KEYWORDS
Ageing, elderly, evidence-based medicine, clinical studies, randomized controlled trials
INTRODUCTION
Older people are becoming a more prominent proportion of modern Western societies, both in absolute and relative terms. This is the result of increasing life expectancy, decreasing fecundity rates, and specific changes in population demographics, such as the baby boom after the Second World War. In Europe the number of inhabitants aged 65 years is 88 million (17% of total population) today and is projected to increase to 157 million (30%) in 2060 (Eurostat Statistics). As a result, a sharp increase in health care demand by older people is foreseen in the near future, which will affect nearly all domains of medicine.1 Evidence-based medicine (EBM) is the hallmark of modern medicine and aims to integrate the individual patient’s situation, scientific evidence and the physician’s experience and expertise in the process of clinical decisionmaking.2 This review aims 1) to assess how the elements that constitute EBM are systematically different in older patients and how these differences affect the degree of EBM in older patients and 2) to propose strategies how to improve EBM in older patients.
CURRENT SITUATION
To come to strategies to improve EBM for older patients, we will first define the components of EBM. Then we explore how the ageing process affects the physiology and function of the older body, how these physiological changes and altered patient situation affect the balance between cost and benefits of treatment decisions and how these aspects are addressed in current scientific evidence.
Evidence-based medicine
The term evidence-based medicine was introduced in the early 1990s and has been defined as the ‘conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients’.2 The essence of EBM is the complementary role of scientific evidence, physicians experience and expertise, and the individual patient’s situation and preferences in clinical decision-making. In clinical practice these components cannot be assessed entirely separately. For instance, the doctor’s opinion is strongly based on his assessment and interpretation of relevant literature and of the patient’s situation.
Consequences of ageing
Ageing results from the accumulation of damage to the body due to internal and external stressors.3 Accumulated macromolecular damage affects the functioning of cells and tissues, which compromises the body’s capacity to maintain homeostasis thus causing an inherent increase in the chance of disease and death.3 This definition of ageing mirrors our clinical observation of increased burden of disease and higher chance of mortality with increasing age in our patients.4 There are several inherent consequences of the ageing process that make the older patient fundamentally different from the younger patient. First, compared with younger ages physiology in the older body is different.5 Second, there is a higher degree of multimorbidity and polypharmacy.6 Third, in the older patient a somatic disease often affects the intricate relationship between somatic disease and physical, psychological and social functioning.6 All three aspects fundamentally change the way treatment strategies and scientific evidence should be assessed. These three aspects are elaborated upon below.
First, physiology of the older body is different than at younger ages. Well-known factors associated with ageing are a decreased renal function, liver function and altered body composition, which affect metabolism and clearance of pharmacotherapeutics.7 Such changes necessitate careful dosing of medications in older patients, especially since there is a concomitant risk of drug-drug interactions in patients with polypharmacy.8 However, besides these pharmacokinetic and pharmadynamic changes, observational findings concerning everyday clinical problems exemplify that the older patient differs from the younger patient. For instance, in the oldest old, having a high blood pressure is associated with longer survival,9 which contradicts the common paradigm that in middle age, hypertension is a well-established risk factor for cardiovascular disease and mortality. Similar paradoxical findings of association with better survival have been made for high levels of cholesterol and subclinical hypothyroidism in those over 85 years.10,11 Likely explanations for these findings include the fact that in old age biology may be different than at younger ages. For instance, in an 85-year-old the vasculature exhibits a higher degree of stiffness, therefore requiring a higher blood pressure to maintain adequate perfusion of organs, and high blood pressure may thus be interpreted as an adequate adaptive response of the body to counteract age-related changes to the vasculature.12
Second, with increasing age the prevalence of disease increases, resulting in a high proportion of elderly suffering from multiple chronic diseases.13 Previous studies show that 55-98% of the elderly have two or more chronic diseases (i.e. multimorbidity).13 Applying clinical guidelines for single diseases to older patients with multimorbidity leads to polypharmacy.14 Furthermore, in those with polypharmacy, the risk of negative outcomes is increased. In one study from the Netherlands, it was estimated that 6% of all hospital admissions was related to negative effects of medication use, and that half of these were preventable.15 It is very likely, that among these patients admitted to hospital, there is an overrepresentation of frail elderly people with multimorbidity and polypharmacy. Furthermore, Opondo and colleagues showed that one in five medications given to elderly patients in primary care is inappropriate.16 Some clinical trial evidence suggests short-term benefit or at least lack of harm of medication withdrawal.17
Third, in older patients the intricate relationship between the four axes somatic disease and physical, psychological and social functioning is more apparent than at younger ages.6 Physical function includes the level of physical activity and the ability to perform activities of daily living, such as dressing, cooking, bathing and doing the groceries. Psychological function includes cognitive performance, apathy and depression. Social functioning is determined by the presence of a spouse, outdoor social activities with friends and the level of support provided by children and the social activity of the patient. In case of severe illness in younger patients, such as oncology patients, it is already custom to measure functional capacity as a marker of patient vulnerability to assess whether the patient can endure intense treatments such as chemotherapy.18 In older patients the intricate relationship is also present when disease is less severe, as multimorbidity and polypharmacy often affect multiple axes. Together, the four axes that characterise the older patient, may mark the extent of increased vulnerability, and may therefore serve as determinants of disease or treatment outcome. However, the four axes could also be endpoints: for the older patient physical, psychological and social function largely determine the level of dependence and quality of life and may be affected by disease and treatment.19 Thorough assessment of all axes is critical both in clinical studies of older patients as well as when treating an individual older patient.
