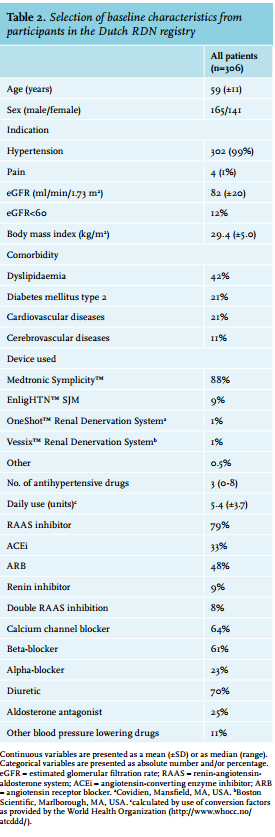
DISCUSSION
We report the first baseline characteristics from an investigator-initiated national registry for RDN. The Dutch RDN registry strives for complete coverage, which means that all patients who underwent an RDN procedure in the Netherlands are to be included. Inclusion is not restricted by specific criteria. Therefore, these data represent real-world clinical practice of RDN in the Netherlands.
The main underlying reason for this initiative is that including the data from all centres and all patients in one study provides faster and more valuable insight into complications and effectiveness when compared with single-centre reports with relatively small numbers of patients. This is especially important for RDN since this new procedure is at the beginning of evaluation in routine clinical practice. Furthermore, a registry may lead to uniformity in data collection, which allows for pooling of the data. Finally, for identification of predictors of response, a large number of patients is needed.
Globally, RDN has been performed on a large scale. Unfortunately, only a fraction of the treated patients has been adequately registered. We estimate, based on correspondence with manufacturers and hospitals, that approximately 70% of the performed procedures in the Netherlands are currently included in this registry. Several registries exist world-wide, of which the Global SYMPLICITY registry, initiated by Medtronic, contains the largest number of patients. Its baseline data were published in 2013 and the first results in 2015.33,34 An important aspect is that the Symplicity™ catheter was exclusively used in the Global SYMPLICITY registry. Due to former reimbursement policies, this device was also most frequently used in the Netherlands up to 2014. Since late 2014, the multi-electrode EnligHTN™ catheter (St Jude Medical, St Paul, MN, USA) has also been approved for conditional reimbursement.
In the literature, RDN was introduced as treatment for therapy-resistant hypertension, defined as a blood pressure ≥ 140/90 mmHg despite appropriate lifestyle measures and the use of a diuretic and two other antihypertensive drugs (adequately dosed).35 These data show that in clinical practice, this definition was not guiding the selection of patients: several patients did not use three or more drugs and diuretics were only prescribed in 70% of the cases.
There are few other RDN registries that we are aware of. Table 4 gives an overview of the results of our search in PubMed, trial registers and Google on 1 June 2015, using the search terms “renal denervation” and “registry”. Multicentre investigator-driven registries for RDN regardless of device, such as the present registry, seem to be scarce. However, we may not have found all registries using the above-mentioned sources and search terms. It is of importance to note that patients registered in our registry can also be registered elsewhere, since it is up to the principal investigator of the centre to decide whether or not to participate in other registries. This is a relevant issue when data from various registries are pooled. The Dutch registry and the Global SYMPLICITY registry differ in several ways, for example with regard to comorbidities and prescribed drugs. In the Global SYMPLICITY registry, the prevalence of diabetes mellitus and chronic kidney disease is considerably higher (41% vs. 21% and 22% vs. 12% in the Dutch RDN registry) and sympathetic blocking agents, both beta-blockers and centrally-acting sympatholytic drugs, are prescribed far more often (77% vs. 61% and 40% vs. < 11% in the Dutch RDN registry).
Although hypertension is the main indication for RDN in the majority of patients, the dataset contains a few patients who underwent RDN to treat kidney-related pain syndromes. So far, percutaneous RDN for this specific indication has only been described in case reports.13,14
Furthermore, the Dutch registration aims to collect detailed procedural information that might be related to outcome. In the literature, several procedural aspects have been related to a better outcome. A previous study revealed a positive correlation between the number of ablation points and the reduction in office blood pressure after RDN.15 Also a positive relation between the ablation points placed close to the kidney and the reduction in blood pressure was found.15,16 Follow-up data from the RDN registry might contribute to these findings. 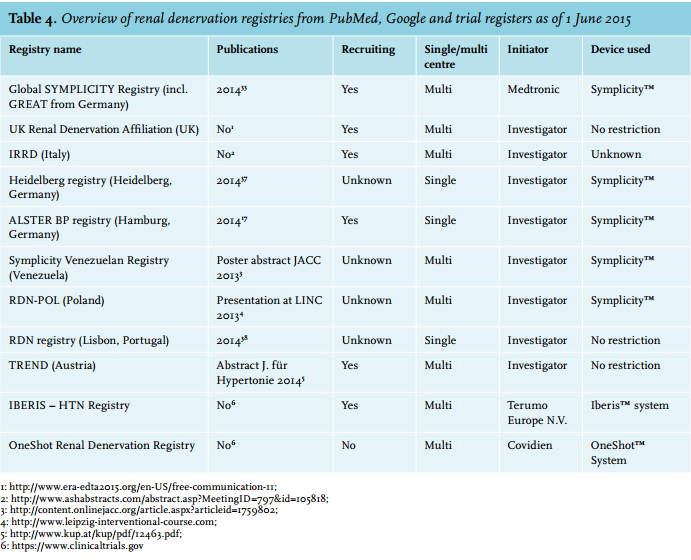
Methodological challenges
The initiation of a national registry using data that are routinely collected has a number of methodological challenges that may hamper the validity of the findings. Without being exhaustive, a few important ones are mentioned. Firstly, the issue around ‘confounding by indication’, that is the effect of patient selection on the outcome of the study, is likely to be of importance, especially when investigating predictors for success.36 Measurement of potential confounders may take away part of the problem.
Secondly, differences across centres in contribution to the registry (size) and difference in measurement protocols are inevitable, but may prove to be important. Therefore, as mentioned in the ‘Materials and Methods’ section, differences across centres will be explored in all analyses. The third challenge, especially in RDN, is adherence to medication. Our registry in its current phase is based on routine clinical practice. In that setting, information on adherence is not routinely collected. In addition, tools to monitor adherence all have their limitations, and drug levels in blood are generally not measured in these patients.
CONCLUSION
Renal denervation is a promising treatment for patients suffering from therapy-resistant hypertension or other diseases related to sympathetic overactivity. The Dutch RDN registry is a collaboration of 26 hospitals in the Netherlands, initiated with the intention to increase our knowledge of this therapy by pooling data of all patients treated with RDN in the Netherlands. Combining data from all centres in one registry should result in faster and more valuable insight into complications and effectiveness, when compared with single-centre cohorts. At the time of writing, 306 patients have been included. Detailed analyses will follow, reporting on safety, effectiveness, predictors of response and potential differences between currently available devices.
DISCLOSURES
M.F. Sanders has nothing to disclose. P.J. Blankestijn reports grants from the Dutch Kidney Foundation during the conduct of the study; grants from Medtronic and St. Jude, other from Medtronic and St. Jude, grants from ZonMw (The Netherlands Organisation for Health Research and Development) outside the submitted work. M.L. Bots reports grants from the Dutch Kidney Foundation during the conduct of the study; grants from Medtronic and ZonMw (The Netherlands Organisation for Health Research and Development) outside the submitted work. The other authors have nothing to disclose.
REFERENCES