KEYWORDS
Atrophic gastritis, dyspepsia, dysplasia, intestinal metaplasia, nodular gastritis
INTRODUCTION
Gastric mucosal nodularity is an endoscopic finding occasionally seen in general practice. There is no consensus about the definite endoscopic definition of nodular gastritis and its clinical classification as an acute or chronic lesion.1-10 The term endoscopic nodular gastritis is generally used as a miliary nodular appearance on the gastric mucosa on endoscopy.1,2 Various terms such as antral nodularity,3-7 antral nodular hyperplasia,8 nodular antritis,9 and micronodular gastritis10 have been used for endoscopic nodular gastritis.
Endoscopic nodular gastritis is more common in areas with high prevalence of Helicobacter pylori infection. Many studies have shown that the prevalence of some types of gastritis such as endoscopic nodular gastritis is higher in H. pylori-positive cases in comparison with H. pylori-negatives.6,7,10-12 However, some reports did not show any significant correlation between endoscopic nodular gastritis and H. pylori positivity.2 There is also no consensus about the association of endoscopic nodular gastritis with histopathological changes such as histological premalignant lesions.1,2,6,7,9,12-14 For example although some studies has been revealed the association of endoscopic nodular gastritis and lymphoid follicle formation,6,7,9 other studies did not show any correlation between them.1,2,12 Association between endoscopic nodular gastritis and premalignant or malignant conditions as a pathological change is also not clear and there are a few published studies which have described this controversial association.2,13-17
Dyspepsia, which is a common heterogeneous group of abdominal symptoms, is used to characterise abdominal pain or discomfort centred in the epigastrium. Although the major cause of dyspepsia is a functional disorder, gastric cancer can also present with dyspepsia.18,19 Gastric cancer, which is a major public health problem, is one of the most common causes of cancer-related mortality.20,21 Mucosal chronic atrophic gastritis, complete or incomplete intestinal metaplasia, and gastric dysplasia are histological premalignant lesions.22-24 A multistep cascade of precursors (superficial gastritis–atrophic gastritis– intestinal metaplasia–gastric dysplasia–carcinoma sequence) has been recognised for the development of the intestinal type of gastric cancer.20
Atrophic gastritis is characterised by the severe decrease or disappearance of typical gastric glands with the evidence of extensive inflammation.25,26
Intestinal metaplasia is a relatively frequent histological premalignant lesion and is defined as the replacement of the glandular gastric epithelium by mucosa that resembles the intestinal type cells. Complete intestinal metaplasia resembles a small intestinal epithelium phenotype with absorptive cells, Paneth cells, goblet cells, and a variety of endocrine cells. Incomplete intestinal metaplasia is diagnosed when the epithelium resembles the colonic phenotype with multiple, irregular mucin droplets of variable size in the cytoplasm and absence of absorptive cells.25,27
Gastric dysplasia is characterised by the decrease of cytoplasmic mucin, cellular pleomorphism, nuclear hyperchromatism, increased nuclear-cytoplasmic ratio, increased mitotic activity, and glandular disarray.28
Because there is no general consensus on the association of endoscopic nodular gastritis and histological premalignant lesions (e.g. atrophic gastritis, intestinal metaplasia, and dysplasia), we designed this study to find a possible connection. In this study a range of histological premalignant lesions were comparatively analysed between two groups of Iranian adult dyspeptic patients with and without endoscopic nodular gastritis.
METHODS
After obtaining the approval of the university ethical committee (93-01-13-8145) as well as written informed consent from each patient or his or her legal guardian in accordance with the Helsinki Declaration, all the consecutive rural patients with dyspepsia were recruited in this cross-sectional study between November 2011 and January 2014.
Diagnosis of dyspepsia was based on clinical findings. Endoscopic nodular gastritis was defined as a miliary nodular appearance on the antrum and/or body of gastric mucosa on endoscopy. All the endoscopic procedures were performed by an expert gastroenterologist with a high resolution white light endoscope. The biopsies were taken from all of the included patients with endoscopic nodular gastritis and normal endoscopy. Two biopsies from the antrum and two biopsies from the body were obtained from all patients with endoscopic nodular gastritis and the control group. Biopsy samples were fixed in 10% formalin and transferred to the lab in the appropriate condition. The staining with haematoxylin and eosin stain and Giemsa stain was done for histological detection of H. pylori. The samples were examined for the presence of atrophic gastritis, complete or incomplete intestinal metaplasia, and dysplasia by two expert pathologists who were blinded for the endoscopic findings.