In conclusion, physiology of the older body is different than at younger ages, there is a high degree of multimorbidity and polypharmacy and in the older patient physical, psychological and social function importantly determine disease and treatment outcome. Altogether, these consequences of the ageing process make the elderly patient more vulnerable for diseases and disease complications, affecting the physical, psychological and social function in the older patient. Treatment outcomes are strongly affected by these aspects, as they affect the balance between ‘costs’ and ‘benefits’ of treatment in the older patients.
Balance between ‘costs’ and ‘benefits’
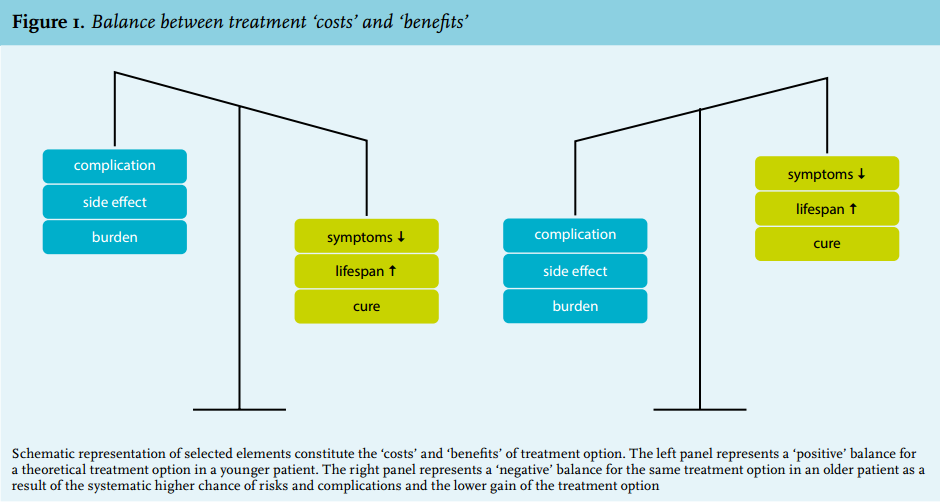
The essence of making treatment decisions is the assessment of the balance of ‘costs’ and ‘benefits’ between different treatment strategies (figure 1, left panel). Positive treatment effects or ‘benefits’ (such as cure, symptom relief or survival) should outweigh the negative consequences or ‘costs’ (such as burden of treatment, risk of complications or side effects). When compared with younger age groups, the negative effects (‘costs’) and positive effects (‘benefits’) of treatment are likely to be different in older patients. In general, the ‘costs’ will be higher and the ‘benefits’ lower (figure 1, right panel). Ageing leads to decreased physiological function, decreased capacity of the body to respond to perturbations and hence increased in vulnerability of the patient.3 Therefore, older patients have higher risks of complications of medication, surgery and other interventions. For instance, inactivation and immobilisation result in loss of muscle mass, which in older age recovers more slowly than at younger ages and is a risk factor in its own right, for instance, for falls.20 This may lead to long rehabilitation periods, functional decline and loss of independence.21 In the perioperative phase older patients have an increased risk of delirium, which in turn is a risk factor for cognitive and functional decline in the postoperative period.22 Furthermore, as pharmacodynamic and pharmacokinetics change in older age there is a higher chance of drug-drug interaction especially in the presence of polypharmacy. A higher dosage above the therapeutic range can lead to more side effects or dosing below the therapeutic range, leading eventually to undertreatment.7
On the other hand, expected benefits are – again in general – lower. With a shorter remaining life expectancy in older age, identical relative benefits on life expectancy are much smaller in absolute terms in older age. For instance, a 10% reduction in ten-year mortality risk is very relevant at the age of 40 years when life expectancy is over four decades or more, but less so at the age of 85 years when remaining life expectancy may be no more than five years based on high calendar age alone. Furthermore, when functional capacity in older age is limited by a combination of factors, such as neurological disorders, sarcopenia, osteoarthritis, treatment of only one of these factors will result in a smaller restoration of physical function compared with an individual in whom only one pathology limits functional capacity. Arguably, the effect of treatments on endpoints is not only quantitatively different in older patients, they may also be qualitatively different. Older patients may value physical or social functioning as their most important determinant of quality.23
The degree to which this is relevant for the individual patient may vary greatly: patients of the same calendar age may be very different in biological age. Due to the large heterogeneity among older patients, generalising treatments based on calendar age may result in overtreatment of frail older patients and undertreatment of fit older patients. Overtreatment may result from automatic prescription of medications according to guidelines to patients with multimorbidity. Especially when the indications of these individual medications are not weighed against the lag time to benefit or effect on quality of life,24 it is likely that polypharmacy may occur which is detrimental to the patients rather than beneficial. On the other hand, at least in some fields such as breast cancer, patients are withheld treatments based on calendar age alone, whereas data suggest that there is undertreatment in older patients.25
