KEYWORDS
Haemorrhagic fever with renal syndrome, Seoul virus, viral haemorrhagic fever, zoonoses
BACKGROUND
In January 2015, the first conclusive evidence was presented for the circulation of Seoul hantavirus (SEOV) in wild brown rats (Rattus novergicus; Norway rats) in the Netherlands.1 The report of circulation of SEOV in the Netherlands followed recent findings of SEOV infections in humans and rats in other North-Western European countries and underlines the emerging character of SEOV-related disease in Europe. SEOV can cause haemorrhagic fever with renal syndrome (HFRS) in humans and is transmitted from rats to humans by inhalation of aerosolised excreta from infected rats.2-4 Until now, there has only been evidence for the circulation of two other hantaviruses in wild rodents in the Netherlands, namely Puumala virus (PUUV) in bank voles (Myodes glareolus) and Tula virus (TULV) in common voles (Microtus arvalis),5 with an annual incidence of notified clinical human PUUV cases varying between 4 and 24.6 Evidence for underdiagnosis of infections with hantaviruses in the Netherlands exists with a lack of awareness for HFRS among physicians as a likely explanation.6,7 The presence of SEOV in rat populations in the Netherlands has direct implications for the clinician and routine hantavirus diagnostics. Here, we review the current knowledge on the clinical manifestation of SEOV versus PUUV infections in humans, the treatment of clinical cases and diagnostics.
EPIDEMIOLOGY
Hantaviruses (family Bunyaviridae, genus Hantavirus) are the aetiological agents of HFRS in Eurasia, and hantavirus cardiopulmonary syndrome (HCPS) in the Americas. HFRS is diagnosed in more than 10,000 individuals in Europe annually and the recorded numbers of hantavirus infections in Europe have been steadily increasing during the last 20 years.3,4 Hantaviruses are carried by rodents, insectivores (Soricomorpha) and bats, and most hantaviruses are restricted to a single reservoir host species. Hantaviruses pathogenic to humans are all associated with rodent reservoirs and humans become infected through inhalation of aerosolised excreta from infected rodents.4 The majority of HFRS cases in Europe are caused by PUUV hosted by the bank vole (Myodes glareolus).4 In addition four genotypes of the Dobrava-Belgrade virus (DOBV) can be found across Europe, each associated with its specific Apodemus spp. and causing HFRS with different degrees of severity. These include DOBV-Aa carried by A. agrarius, which is recognised by the International Committee on Taxonomy of Viruses as a unique hantavirus species, Saarema virus (SAAV). The classification of Apodemus-borne hantaviruses is still under debate, hence SAAV and DOBV-Aa are both used in the literature to indicate A. agrarius associated hantavirus.8,9
The specific relationship between hantaviruses and their carriers makes host ecology the deciding factor in the geographic distribution of these viruses, resulting in a clear distinction between Old World and New World hantaviruses.10 SEOV is the only hantavirus with a worldwide distribution as its main reservoir, the brown rat is omnipresent due to global trade and human migration in the past centuries.11,12 In Europe, evidence for SEOV circulation in brown rats has been accumulating in the past two years with molecular evidence in wild rats in France, Belgium and the United Kingdom (UK), and in pet rats in the UK and Sweden.13-19 Besides a few reports on zoonotic transmission of SEOV through handling of laboratory rats in the 1980s and 1990s in Belgium, France, the Netherlands and the UK,17 reports on human infections with SEOV outside Asia are rare and limited to urban settings.20-22 The first non-laboratory related infections with SEOV that were reported in Europe were in a farmer in the UK and a pregnant woman in France in 2012, both in rural settings and most likely due to indirect contact with wild brown rats.15,23,24 A seroprevalence study among farmers in the same region in the UK suggested a widespread rural circulation of SEOV.25 In 2013, three human SEOV cases were reported among pet rat owners in the UK.13,26 In 2014 serological and molecular evidence was found for the circulation of SEOV in wild brown rats in a region in the east of the Netherlands.1 However, an investigation in a syndromic cohort in the Netherlands in 2010 and 2011 did not yield evidence for human SEOV infections in the Netherlands.7
