KEYWORDS
Immunotherapy, SCIT, SLIT
INTRODUCTION
Immunotherapy with inhalation allergens is over 100 years old. The treatment is indicated for patients with birch pollen, grass pollen, house dust mite or cat dander allergy. The therapy induces allergen-specific immune tolerance for inhalation allergic patients and leads to a reduction of allergic symptoms in patients with rhinitis, conjunctivitis and allergic asthma. Immunotherapy is the only available effective treatment to target the disease instead of the symptoms. Whether immunotherapy is prescribed depends on the severity of symptoms, the effect of elimination measures, or medication and the desire of the patient to stop long-term pharmacological treatment. Currently, immunotherapy can be given either subcutaneously (SCIT) or sublingually (SLIT). Grass pollen has been registered for subcutaneous and sublingual administration, whereas birch pollen, house dust mite and cat dander have been registered for subcutaneous use only. Allergens are administered subcutaneously under medical supervision. The therapy has a build-up phase with, in general, weekly injections with an increasing concentration of the allergen. The duration of this build-up phase depends on the frequency of injections and ranges from 3-6 months. The build-up phase is followed by monthly maintenance injections for 3-5 years. Another option is to use an accelerated schedule (rush immunotherapy) for the build-up phase. This approach shortens the build-up phase substantially. A series of injections is administered in one visit. SLIT uses sublingual administration of drops or tablets under the tongue and is usually taken at home, except for the first dose. The safety profiles of SCIT when using the conventional schedule or the rush schedule are comparable. The safety profile of SLIT is superior to SCIT. Which route of immunotherapy is used depends on several factors such as vaccine availability, patient characteristics, cost, and physician and patient preferences.1,2
MECHANISM
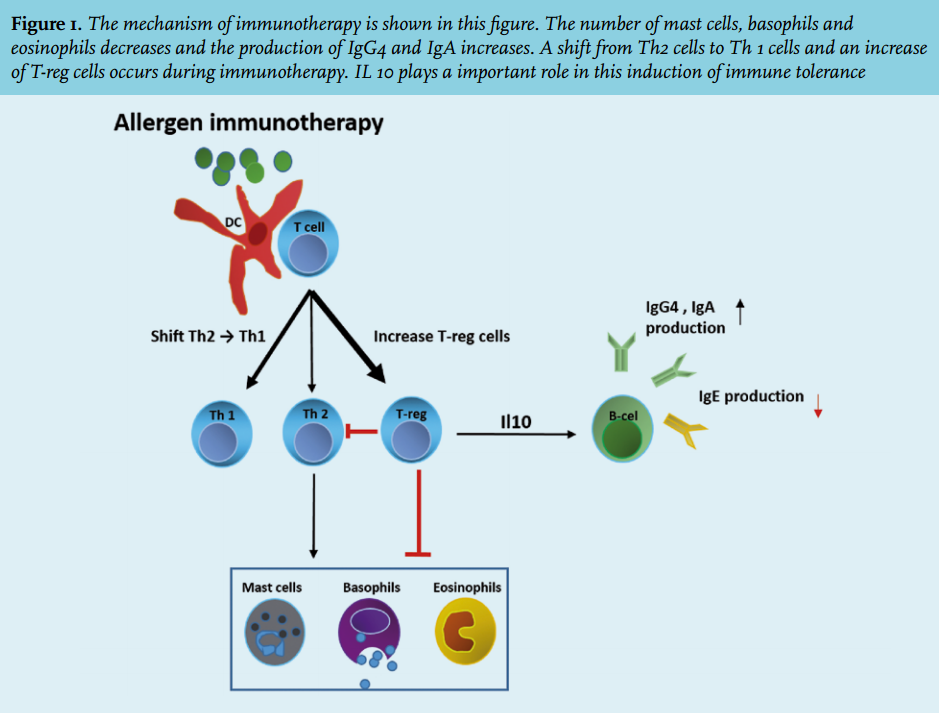
The mechanisms of allergen-specific immune response are complex and not fully understood. For this response, an early and a late phase can be distinguished. In the early phase of immunotherapy a decrease occurs in the number of tissue mast cells, eosinophils and basophils along with a reduction in mediator release.3 Basophil decrease is caused by up-regulation of H2 receptors, which causes inhibition of FcεRI-mediated release of histamine and other mediators. Also an increase of IgG4 and IgA synthesis is observed in the early phase of immunotherapy.4 IgG4 blocks the interaction between IgE and the allergen and the presentation of the allergen to T cells. In the late phase, after one to several months of