In conclusion, in older age the balance of cost and benefit of any medical treatment is in general less advantageous than at younger ages. However, large inter-individual differences exist and endpoints of interest may be different in older patients.
Scientific evidence in old patients
The different physiology, the increased level of multimorbidity and polypharmacy, and the multidomain functioning of the older patient constitute different requirements for clinical studies to be relevant for older patients compared with younger patients. Such requirements include the inclusion of representative older patients (i.e. including age-related physiological changes, multimorbidity and polypharmacy), the reporting and weighing of all four geriatric axes, and the inclusion of study endpoints that are relevant for older patients, such as physical, psychological or social functioning and quality of life. Clinical studies can be categorised in different domains: aetiological, prognostic, diagnostic, or intervention studies. Here we will explore whether these requirements are met for each of the different domains.
Dedicated aetiological studies are essential in understanding how health and disease work. Numerous large cohorts exist that specifically study health and disease in older age to understand how the ageing body works.26,27,28 Typically these are observational studies, often hampering causal inference but providing testable hypotheses with respect to interventions to improve health and functioning. Aetiological studies performed in representative older patients may provide useful evidence for the treatment of older patients.
In clinical practice, several prognostic tools are being used to translate the individual patient characteristics into clinical advice. Well-known examples include the Framingham risk score for predicting cardiovascular risk,29 Euroscore to predict mortality risk for cardiothoracic surgery,30 and Adjuvant online,31 an online tool to predict effects of different treatment modalities in patients with breast cancer. However, none of these three tools function well in older patients.32,33,30 The systematic problem of these prognostic tools includes that they were not developed and validated in older populations and did not include data relevant to older patients, such as physical or cognitive function either as a prognostic factor or as outcome of treatment. There are very few clinically useful tools to assess vulnerability of the individual older patient, which carries the risk of generalisation of treatment advice. This may lead to systematic overtreatment of those who are considered fitter than they actually are and undertreatment of those who are fitter than considered generally.
Diagnosis of disease is not fundamentally different in older age compared with younger ages. However, the use of diagnostic tools may be different in several aspects. First, the a priori chances of a diagnosis may vary and hence the predictive value of a diagnostic tool may be different. For instance, the chance of an adrenal incidentaloma increases with age, but it is not always clear what the diagnostic approach or long-term follow-up should be.34 Second, the burden of diagnostic tests for the patient may be higher. The preparation for a colonoscopy is troublesome in an older patient with mobility problems, increased fall risk or cognitive disorders. The indication for a colonoscopy in such a patient should be considered in the light of the indication, but also in light of the possible finding. If an operation for a potential tumour is not possible or desired by the patient, the burden of the colonoscopy may well outbalance the potential winnings. Third, it is unclear whether ‘normal’ values in old age are similar to younger ages. In older ages average haemoglobin and renal function are both below the normal range for younger patients. Sometimes these lower values are therefore considered ‘normal for this age’. It is unclear whether this is true for all parameters. In the oldest old, for instance, haemoglobin levels below the normal limit is a common finding, but it is associated with increased risk of death.35 In conclusion, diagnostic tools may perform differently in old age and applicability for the older patient should be assessed for each diagnostic tool in each setting separately.
