KEYWORDS
Aortic dissection, CT scan, chest pain, Horner’s syndrome 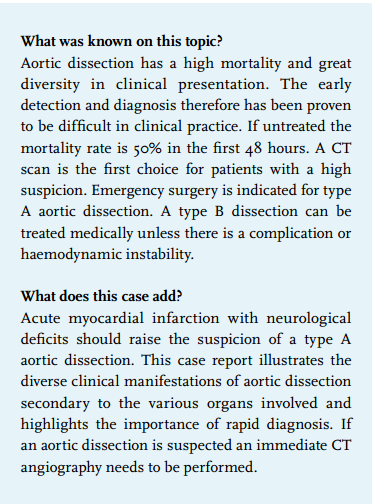 INTRODUCTION
INTRODUCTION
The differential diagnosis of chest pain is extremely diverse. In acute chest pain accompanied by somnolence and neurological deficits, one should be aware of serious diseases such as pulmonary embolism, acute myocardial infarction, severe aortic valve stenosis, left-sided endocarditis with embolisation, or aortic dissection. In this context we discuss a dramatic case of chest pain in a 79-year-old man with somnolence and Horner’s syndrome.
CASE REPORT
A 79-year-old man was presented in the emergency department because of an acute violent and sharp pain located retrosternally and in the throat. Patient was known with hypertension, a coronary stent and a dilated aortic root (diameter 53 mm; stable for years) with a tricuspid aortic valve. The patient was somnolent with a significant difference in blood pressure in the two upper extremities (right 85/40 vs. left 110/60 mmHg) and cold extremities with normal peripheral oxygen saturation. Physical examination of the heart, lungs and arteries revealed no abnormalities. The right pupil was constricted with drooping of the eyelid. An electrocardiogram showed no abnormalities except sinus bradycardia. Blood tests showed a normal C-reactive protein, but a prolonged international normalised ratio (INR) (2.7) with thrombocytopenia (113 x 109/l) and a normocytic anaemia (haemoglobin 6.1 mmol/l). The chest X-ray showed no abnormalities.
The most likely diagnosis was aortic dissection with neurological symptoms fitting Horner’s syndrome. This was supported by the difference in blood pressure between the left and the right arm together with the spontaneously prolonged INR, thrombocytopenia and anaemia. However, in the meantime the chest pain increased. A new electrocardiogram showed signs of acute inferior myocardial infarction and the patient deteriorated haemodynamically. CT angiography demonstrated aortic dissection from the aortic valve to the renal arteries, extending to the right coronary artery, the common carotid artery and the right and left subclavian artery with a minimal antegrade flow in the ascending aorta (figure 1a). Taking into account the age of the patient, the complexity of the dissection and the high mortality from operation in a haemodynamically poor initial situation it was decided, in collaboration with the family, to refrain from surgery. The patient died three hours after presentation. Autopsy confirmed the diagnosis of type A aortic dissection. The defect in the arterial wall was situated in an atherosclerotic plaque in the ascending aorta and extended to the descending anterior branch (figure 1b), the right coronary artery, the right common carotid artery (until the bifurcation) (figure 1c), right and left subclavian artery, and along the aorta (until 8 cm above the level of the renal arteries origin). 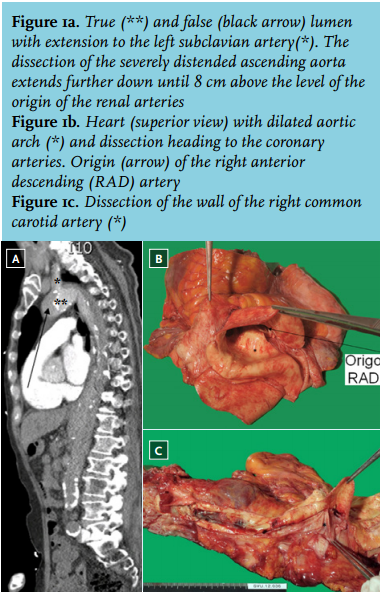
DISCUSSION