immunotherapy, a shift occurs from Th2 to Th1 cells, as well as an increase in the number and function of two types of T-regulatory cells (T-reg) cells.3 The two types of T-reg cells are the natural T-reg (nT-reg) cells and inducible T-reg (iT-reg) cells. iT-reg cells are IL-10 secreting cells derived from naïve CD4+ T lymphocytes and are an important factor in peripheral tolerance induction.5,6 Il-10 inhibits the production of IgE, enhances IgG4 and is directly involved in the suppression of allergen-specific T-effector cells.7 nT-reg cells (CD4+, CD25+ and FOXP3+ (Forkhead box protein 3)) originate from the thymus and show a corresponding function to the iT-reg cells.8 nT-reg cells express high levels of IL-10 and TGF-beta.9 T-reg cells induce IL-10 secreting dendritic cells. These dendritic cells play a role in the activation and differentiation of T-cells into different subtypes. These are able to cause inflammatory response or immune tolerance depending on their maturity stage.10 iT-reg cells induce suppression of IgE production by effector B-cells. Recently, IL-10 secreting B-cells have been detected in venom-allergic patients after immunotherapy.11 IL-10 secreting natural killer cells have also been reported to play a role in the immune tolerance by antigen-specific T-cell suppression and via a decrease in IgE production. However, more research is needed to reveal their specific role.12 All these immunological effects, i.e. decrease in the number of tissue mast cells, eosinophils and basophils, an increase of IgG4 and IgA synthesis, a shift from Th2 to Th1 cells and an increase in the number and function of IL-10 producing T-reg cells, may contribute to long-term immune tolerance and to a change in the immune system (figure 1). The immunological mechanisms in SCIT and SLIT are considered to be identical.9
EVIDENCE FOR EFFICACY AND SAFETY OF SCIT AND SLIT
Pollen
Many studies have been performed in patients with a seasonal allergy on the efficacy of SCIT and SLIT. Three meta-analysis on this topic have appeared (table 1).
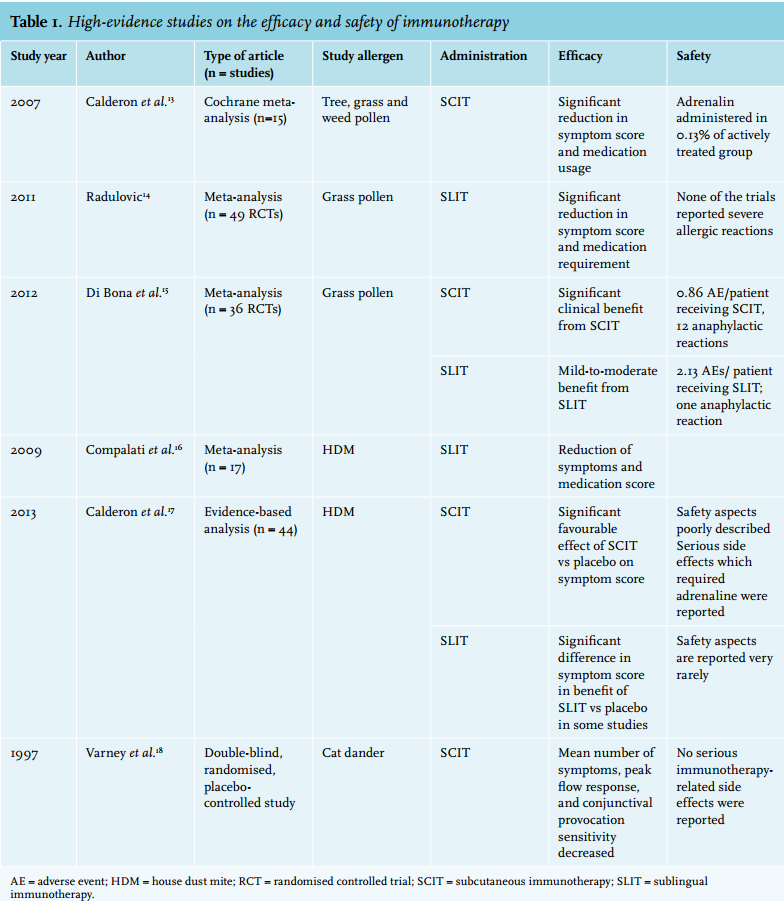
The Cochrane meta-analysis of Calderon et al. (2007) evaluated the safety and efficacy of allergen (tree, grass and weed) SCIT for patients with seasonal allergic rhinitis.13 In the symptom score meta-analysis 15 studies (n = 597 immunotherapy, n = 466 placebo) and in the medication score meta-analysis 13 studies (n = 549 immunotherapy, n = 414 placebo) were included. The authors conclude that a significant reduction in symptom score and medication usage can be achieved with immunotherapy. With regard to the safety aspects of this treatment, adrenaline was administered to only 0.13 % of the actively treated patients to cope with adverse events due to the immunotherapy.
