KEYWORDS
Malignant paraganglioma, catecholamines, cardiomyopathy, SDHA-germline mutation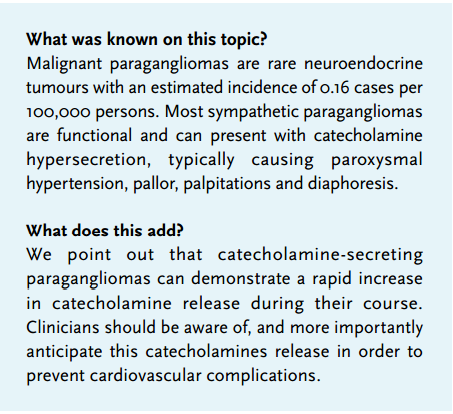
INTRODUCTION
Paragangliomas are rare neuroendocrine tumours deriving from chromaffin cells. Only 15-20% of chromaffin-cell tumours are extra-adrenal paragangliomas, 80-85% being adrenal pheochromocytomas.1 Most paragangliomas occur as sporadic tumours, but 30-35% are associated with hereditary syndromes or germ-line mutations in susceptibility genes. Malignancy, defined as metastasis in non-chromaffin tissue, is reported in 10-17% of all paragangliomas.1-2,3 Paragangliomas commonly produce one or more types of catecholamines: epinephrine, norepinephrine and dopamine. High levels of catecholamines can result in cardiovascular complications, varying from hypertension and palpitations to acute ventricular dysfunction due to a catecholamine-induced cardiomyopathy. Stress cardiomyopathy (or Takotsubo cardiomyopathy) is an acute, transient ventricular dysfunction displaying severe left ventricular wall motion abnormalities. It often mimics an acute coronary syndrome in the absence of coronary artery disease. Precipitants of Takotsubo cardiomyopathy are numerous but catecholamine mediated β2-adrenoceptor stimulation is thought to be an important common component in the aetiology.4 Here, we report a case of a patient suffering from a malignant paraganglioma who died as a result of an overwhelming catecholamine-release and subsequent cardiopulmonary complications.
CASE REPORT
A 36-year-old man was diagnosed with a retroperitoneal malignant paraganglioma. Further evaluation included a CT scan showing irresectable, retroperitoneal masses, and liver and bone metastases; MIBG scintigraphy and Octreoscan which did not yield treatment options for 131I-MIBG therapy or peptide-receptor radiotherapy with 177Lutetium octreotate. Therefore it was decided to start palliative chemotherapy treatment. Although the more commonly used chemotherapy regimens for malignant paragangliomas include cyclophosphamide, vincristine, and dacarbazine, it was decided to treat this malignant paraganglioma as a small-cell malignancy because of a small-cell component that was found at histopathology and the aggressive nature of the tumour. The patient was started on four-weekly cycles of intravenous carboplatin (AUC 5 on day 1) and etoposide (100 mg/ m2 days 1-3). A follow-up CT scan after the second cycle showed disease progression and the chemotherapy was discontinued. Thereafter the patient was evaluated for phase I study treatment. However, within six weeks, our patient was admitted because of an impending thoracic paraplegia at the level of Th7. The patient was started on dexamethasone and received emergency radiotherapy (8 Gy) at Th 5-Th9 and L1-L4 and extensive radiation to the retroperitoneal mass. Treatment resulted in stabilisation of his neurological symptoms. After four days the patient developed a sudden tachypnoea with SpO2 92% and marked jugular venous distention. A chest X-ray showed bilateral pulmonary oedema. An ECG showed a sinus tachycardia of 148 bpm, with signs of left ventricular hypertrophy with abnormal repolarisation. Blood pressure was 110/70 mmHg. Transthoracic echocardiogram revealed severely impaired left ventricular function which was described as almost functionally asystolic (echocardiography images are available in the online supplement). There was no pericardial effusion and intravenous diuretics were started. The possibility of a Takotsubo-like cardiomyopathy as a result of catecholamine release by the paraganglioma was suggested. At the time of diagnosis, the patient’s normetanephrine excretion in the urine was increased (normetanephrine 5558 µmol/ mol creatinine (reference: 70-260 µmol/mol creatinine)), and the patient was subsequently given doxazosin 4 mg once daily to pre-emptively reduce potential blood pressure elevation. Until now, our patient had never displayed any clinical signs of excessive catecholamine production (e.g. hypertension or flushes); however, during the current admission he started complaining of sweats and palpitations. A urinary sample was collected to determine the current normetanephrine levels. The differential diagnosis included pulmonary embolism, but this was thought to be less likely because of the use of prophylactic low-molecular-weight heparin and an alternative explanation was sought. Meanwhile, the patient’s condition deteriorated rapidly. Due to the underlying malignant disease without any therapeutic options, it was decided together with the patient and his family that inotropic support or admission to the intensive care unit was not an option. Eventually palliative sedation was started and our patient passed away the subsequent day. Autopsy surprisingly revealed a saddle embolus in the pulmonary artery. The heart was found to be enlarged (610 grams (reference: 330 grams in males)) with dilated, non-hypertrophic, ventricles, without obstructive coronary artery disease. DNA analysis revealed an SDHA-germ line mutation, explaining the occurrence of a malignant paraganglioma at our patient’s young age. This rare mutation has a dominant autosomal inherence pattern. Currently there are only 14 known patients in the Netherlands with SDHA-germline mutations associated paragangliomas. The pathologist’s first conclusion was: ‘death as a result of pulmonary embolism’. However, the urinary sample came back revealing astounding amounts of normetanephrine (37,240 µmol/mol creatinine (reference: 70-260 µmol/ mol creatinine)) and 3-methoxytyramine (8218 mmol/mol (reference 0.4-1.5 mmol/mol creatinine)). These results led to the second hypothesis of catecholamine-induced cardiomyopathy as we will now continue to discuss.