VIROLOGY
Hantaviruses are negative-stranded, enveloped viruses with a tri-segmented RNA genome. The large segment (L) codes for the RNA polymerase, the medium segment (M) codes for the surface glycoproteins Gn and Gc, and the small segment (S) codes for the nucleocapsid protein. The termini of these RNA segments contain conserved regions and are often used as targets for detection of hantaviruses in patients and reservoir hosts.4
CLINICAL MANIFESTATION
Haemorrhagic fever with renal syndrome
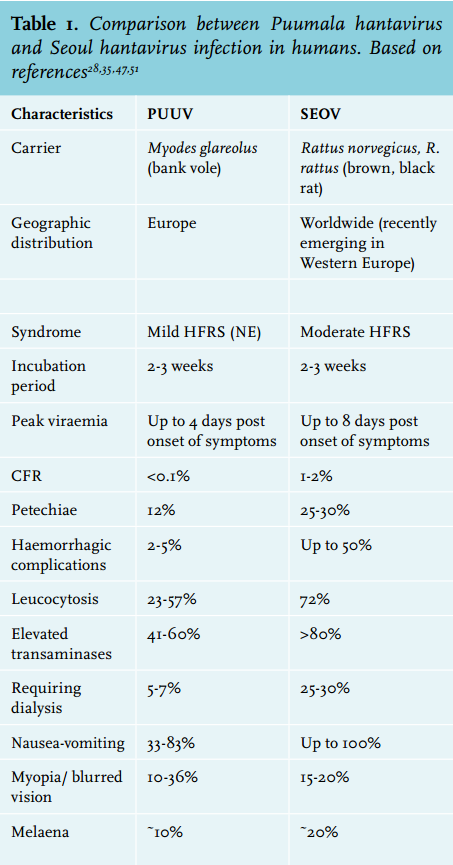
The classic presenting symptoms, often referred to as the HFRS triad, of Old World hantavirus infection, are the combination of acute kidney injury (AKI) and fever which could both potentially be accompanied by (severe) bleeding complications.2 Although bleeding complications only occur in a minority of HFRS patients (namely 5-60% of the symptomatic cases depending on the causative hantavirus species) HFRS-causing hantaviruses are generally classified among the viral haemorrhagic fever pathogens.27,28 In general, five phases can be recognised in the disease course of HFRS: first, after an incubation period varying between two to three weeks, patients enter a febrile phase characterised by high fever (> 39 °C) accompanied by aspecific ‘flu-like’ symptoms such as myalgia and a severe headache. This phase is followed by a hypotensive state which is very likely to be the result of inadequate vascular tone and increased vascular permeability associated with pathological findings of pulmonary and retroperitoneal oedema.27 After this shock-like condition patients could develop oliguria which is followed by a diuretic phase and eventually convalescence.2,27 Of the three hantaviruses known to circulate in the Netherlands, PUUV causes a mild HFRS, which also seems to be the case for TULV, although evidence for the clinical course of TULV in human remains scarce. Based on data from Asia and case reports in Europe, SEOV seems to cause a moderate HFRS with, in general, a more severe clinical outcome of the disease when compared with PUUV and TULV.
Puumala virus: mild HFRS, nephropathia epidemica
Until now the basic assumption in the Netherlands is that all cases of HFRS are caused by PUUV, although infection with TULV cannot be excluded due to the use of serology-based diagnostics (see below). The clinical course and outcome of PUUV have been relatively well studied in Europe.29,30 The majority of PUUV infections are asymptomatic (70-80%) and PUUV HFRS is considered a ‘mild’ form of HFRS, often referred to as nephropathia epidemica. 31 Most of the symptomatic patients present with AKI, fever and limb and back pain potentially accompanied with nausea and vomiting. The case fatality rate (CFR) for PUUV varies at around 0.1% and is especially associated with the age of the infected individual. Most nephropathia epidemica deaths occur in older persons and fatalities in patients below 50 years of age are rare.32 The percentage of clinical cases that develop haemorrhagic complications is estimated to lie between 1-5%. Both CFR and the percentage of clinical cases with bleeding complications are considerably lower when compared with other Old World hantaviruses, such as SEOV, which cause moderately severe HFRS (see below).29,31 Laboratory analysis most often reveals a clear thrombocytopenia combined with increased creatinine levels. Furthermore, the leukocyte count is elevated and left-shifted combined with elevated C-reactive protein levels. Sporadic long-term complications of nephropathia epidemica include hypertension, proteinuria and persistent haematuria.29 PUUV infections have been notifiable in the Netherlands since December 2008.