The publication by Radulovic et al. (2011) is a systematic review on the efficiency and safety of SLIT.14 A total of 49 RCTs were used for the meta-analysis to evaluate the effect on symptom score (n= 2333 immunotherapy, 2256 placebo) and 38 RCTs (n= 1737 immunotherapy, 1642 placebo) to evaluate the effect on medication score. A significant reduction in symptom score and medication requirements was measured in the actively treated group compared with the placebo group. Severe systemic reactions such as anaphylaxis were not reported in any of these trials. Grazax® and oralair® are used for SLIT therapy in clinical practice since they were registered in Europe in 2006 and 2008, respectively.
The meta-analysis by Di Bona et al. (2012) has demonstrated the effect of grass pollen SCIT and SLIT on symptom score and medication score in 36 RCTs (immunotherapy n= 3014, placebo n = 2768).15 This study evaluated the standardised mean difference between SLIT, SCIT and placebo: there appears to be a significant clinical benefit for patients treated with SCIT and a mild-to-moderate benefit for patients treated with SLIT, both compared with placebo. Data on medication score have been analysed for 20 SLIT RCTs and 11 SCIT RCTs. These analyses showed a significantly better pooled mean estimation of treatment with SLIT and SCIT on the medication score compared with placebo. This study reported a total of 960 adverse events (AEs) due to the immunotherapy (0.86 AEs/patient for SCIT and 2.13 AEs/ patient for SLIT.) Paradoxically, the total number of AEs reported was higher in the SLIT group compared with SCIT group. However, these AEs varied from mild to severe and in total 12 anaphylactic reactions were reported for SCIT-treated patients and one for SLIT-treated patients. In summary, SCIT and SLIT generally achieve a reduction in symptom score and medication usage, but these treatments are not without local and systemic side effects. SCIT has been found effective and safe for birch pollen and grass pollen sensitised patients, whereas SLIT was only effective and safe for grass pollen sensitised patients.
House dust mites
Only a few meta-analyses have been performed on the effectiveness of house dust mite immunotherapy.
First, Compalati et al. (2009) performed a meta-analysis on the efficacy and safety of house mite dust SLIT in allergic rhinitis patients and allergic asthma patients.16 The data from eight of the 12 selected RCTs (n = 382 allergic rhinitis patients and n =476 allergic asthma patients) in allergic rhinitis patients were included in this meta-analysis, revealing a reduction of symptoms and medication score. Similar results have been found with allergic asthma patients, based on nine out of the 12 selected RCTs. These led the authors to conclude that there is promising evidence of efficacy of house dust mite SLIT for patients with allergic rhinitis and allergic asthma, but more high-quality studies are required to substantiate this. Another study was initiated as an evidence-based analysis of house dust mite allergen SLIT and SCIT for allergic asthma and allergic rhinitis patients.17 Nine out of 19 selected studies on SCIT (n = between 22 and 132 randomised participants per study) in patients with allergic asthma were found to reveal a significant difference in mean ± SD symptom score for symptom-related parameters. Unfortunately, the safety aspects were rather poorly described in these studies: nearly all serious side effects, which required adrenaline, were reported to occur during the rush dosing phase. Only two of the 14 selected studies (n = between 15 and 465 randomised participants per study) on SLIT in allergic asthma patients demonstrated a significantly better symptom score of SLIT over placebo. Safety aspects were scarcely reported in these studies. However, a few studies have specifically mentioned that no adverse events occurred. Three out of seven studies (n = between 32 and 145 randomised participants per study) on SCIT in allergic rhinitis patients reported a significantly favourable effect of SCIT versus placebo on the symptom score. The quality of safety reporting was low in most of these studies. However, anaphylactic reactions were reported in only one study. Two out of 15 studies (n = between 15 and 257 randomised participants per study) on SLIT in allergic rhinitis patients showed significant benefit of SLIT versus placebo on symptom score. The conclusion was that there were too many shortcomings in primary and secondary efficiency criteria in all of the considered studies to allow a solid meta-analysis on the efficiency of house mite dust immunotherapy. However, they were able to establish statistically that SCIT shows a significantly favourable effect compared with SLIT and placebo. The safety aspects were described only moderately. No serious AEs due to the immunotherapy were reported in the actively treated group.17
Cat dander
To our knowledge, the only published study on the effectiveness of cat immunotherapy was performed by Varney et al. 18 This is a double-blind, randomised, placebocontrolled study with 28 cat allergic patients, investigating the efficacy of immunotherapy with standardised cat dander extract. This study established that immunotherapy with standardised cat dander is an effective treatment for cat allergic patients. No serious immunotherapy-related side effects were reported in this study.
In conclusion, the efficacy and safety of pollen, house dust mite and cat dander SCIT and SLIT have been investigated in many trials, meta-analyses and reviews and are implemented in clinical practice to treat therapyresistant patients, because of the good safety profile and effectiveness in most patients.
Prevention
There is evidence that immunotherapy can prevent the development of asthma and new sensitisations. The first prospective long-term follow-up study on this topic is the Preventive Allergy Treatment (PAT) study.19 Children with seasonal rhinoconjunctivitis (n = 250) were selected from three paediatric allergy centres and randomised into a group receiving grass and/or birch pollen specific immunotherapy (SIT) for three years and an open placebo group. The SIT group showed significantly fewer asthma symptoms and improved results of methacholine bronchial provocation testing after three years compared with the placebo group. The subsequent follow-up of the PAT study performed by Jacobsen et al. evaluated the even longer-term clinical effect and the preventive effect on developing asthma in 147 patients treated with grass and/or birch pollen SIT.20 A significant improvement of rhinoconjunctivitis and conjunctival sensitivity persisted seven years after a three-year SIT treatment (ten-year follow-up.) Also significantly less patients in the SIT group developed asthma evaluated by clinical symptoms after ten years. The retrospective study by Purello-D’Ambrosio et al. based on 8396 mono-sensitised patients, treated with immunotherapy or pharmacotherapy (groups are well balanced in numbers), demonstrated that 27% of the patients treated with immunotherapy were poly-sensitised after seven years and even 77% of the pharmacological group. Asthmatic patients were more prone to develop poly-sensitisation than rhinitis patients.21