This case is illustrative of the differential diagnostic thinking in a patient with acute chest pain with neurological symptoms. The two most commonly involved organ systems in the process of aortic dissection are the cardiovascular and neurological system.11 Alarming findings with this presentation were the experienced subjective somnolence in combination with haemodynamic instability. This may fit insufficient cerebral perfusion, which is a sign of (impending) shock. It is important to quickly identify the cause. In this case there were several signals that pointed to aortic dissection. The nature of the pain (acute, violent and sharp) was in line with the classic presentation of aortic dissection. The spontaneously prolonged INR and thrombocytopenia indicate diffuse intravascular clotting as a result of bleeding in the aortic wall. In addition, the clinical diagnosis is supported by the difference in blood pressure between the arms (> 20 mmHg). Striking in this case were the miosis and ptosis of the right eye. This is a result of compression of the sympathetic fibres of either the preganglionic neuron (dissection of the subclavian artery), or of the postganglionic neuron (dissection of the internal carotid artery). In this case the cause was most likely preganglionic as the dissection extended to just after the origin of the right subclavian artery. Other possible neurological manifestations of an aortic dissection are a cerebrovascular accident, syncope, vocal cord paralysis and hoarseness. Cerebral ischaemia/stroke is the most common neurological manifestation associated with aortic dissection and has been reported to affect 5-10% of patients.8-10 Most patients with aortic dissections who present with stroke also reveal a history of chest pain. Besides stroke, the altered cerebral perfusion may cause symptoms of transient cerebral hypoperfusion ranging from altered mental status to syncope.11 The subacute inferior myocardial infarction was the result of compression of the right coronary artery by extension of the ascending aortic dissection 2 cm beyond the origin of this artery.
Dissection of the aorta has a low prevalence and high mortality. A dissection is created by a tear in the intima resulting in a progressive ‘false’ lumen in the wall of the vessel. Extension of the dissection can lead to a diverse clinical spectrum. The clinical manifestations depend on which of the various branches of the aorta, the pericardium, the coronaries and/or the aortic valve are involved (table 1). The early detection and diagnosis, therefore, has been proven to be difficult in clinical practice. In 25-50% of patients with an aortic dissection the wrong diagnosis is made.1,3,4 The diagnosis of aortic dissection begins with clinical suspicion, which is the most crucial step in diagnosing this catastrophic disease.11,12 The mortality rate for patients with untreated proximal aortic dissections has been reported to increase by 1-3% per hour after presentation and is approximately 50% during the first 48 hours after the initial presentation.5,6 Rapid diagnosis and treatment may result in a one-year survival of 90%.7
A CT scan is the first choice for patients with a high suspicion. In acutely ill patients, delays in imaging may adversely affect patient care. Emergency surgery is indicated for type A aortic dissection. A type B dissection can be medically treated unless there is a complication or haemodynamic instability. In conclusion, neurological symptoms resulting from cerebral hypoperfusion and peripheral nerve dysfunction are alarming symptoms in a patient with chest pain. As soon as an aortic dissection is suspected immediate CT angiography is warranted, as early recognition of an aortic dissection type A is of great importance in view of the high mortality.
DISCLOSURES
The authors declare no conflicts of interest.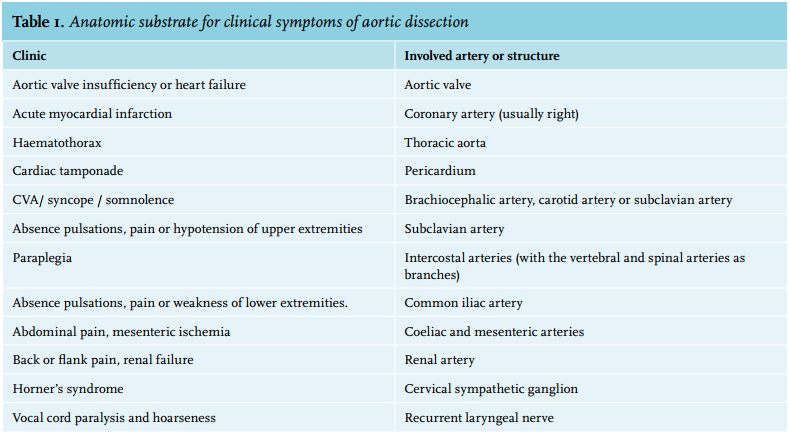
REFERENCES