Randomised controlled trials (RCTs) are considered the hallmark of EBM.36 From all the different types of studies, RCTs or meta-analyses of multiple RCTs are regarded to have the highest ‘level of evidence’ and this drives clinical guidelines to formulate treatments based on the results of these RCTs or meta-analyses of multiple RCTs. However, older patients are underrepresented in clinical trials as a result of selection by eligibility criteria.37,38,39 The experimental design of randomisation reduces the chance of bias or confounding. From the researcher’s perspective, including older patients in a clinical trial when studying the effects of a new treatment modality is not always attractive. Older participants introduce a higher burden of comorbidities and a higher rate of serious events that do not relate to the treatments that are compared. This ‘competing risk’ introduces an increased rate of randomness in the occurrence of endpoints, and therefore necessitates larger sample sizes and/or longer follow-up.40 For similar reasons sometimes specific patient characteristics are required to study the effect of a drug that would result in exclusion of elderly participants from the study. For instance, to study the effects of a drug that is cleared by the kidney, a patient population may be required that does not include patients with renal failure.
These inclusion criteria often select more implicitly in favour of younger participants. For instance, having an impaired renal function, defined as a clearance of 60 cc/ min or more, is not a common finding in the oldest old, in which the average renal function is around 45 cc/ min.41 Finally, older participants are excluded for practical reasons: a trial protocol that requires participants to visit a study centre multiple times excludes older participants with mobility problems. Explicit exclusion criteria can be an upper age limit, or the exclusion of diseases (such as dementia) that are almost only seen in older adults. Notably, the reason for excluding patients based on age is not always justified when reporting the results.38 As a result of these selection criteria, the elderly are underrepresented in RCTs. For instance, in a meta-analysis of RCTs performed in patients with acute coronary syndrome, among over 70,000 patients only 12% were aged over 70 years, whereas among prevalent cases this percentage is around 43%.42 And when selection criteria made in RCTs regarding breast cancer treatment were applied to a clinical cohort of breast cancer patients, only 12% of patients could have been included.43 Evidently, the older people who did participate in the RCTs could fulfil the selection criteria and are therefore not representative for the older population in general.44 Endpoints in RCTs are often related to the incidence of disease and mortality, whereas for older patients the endpoints physical, psychological and social functioning may be considered more important.23
In conclusion, RCTs are the hallmark of evidence-based medicine, but for various reasons the elderly are systematically excluded. This leads to a quantitative underrepresentation of older adults and the older participants who are included are not representative for the general population of elderly people. Clinical guidelines are often written drawing on clinical trials in selected patients without comorbidities; therefore, external validity of these guidelines for older patients with multimorbidity is lacking. Endpoints studied by RCTs are not always relevant for older patients.
IMPROVING EBM IN OLDER PATIENTS
The level in which medicine for older patients is evidence-based can be increased by improving the contribution of each of the three elements to clinical decision-making. Below we will outline how the three elements of EBM can be improved: by systematically acknowledging the patient situation, generating more scientific evidence and increasing doctor’s expertise with respect to EBM in older patients.
Systematic acknowledgement of the patient situation
The situation of the older patient should routinely be part of clinical practice as determinants of disease or treatment outcome. This starts with the awareness of the physician of the physical, psychological and social functioning of the patient and his/her preference with respect to the treatment goal. However, routinely performing a comprehensive geriatric assessment (CGA), in which all four axes of the older patient are thoroughly investigated in all patients above a certain calendar age, is likely not feasible or efficient in all situations, as it is very elaborate. CGA has been proven not to be effective, for instance, in the acute setting.45 Furthermore, it is complex to derive specified clinical advice with respect to treatment of specific diseases from the CGA. Screening tools have been developed to assess the patient situation in a routine setting that include questionnaires assessing functional capacity, assessment of comorbidities and measurements of functional capacity (including cognitive function).46 One of the most frequently used screening tools is the ‘Fried Frailty Indicator’ which defines frailty as the co-existence of at least three out of five potential symptoms: low gait speed, weight loss, self-reported exhaustion, low grip strength or low physical activity.47 Gait speed in itself is also a robust prognostic marker for mortality risk.48 Another approach to access frailty is to consider the burden of comorbidities. The most frequently used is the Charlson comorbidity index.49 For large-scale clinical research CGA is not feasible either; rather, validated screening tools can be used. Such tools could serve as prognostics markers.46 However, such screening tools have not found their way into clinical practice on a large scale, as they have not been tested and validated in clinical studies. Further studies are warranted to first design and validate screening tools and then to implement and test them for efficacy in routine care trajectories. Innovative approaches using modern technologies, such as internet and health sensors, may facilitate studying of important parameters such as physical activity and cognition in large and heterogeneous populations.