Tula virus: unclear, most likely mild HFRS
Descriptions of the clinical course of TULV infection in humans are rare. The detection of TULV-specific antibodies in German forestry workers and healthy blood donors in the Czech Republic strongly suggests that TULV can be transmitted to humans. Furthermore, TULV infection resulted in an HFRS-like syndrome with severe lung involvement in an immune compromised patient in the Czech Republic. Another TULV case report describes a period of fever and exanthema in a patient bitten by a rodent.33-36
SEOV: moderate HFRS
The specific course of HFRS caused by SEOV is less well studied than that of PUUV and some discrepancies between studies are present. As in nephropathia epidemica, most patients present with the classic triad of fever, renal insufficiency and possibly accompanied by bleeding symptoms. Of importance is the high number of patients that also show gastrointestinal symptoms at the time of presentation. SEOV is classified as causing a ‘moderate’ form of HFRS with a CFR of 1-2% when compared with severe HFRS caused by DOBV and Hantaan virus (HTNV), which have a CFR > 10%.37 Multiple cohort studies (mainly from China) describe signs of haemorrhage (petechia, haematuria and epistaxis) in about 50% of the patients diagnosed with SEOV-caused HFRS, which is remarkably higher than the 5% reported for PUUV, but lower than the 70-80% reported for HNTV and DOBV.38,39 A recent case report of a SEOV infection in France described severe disease with signs of haemorrhage and increased liver enzymes in a pregnant woman.24 Increased liver enzyme levels are of interest since these were also present in the other European SEOV case in the United Kingdom.23 The pronounced elevation of the liver enzymes made the treating physicians first suspect viral hepatitis or leptospirosis as the causative pathogens, and is in general not mentioned in the classical clinical picture of an HFRS case and especially not in PUUV. Actually, it has been suggested that liver involvement could be used as one of the key differentiators between SEOV infection and other hantavirus infections.40,41 In the clinical cohort studies higher numbers of patients with proteinuria, liver injury and a longer febrile period have been reported in SEOV cases. However, one should take into consideration that the PUUV and SEOV clinical studies were performed in different populations, namely Western-European and Asian cohorts.
Presenting symptoms outside the classical HFRS triad are increasingly being reported in the literature and could lead to ‘missed’ cases and subsequent underdiagnosis.7 Furthermore, recent papers debate the absolute difference between HFRS and HCPS hantavirus syndromes. It seemed in many cases that symptoms overlap and HFRS cases presented with acute respiratory failure without signs of kidney involvement while HCPS patients may show renal complications.42 Therefore, it has been suggested to use the term ‘hantavirus disease’ for all hantavirus-related described syndromes.
CLINICAL MANAGEMENT AND TREATMENT
In both HFRS caused by SEOV and in HFRS/nephropathia epidemica due to a PUUV infection the initiation of prompt and proper supportive treatment is crucial, such as monitoring fluid balance, diuresis, kidney function and the use of fresh frozen plasma/transfusions in case of haemorrhagic complications when necessary.32,43 Small trials and case reports have shown that ribavirin treatment can be useful in the very early phase of HFRS by reducing the risk of haemorrhagic events and the severity of renal insufficiency.43-46 Interferon inhibits hantavirus replication in vitro but shows no beneficial effect in vivo, and the same holds true for adjunctive prednisolone treatment which showed no beneficial outcome in a placebo-controlled clinical trial.2,43,44,47 Recently, two case reports described efficient treatment of severe PUUV cases in Finland with the bradykinin receptor antagonist icatibant.48,49 Since treatment and supportive care in PUUV and SEOV are the same, the importance for clinicians to differentiate between the two infections lies in the clinical course of infection and prognosis. Since both the haemorrhagic complications and CFR are much higher in SEOV, when compared with PUUV, clinicians might tend to provide an early start of ribavirin treatment in SEOV HFRS cases, where in PUUV the relative course of disease might not outweigh the side effects of ribavirin treatment.
DIFFERENTIAL DIAGNOSIS
As for most viral haemorrhagic fever pathogens, HFRS caused by SEOV has a broad differential diagnosis. Especially early in disease when symptoms are most likely to be aspecific it is impossible to differentiate between other viral or bacterial infections purely on a clinical basis. The broad differential diagnosis of an acute SEOV infection includes acute kidney injury, acute abdomen, septicaemia and more specifically leptospirosis, scrub typhus, murine typhus, dengue, haemorrhagic scarlet fever and the spotted fevers.50 Considering that the distinction between HFRS and HCPS might not be as clear as historically thought, one should keep in mind that the differential diagnosis of more aspecific presentations of HFRS warrants a much broader differential diagnosis and subsequent diagnostic approach.