DISCUSSION
Catecholamine-secreting paragangliomas produce one or more catecholamines. The sensitivity of catecholamine measurement in plasma is limited by the episodic release from tumour cells.5. A more accurate test involves measurement of metanephrines (normetanephrine and metanephrine) in plasma or urine.6 These metabolites are produced continuously within the tumour, independent of intermittent catecholamine release. As depicted in the case report, the normetanephrine and metanephrine levels in our patient were raised dramatically. Assuming that our patient died as a result of cardiac failure and the formation of a pulmonary embolism due to excessive catecholamine release, the question arises whether this could have been prevented. Retrospectively, there were accumulating factors that might have negatively influenced the patient’s outcome. First of all, the disease was rapidly progressive in this patient. Furthermore, little is known about the effects of radiation therapy in the treatment of malignant paraganglioma, which is usually reserved for inoperable or relapsed cases. Vogel et al.7 showed that radiation therapy can be safely used in the case of skeletal metastasis, but no recommendations are available on soft-tissue metastasis. We hypothesise that extensive radiation on the surrounding retroperitoneal mass might have led to increased release of catecholamines from the tumour by cell lysis. The two chemotherapy cycles in this patient were not accompanied by haemodynamic changes, but perhaps insufficient cell lysis was induced, besides a 24-hour blood pressure measurement was never performed. Nevertheless, there might be a rationale for a higher degree of alpha-adrenergic receptor blockade during radiotherapy and chemotherapy for malignant pheochromocytoma/paraganglioma, similar to the preoperative treatment with doxazosin or phenoxybenzamine in patients with these disorders.8 Secondly it is known that certain medications may alter catecholamine levels, such as dopamine D2-receptor antagonists, opioid analgesics, corticosteroids, β-adrenergic receptor blockers and SSRIs. On admission, our patient was on transdermal fentanyl, oxycodone immediate release (IR), dexamethasone, and metoclopramide. Because of the radiotherapy the dexamethasone dose was altered from 3 mg daily to 8 mg twice daily after a single intravenous bolus of 10 mg. Simultaneously fentanyl was raised from 50 to 100 µg along with oxycodone IR 20 mg six times a day. Of course these were sensible clinical actions but we cannot exclude exacerbation of catecholamine release. The acute management of catecholamine-induced cardiomyopathy should be aimed at lowering sympathetic activation by means of an α-adrenergic receptor blocker, diuretics in case of volume overload, β-blocker administration to slow the heart rate and increase end-systolic volume and anticoagulation with heparin to prevent left ventricular thrombus formation.9
CONCLUSION
We want to emphasise that clinicians should be aware of the potentially life-threatening increase in catecholamine release in paragangliomas during the course of disease and treatment. In the case of catecholamine-producing tumours we would advise to regularly check for clinical signs of raised catecholamine release (e.g. palpitations, diaphoresis, flushed of raised blood pressure (consider ambulatory blood pressure measurement)), consider increase of α-adrenergic receptor blocking medication prior to radiotherapy on soft-tissue metastasis, avoid medications that can raise catecholamine excretion and increase awareness among the medical staff with regard to the potential clinical signs of excess catecholamine levels in order to respond rapidly and, hopefully, avoid cardiovascular collapse.
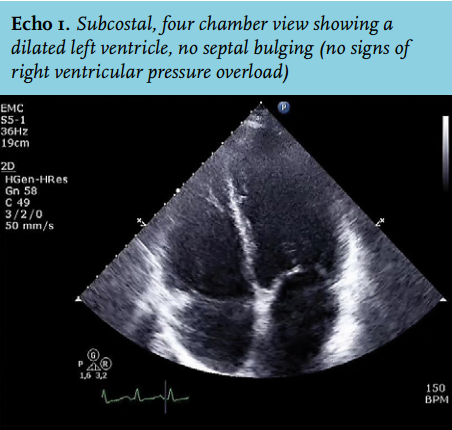
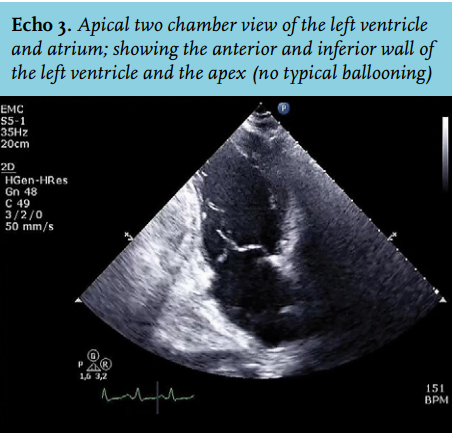
Online supplement: echocardiography images of this patient, showing the severely impaired left ventricular function:
Echo 1. Subcostal, four-chamber view showing a dilated left ventricle with impaired function, no septal bulging (no signs of right ventricular pressure overload), and a reasonable longitudinal contractility of the right ventricle compared with the left ventricle
Echo 2. Short-axis, mid-ventricular view, again showing globally impaired contractility of the left ventricle
Echo 3. Apical two-chamber view of the left ventricle and atrium, showing the anterior wall of the left ventricle, the apex (no typical ballooning) and inferior wall
Echo 4. Apical three-chamber view, showing the aortic valve and aortic root and the impaired contractility of the anterolateral and posterior walls of the left ventricle
|
DISCLOSURES
The authors declare no conflict of interests.
REFERENCES