Generating more scientific evidence
To increase the scientific underpinning of our everyday clinical practice, several measures can be taken. First, for specific diseases and guidelines, existing evidence can be assessed for validity for older patients in general and individual patients specifically. Second, more information can be obtained by using already available evidence. Given the lack of large numbers of representative older adults in individual studies, pooling data from multiple studies (preferably by pooling individual patient data) may provide interesting evidence for the older patient without the necessity of repeating such trials. Successful examples of such pooling of data are the meta-analyses of several trials, assessing the effects of newly introduced novel oral anticoagulation drugs (NOACs), showing no additional risk in the use of these agents in older patients.50 Third, more and more representative older patients should be included in clinical studies. It is impossible to replicate all RCTs performed in middle age for all individual older patients. The heterogeneity of this patient group as a result of multimorbidity would necessitate a large number of RCTs,51 which is not feasible because of financial constraints. Furthermore, performing RCTs is a greater burden for the patients.
It is, however, possible to perform clinical studies that are relevant for the older patient and contribute to a higher level of scientific evidence. Designing clinical studies for older patients requires specific measures, such as measures to ensure inclusion of representative older patients, adequate phenotyping of their physical, psychological and social functional status and studying relevant endpoints. There are guidelines on how to perform a RCT specifically in older age.52 It is, however, not feasible to repeat all clinical trials in old age. Therefore alternative study designs may be more attractive. An observation design may help to increase our understanding of the effects of the ageing process and therefore may inform treatment decisions. Studies may be tailored to overcome the unique barriers of participation of older patients.53 However, caution is warranted with respect to causal inference, which can be overcome by genetic Mendelian randomisation studies.54 When diseases are studied that are relatively rare, or when observational studies are small, pooling data in individual patient data (IPD) meta analyses can provide valuable insights.55 Because repeating all RCTs for older patients is not feasible, alternative designs for intervention studies can be considered. For instance, the stepped wedge design uses an approach in which the effect of an intervention is assessed before and after implementation in clinical practice.56 In this way, evidence can be obtained on effectiveness without the necessity to randomise individual patients. Another design is the regression discontinuity design.57 In this design patients who fulfil a certain criterion (for instance a blood pressure above 140 mmHg) are given a treatment that is medically indicated and compared with the effects in patients with a low blood pressure who do not get the treatment. In this design, the number of included patients is higher compared with an RCT, but because treatment indication reflects common practice, it may be more feasible to obtain larger number of patients.
Increasing doctors’ experience and expertise
There is a need for better teaching and training of medical doctors in their understanding of the specific needs of older patients. This requires knowledge of the pathophysiology of the ageing process and its implications for the effects of treatments. Older patients are a part of the practice of all doctors and specific attention for older patients is not restricted to the attention of geriatricians. In clinical practice the presence or absence of evidence specifically for older patients needs to be taken into account by the treating physician. Furthermore, the lack of evidence should be discussed with the patient in the light of the individual patient situation and preferences. The general lack of evidence in older age means that there is often not one single ‘best’ treatment option, and underscores the necessity of shared decision-making.58 This requires specific teaching of physicians with respect to communication skills and attitude towards the older patient.
DISCUSSION AND CONCLUSION
Taken together, the ageing process systematically affects all three elements that constitute EBM: patient situation, scientific evidence and doctors’ experience and expertise. This ultimately leads to a low level of EBM in older patients. Strategies to improve the level of evidence-based medicine in older patients include systematically assessing the patient, designing more studies specifically targeting or including more representative older patients and teaching of medical doctors about the ageing and the older patient. The level of scientific evidence for the treatment of our older patients may never reach the level of that for younger patients, as it will be impossible to repeat all clinical studies for each individual older patient with his own unique combination of comorbidities and vulnerabilities. However, not only the level of scientific evidence can be improved substantially, but also the other elements of EBM: addressing the patient situation and teaching of doctors. Arguably, the patient situation and hence patient preference may also be more heterogeneous in older patients, making the contribution of this element relatively more important than it is at younger ages and increasing the necessity to also teach doctors in ‘shared decision making’ in the light of absence of scientific evidence. In conclusion, in older patients the same elements constitute EBM, but the elements need tailoring to the older patient. Given the paucity of clinical studies that are valid for older patients more clinical studies in representative older patients are warranted. In the clinic, a thorough assessment of the individual patient preferences and physical, mental and social functioning in combination with increased level of experience of the doctor can guide individualised treatment decisions.
DISCLOSURES
The Institute for Evidence-Based Medicine in Old Age (IEMO) is funded by the Dutch Ministry of Health and Welfare and supported by ‘ZonMW (project number 62700.3002)
REFERENCES