DIAGNOSTICS
The current diagnostics of HFRS in the Netherlands (and the majority of North-Western Europe where only PUUV and TULV are known to circulate)51 relies on the basic assumption that PUUV is the causative agent. HFRS (nephropathia epidemica) by PUUV is routinely diagnosed by serology, as the viraemic stage is short and diagnostic requests for HFRS are often too late in the course of disease to justify diagnostics by reverse transcriptasepolymerase chain reaction (RT-PCR). However, the extent of viraemia varies per hantavirus species. In nephropathia epidemica, the level of viraemia is considerably lower than in more severe forms of HFRS as caused by SEOV.4 As a consequence infection with SEOV might provide a broader time window for molecular detection than PUUV. For PUUV the optimal timeframe for molecular detection lies within the first four days of onset of illness,4,52,53 while for SEOV routine molecular detection has been described up to eight days post onset of disease,24,28,38,52,53 with one report even mentioning molecular detection in the second week.28 Therefore, molecular testing for HFRS using a genus-wide or PUUV/ SEOV multiplex RT-PCR on samples taken up to eight days after onset needs to be considered in countries with known circulation of both PUUV and SEOV.
Since almost all acute cases of HFRS have IgM and IgG antibodies against the nucleocapsid protein of hantaviruses, serodiagnostics are the most commonly used method for verifying hantavirus infection using indirect IgG and IgM enzyme-linked immunosorbent assays (ELISA), IgM capture ELISAs or immunofluorescence assays (IFA).54,55 However, routine hantavirus serology targeting PUUV as causative agent might encounter problems with the ready detection of antibodies specific to SEOV. Although cross-reactivity exists in hantavirus serology, PUUV and SEOV are in different cross-reacting serogroups reflecting the relatedness of their carrier rodents. PUUV antibodies show the strongest cross-reaction with TULV and New World hantaviruses such as Sin-Nombre virus (SNV) while SEOV antibodies show strong cross-reactivity with the genotypes of DOBV/SAAV and HNTV. Between these two groups the cross-reactivity is weak or sometimes completely absent.2,51 The weak cross-reactivity in the serological response between the two groups is reflected in the test specifications for some commercial PUUV-specific ELISAs and IFAs which report a (strongly) reduced diagnostic efficiency for SEOV and are therefore not indicated for the diagnosis of HFRS caused by SEOV. Genus-wide ELISA methods using a cocktail of antigens from different hantavirus species might address this issue. However, commercially available tests show a very low sensitivity for SEOV (as low as 50%) which will result in missed cases as well. In addition, there are mosaic IFA slides on the market which offer parallel, multiplex testing for IgM and IgG antibodies to PUUV, DOBV/SAAV (the two most common genotypes), SEOV, HTNV and SNV. According to the test specifications, the cumulative specificity and sensitivity for infection with a hantavirus are excellent, including the diagnostic efficiency for PUUV. However, the efficiency to pinpoint an HFRS case to a SEOV infection seems less optimal. Countries that have endemic circulation of both DOBV/SAAV and PUUV (North-Eastern Germany, Central Europe)50 will have covered both serogroups in their routine diagnostics, which might suffice for routine SEOV diagnostics. There are commercial ELISAs based on HTNV antigens that are offered for both DOBV/ SAAV and HTNV/SEOV diagnostics. Finally, because of the observed cross-reactivity in hantavirus serological responses, comparative virus neutralisation tests remain the gold standard in hantavirus serology to confirm an infection with a specific hantavirus species.2,7 However, as the neutralising antibodies are not always virus species-specific early in infection (probably due to both neutralising IgM and IgA), virus neutralisation is only indicated in later phases of infection and when definitive insight into the causative hantavirus species is wanted. It is important that the adequacy for SEOV diagnostics of the numerous hantavirus serology tests available on the market is evaluated in routine diagnostic settings for their performance in SEOV diagnostics.
CONCLUDING REMARKS
The presence of SEOV in rat populations in the Netherlands has direct implications for the clinician and routine hantavirus diagnostics. The clinical outcome of an infection with SEOV and PUUV will greatly benefit from an early diagnosis which will reduce the costs of unnecessary tests and treatments as well. This can be secured by increased awareness among physicians for both mild and moderate HFRS and the availability of diagnostics properly validated for both PUUV and SEOV. Laboratories performing hantavirus diagnostics in countries were SEOV emerges should review and revalidate their current hantavirus diagnostics (targeting PUUV and/ or DOBV), for adequate diagnosis of SEOV infection.
DISCLOSURES
This study was partially funded by EU grant FP7-602525 Prepare and FP7-261504 EDENext and is catalogued by the EDENext Steering Committee as EDENext 308 (http:// www.edenext.eu).
REFERENCES