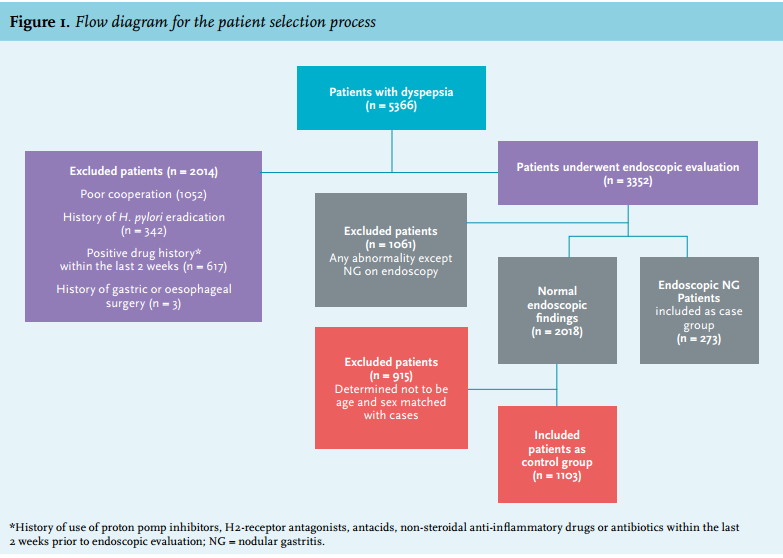
The patients were excluded from the study if one of the following conditions existed: (a) patients in a poor cooperation; (b) history of H. pylori eradication; (c) history of use of proton pomp inhibitors, H2-receptor antagonists, antacids, non-steroidal anti-inflammatory drugs or antibiotics within the last two weeks prior to endoscopic evaluation; (d) history of gastric or oesophageal surgery; (e) any abnormality except nodular gastritis on endoscopy.
Statistical analysis
Comparisons between the two groups were analysed by using the chi-square test for categorical variables and by t-test for continuous variables. Two-sided values of p < 0.05 were considered statistically significant. Statistical analyses were performed with SPSS 15.0. Odds of premalignant lesions were analysed by using logistic regression with adjustment by sex and age.
RESULTS
From 5366 evaluated patients, a total of 273 patients with endoscopic nodular gastritis and 1103 precipitants with normal endoscopic findings as a control group were evaluated (figure 1).
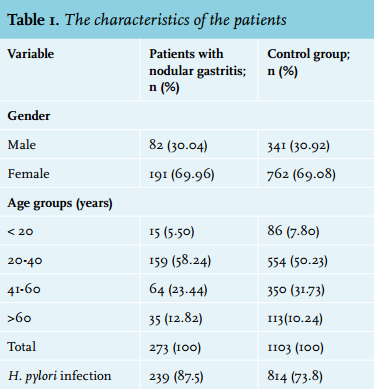
The mean age (SD) of patients with endoscopic nodular gastritis and the control group was 38.19±16.23 and 39.21 ±15.62 years, respectively. Of the patients with endoscopic nodular gastritis, 58.24% were in the age group 20-40 years and the majority of them (69.96) were woman. Histological H. pylori infection was detected in 87.5% of patients with endoscopic nodular gastritis, whereas 73.8% of the control group were H. pylori positive. The prevalence of H. pylori infection was significantly higher in patients with endoscopic nodular gastritis than in the control group (OR 2.31; 95% CI 1.72-3.70; p < 0.001) (table 1). In the H. pylori-positive subgroup the prevalence of premalignant lesions in patients with nodular gastritis was significantly higher than in the normal endoscopy group (16.3% vs. 7.9%, p = 0.000).
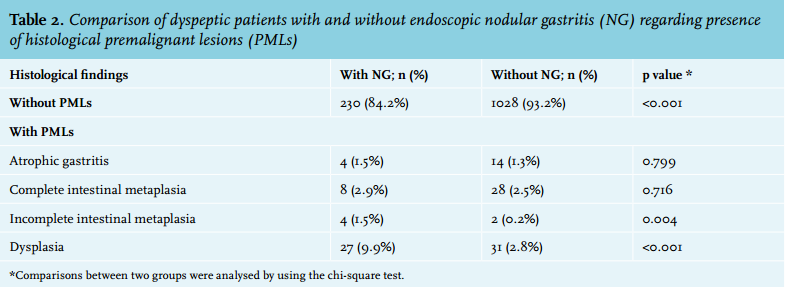
On histopathological examination, the rates of atrophic gastritis in patients with endoscopic nodular gastritis and the control group were 1.5% (4/273) and 1.3% (14/1103), respectively. Intestinal metaplasia (complete or incomplete) was detected in 4.4% of patients with endoscopic nodular gastritis but only 2.7% of the control group had evidence of intestinal metaplasia. Of the patients with endoscopic nodular gastritis, 2.9% and 1.5% had complete intestinal metaplasia and incomplete intestinal metaplasia, respectively. Of the control group 2.5% and 0.2% had complete intestinal metaplasia and incomplete intestinal metaplasia, respectively. The rates of dysplasia in patients with endoscopic nodular gastritis and control group were 9.9% and 2.8%, respectively (table 2).
The prevalence of dysplasia (OR 3.98; 95% CI 2.27-6.66; p < 0.001) and incomplete intestinal metaplasia (OR 8.63; 95% CI 1.47-45.00; p = 0.004) in patients with endoscopic nodular gastritis were significantly higher than the control group. On the other hand, atrophic gastritis (OR 1.18; 95% CI 0.38-3.60; p = 0.799) and complete intestinal metaplasia (OR 1.21; 95% CI 0.51-2.57; p = 0.716) were more frequent in patients with endoscopic nodular gastritis than in the control group, but the difference was not significant (table 2).