New developments
Immunotherapy in its current form is not without side effects and patient adherence still remains a problem. Immunotherapy is cost-effective for both SCIT and SLIT compared with symptomatic therapy from around six years (threshold of £20,000-30,000 per quality-adjusted life years, QALY),22 but these costs remain significant. Furthermore, there are still problems with the efficacy. The extrinsic factors that might play a role in the effectiveness/ ineffectiveness of immunotherapy are the doses of the allergen used, the allergens present in the preparation, the route of administration, the indication for which it is prescribed and therapy adherence. It is not clear which intrinsic factors in the immune mechanisms are important per patient for establishing whether the immunotherapy actually translates into clinical tolerance/improvement of symptoms or failure of immunotherapy non-responders. The costs, ineffectiveness of immunotherapy in some patients and the safety aspects stimulate researchers to develop new immunotherapy strategies. Targets are numerous: novel route of administration, combined treatment with immune response modifiers, fusion with immune response modifiers and allergen coupled to adjuvants. Other targets are reconstruction of natural extracts with multiple recombinant allergens (allergens produced by recombinant DNA technology) or with modified allergens (altered composition of allergens) or the use of peptides of allergens as extracts (table 2).2,23
Novel routes are, for example, intralymphatic or epicutaneous administration, which have both already scored in efficiency and safety in clinical trials.24-27 Pretreatment patients with anti-IgE omalizumab before immunotherapy, and an optional period during immunotherapy, caused a significant decrease of systemic allergic reactions and a decrease in the need for rescue medication to suppress symptoms.28,29 The fusion of allergens with immune response modifiers should ensure a more effective form of immunotherapy with fewer side effects. The fusion with human Fcy receptors inhibits basophil and mast cell degranulation by cross-linking of Fcy and FcεRI receptors.30 The major cat allergen Felis domesticus 1 (Fel d 1) was fused to TAT peptide and to a part of the human variant chain, creating a transporter (MAT) vaccine (MAT-Fel d 1.) MAT-Fel d 1 on intralymphatic administration has proved to be safe and effective for immunomodulation.26 Allergens are also coupled to GpG oligonucleotide, virus-like particles, monophosphoryl lipid A, carbohydrate-based particles and hepatitis B PreS to cause a shift in immune reaction, to increase the efficiency or to decrease the side effects of the immunotherapy. These forms of immunotherapy show promising results in humans and mouse models.23 The efficacy and safety of immunotherapy with a mixture of grass pollen components (allergenic proteins in allergens) to allergic patients demonstrated a strong IgG response.31
The idea behind immunotherapy with modified allergens is to induce T-cell tolerance and to avoid IgE-related side effects. The allergens can be administered in allergen fragments, fusions, hybrids or chimeras.32 Fel d 1-derived cat peptides have been proven safe and well tolerated by patients with a cat allergy.33
In summary, these are approached along novel routes including improved administration, combined treatment with immune response modifiers, fusion with immune response modifiers, allergen coupled to adjuvants and reconstruction of natural extracts with multiple recombinant allergens or with modified allergens. These are promising new developments, but more research is required to implement these in clinical practice. 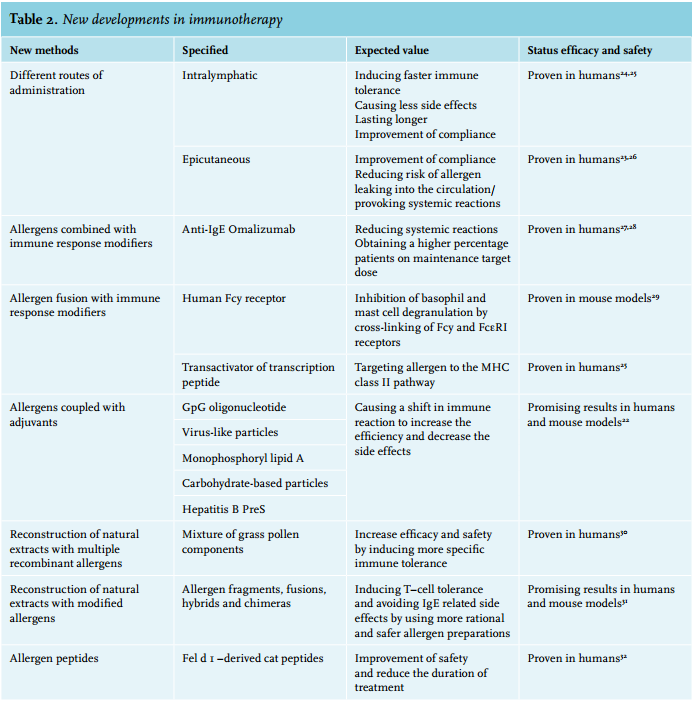
CONCLUSION
Allergen immunotherapy has been prescribed now over a long period for birch pollen, grass pollen, house dust mite and cat allergic patients. The efficacy and safety have been proven in many years of practice, despite the fact that the immunological reactions are not fully understood. This treatment has a lot of benefits for patients, such as decrease of symptoms, decrease of medication usage, long-term effect and prevention of new sensitisation or asthma. Therefore, immunotherapy should be prescribed more often as therapeutic option, in particular if you take the high prevalence of airway allergy into consideration. However, the development of new immunotherapy methods will continue to improve the prolonged period of the treatment, the side effects and the ineffectiveness for some patients. Despite the fact that the results of the new developments are promising, more research is needed to implement these new technics in clinical practice.
DISCLOSURES
The authors declare no conflicts of interest.
REFERENCES