DISCUSSION
There are a few published studies that describe the association of histological premalignant lesions with endoscopic nodular gastritis. As far as we know, this study is the first report on a population of adult patients with dyspepsia in which a range of histological premalignant lesions were comparatively analysed between two groups of patients with and without endoscopic nodular gastritis. In a case-control study Sokmensuer et al. 2 showed that intraepithelial lymphocytosis was significantly more prominent in patients with nodular gastritis and may contribute to nodule formation. In this study lymphoid hyperplasia was not more frequent in patients with nodular gastritis and the prevalence of H. pylori infection was not significantly higher than patients without endoscopic nodular gastritis. They showed that gastric dysplasia and complete metaplasia were more frequent in patients with nodular gastritis. They proposed that endoscopic nodular gastritis should be biopsied for the possibility of dysplasia and intestinal metaplasia.
A case-control study in dyspeptic patients in Kuwait showed that the prevalence of nodular gastritis was significantly higher in young women. They also showed that glandular atrophy (nodular gastritis 6.3%, controls 0%; p = 0.492) and intestinal metaplasia (nodular gastritis 3.1%, controls 0%; p = 1) were more frequent in patients with endoscopic nodular gastritis.16
In a case-control study, Dwivedi et al. 17 showed that atrophy (casess 25%, controls 5%; p < 0.05) and intestinal metaplasia (case 12.5%, controls 0%) were more frequent in patients with nodular gastritis. The mucosal inflammation was present in 93% of patients with nodular gastritis and 37.5% of the control group.
In a case-control study by Miyamoto et al. 13 nodular gastritis was predominantly seen in young women. The prevalence of lymphoid follicles was significantly higher in patients with nodular gastritis than in the control group. Gastric cancer was seen in 1% of the patients with nodular gastritis. They concluded that H. pylori eradication therapy should be considered for all patients with nodular gastritis for decreasing symptoms, risk of peptic ulcer disease, and possibly gastric cancer.
In another study, Nakashima et al. 29 showed that atrophy and intestinal metaplasia are rare but activity and chronic inflammation are severe in patients with nodular gastritis. Nodular gastritis was predominantly seen in the women, which tended to decrease in prevalence with the increase of patient age. All the patients with nodular gastritis were H. pylori positive.
A case-control study in Turkish adults showed that lymphoid follicle was not more prevalent in patients with nodular gastritis than in the control group. The prevalence of H. pylori was 65.4% and 59.2% among the patients with nodular gastritis and the control group, respectively.1 A cross-sectional study by Loffeld30 in 305 consecutive patients with macroscopic signs of gastritis showed that the only sign with a high positive predictive value for H. pylori infection is antral nodularity.
In our series, similar to many other studies, the prevalence of H. pylori infection was significantly higher in patients with endoscopic nodular gastritis than in the control group (p < 0.001).1,6,7,10-12,15,29-32 This result shows that H. pylori infection can be considered an effective factor to the formation of endoscopic nodular gastritis.
Most of our patients with endoscopic nodular gastritis were in the 3th and 4th decade of life (table 1) with a predominance for the female sex. These results, which are similar to other studies, showed that the prevalence of endoscopic nodular gastritis was more common in young women.13,15,16,29
In this study atrophic gastritis, intestinal metaplasia, and dysplasia were more frequent in patients with endoscopic nodular gastritis. The prevalence of incomplete intestinal metaplasia (p = 0.004) and gastric dysplasia (p < 0.001) in patients with endoscopic nodular gastritis was significantly higher than in the control group. In this study, similar to some other reports, the prevalence of histological premalignant lesions was more frequent in patients with endoscopic nodular gastritis but at a more significant level (table 2).2,16,17 These results show that endoscopic nodular gastritis may be considered a possible risk factor for the formation of histological premalignant lesions.
In this study, and some of the other reports, the H. pylori infection showed a significant increase in the endoscopic nodular gastritis,1,6,7,10-12,15,29-32 on the other hand in many studies, the high prevalence of H. pylori infection in patients with histological premalignant lesions and cancer is described.33,34 So H. pylori infection can be one of the possible mechanisms of increase in histological premalignant lesions in individuals with endoscopic nodular gastritis. Interestingly according to our results the prevalence of premalignant lesions in endoscopic nodular gastritis was also significantly higher than normal endoscopy in the H. pylori-positive subgroup (p = 0.000), which is in favour of a possible role for nodular gastritis in premalignant lesions.
Our study had some limitations. First, this was a single-centre study. Second, we evaluated only symptomatic patients. Third, we evaluated only rural participants. Fourth, we confirmed H. pylori infection with only one method.
In conclusion, we propose that incomplete intestinal metaplasia, gastric dysplasia and H. pylori infection is significantly more frequent in patients with endoscopic nodular gastritis. However, more studies should be done to the clarify the association between endoscopic nodular gastritis and histological premalignant lesions. Because of these significant correlations, we recommend that endoscopic nodular gastritis could be biopsied in all patients for the possibility of histological premalignant lesions such as intestinal metaplasia and dysplasia in addition to H. pylori infection.
DISCLOSURES
The authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES