KEYWORDS
Achalasia, complications, peroral endoscopic myotomy, risk factors
INTRODUCTION
Since Inoue et al.1 a pplied peroral endoscopic myotomy (POEM) to treat achalasia in 2010, its safety and efficacy have been evaluated in both animal studies and clinical trials.2-6 However, various studies have demonstrated the presence of some POEM-associated complications, such as infections, pleural effusion, haemorrhage, mucosal perforation and gastrointestinal tract fistula. The most common complications are gas-related, such as subcutaneous emphysema, pneumothorax and pneumoperitoneum. The chance of occurrence varied greatly among different reports and could be as high as 100%.7,8 Although many patients could obtain relief through conservative treatment, these complications might cause discomfort, extend the duration of the operation and even result in pulmonary a telectasis and respiratory failure in severe cases, when invasive interventions are needed to relieve the symptoms.8 Thus, it is of vital importance to detect and prevent the occurrence of complications. Our objective was to determine the risk factors for gas-related complications so as to provide the rationale for preventing the occurrence of these complications.
MATERIALS AND METHODS
Patient clinical data
A total of 216 achalasia patients receiving POEM from August 2011 to November 2013 were recruited, comprising 109 males and 107 females with a mean age of 41.9 (14-74) years. Prior to POEM, the mean Eckardt score9 and duration of symptoms were 6.2±1.7 and 4 (0.5-33) years, respectively. The Eckardt score grading was: II (n = 8), III (n = 127) and IV (n = 81). The grading of Henderson criteria10 for t he degree of oesophageal dilatation was: I (n = 21), II (n = 169) and III (n = 26). There were 11 cases of sigmoid-type oesophagus. Those undergoing previous therapy with calcium antagonists or nitrates accounted for 1.9% (4/216), stenting 1.9% (4/216), balloon dilatation 9.3% (20/216) and laparoscopic Heller’s myotomy 3.2% (7/216). Thirteen related risk factors were recorded: patient age, gender, symptom duration, previous therapies, Eckardt score, oesophageal dilatation degree, sigmoid-type oesophagus, simple longitudinal mucosal incision, tunnel length, tunnel width, myotomy depth, myotomy length and operative time. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki (6th revision, 2008) as reflected in a priori approval by the institution’s Human Research Committee. Informed consent was obtained from all patients before the procedure was performed. All patients were informed of the possible complications and other possible treatment options.
POEM procedures
POEM was performed under general anaesthesia via tracheal intubation using a single-channel endoscopy (GIF-Q260Z; Olympus, Tokyo, Japan) with a transparent cap (D-201-11802, Olympus) attached to the front. A carbon dioxide insufflator (UCR; Olympus) was used. Other equipment and accessories included a high-frequency generator (ICC 200; ERBE, Tübingen, Germany), an argon plasma coagulation unit (APC300; ERBE), a hybrid knife (ERBE, Erbe Elektromedizin GmbH) or a dual knife (KD-650Q; Olympus, Japan), an injection needle (NM-4L-1; Olympus), and haemostatic clips (HX-600-90; Olympus).
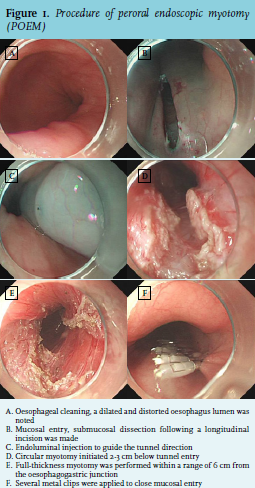
The POEM procedure was performed as follows:
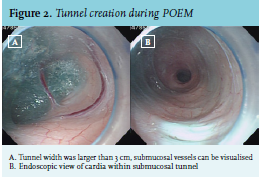
Figures 1 and 2 depict an example of the peroral endoscopic full-thickness myotomy procedure.
Follow-up
Patients were scheduled for a follow-up visit at 1, 3, 6 and 12 months after POEM and then annually for oesophagogastroduodenoscopy to observe the healing of the wound and check for any signs of reflux oesophagitis. They also underwent barium swallow to measure the oesophageal diameter. Patients were contacted by telephone to assess the occurrence of complications and obtain a current Eckardt score.
Statistical analysis Continuous variables were expressed as mean ± standard deviation. All data were analysed with SPSS17.0 statistical software. Chi-square or Fisher’s test was used for univariate analyses and logistic regression for multivariate analyses.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation. All data were analysed with SPSS17.0 statistical software. Chi-square or Fisher’s test was used for univariate analyses and logistic regression for multivariate analyses.
RESULTS
Clinical efficacies
Of the 216 patients, 86 underwent a simple longitudinal incision, while the others underwent additional submucosal dissection of at least 0.5 cm along both sides of the longitudinal incision. The width of the submucosal tunnel was > 3 cm in 100 cases and ≤ 3 cm in another 116. Simple circular myotomy was performed in 83 cases, while full-thickness myotomy in 133 cases. The overall treatment success rate (Eckardt score ≤ 3) was 99.1% (214/216). The average operative time was 59.1 (38-120) min, and average follow-up period 16.8 (6-33) months. As compared with pre-operation, the Eckardt score decreased markedly at 12 and 24 months after the operation (0.54 vs. 6.1, 0.56 vs. 6.0, p < 0.001); the average oesophageal diameter decreased significantly at six months’ post-operation (53.7 vs. 30.8 mm, p < 0.001). There was no recurrence during the follow-up period (recurrence was defined as an Eckardt score ≥ 4 at > 6 months post-operation).
Complications
Of the total patients, 28 (13.0%) had complications, namely gas-related complications (n = 22, 10.2%), tunnel mucosal perforation (n = 3, 1.39%), reflux oesophagitis (n = 2, 0.92%) and acute peritonitis (n = 1, 0.46%). The 22 cases of gas-related complications were subcutaneous emphysema (n = 21) and mediastinal emphysema plus subcutaneous emphysema (n = 1). For the 21 cases of simple subcutaneous emphysema, no special intervention was required, and all were absorbed spontaneously within 3-5 days. The patient with mediastinal emphysema plus subcutaneous emphysema had chest tightness, which disappeared after deflation through a subcutaneous puncture. For three cases of tunnel mucosal perforation, 1-2 clips were applied for closure. After an oral intake of PPI, the symptoms of patients with reflux oesophagitis were relieved. The patients with acute peritonitis had a postoperative onset of moderate fever (highest body temperature of 38.9°C), epigastric pain, epigastric tenderness and rebound tenderness. The symptoms subsided after a five-day course of antibiotics.
Risk factors for gas-related complications
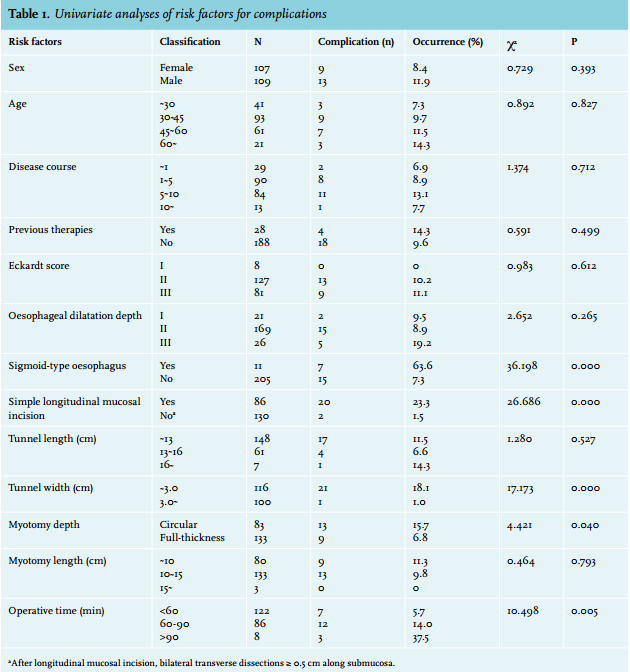
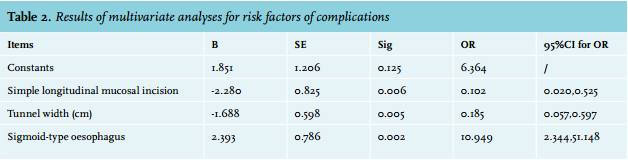
Univariate analyses revealed that simple longitudinal mucosal incision, tunnel width, sigmoid-type oesophagus, myotomy depth and operative time were risk factors for gas-related complications (table 1). Multivariate analyses further indicated that simple longitudinal mucosal incision, tunnel width and sigmoid-type oesophagus were risk factors, but not myotomy depth and operative time. The occurrence of complications increased for those patients with a simple longitudinal mucosal incision, tunnel width ≤ 3 cm and sigmoid-type oesophagus (table 2).
DISCUSSION
Achalasia is an oesophageal motility disorder characterised by lack of peristalsis of the oesophageal body and impaired relaxation of the lower oesophageal sphincter with clinical symptoms including dysphagia, chest pain, regurgitation, and even coughing and aspiration pneumonia.11 POEM is a novel technique for the treatment of achalasia with exciting results in both animal experiments and clinical studies.2-6 As shown in an international prospective multicentre clinical trial, POEM has become an effective therapeutic modality for achalasia.12 As demonstrated by clinical trials, gas-related complications occurred frequently during POEM. Although the occurrence varies greatly in different reports, it may reach up to 100%.7 The gas-related complications are known to include subcutaneous emphysema, pneumothorax, pneumoperitoneum and mediastinal emphysema. The cases with mild complications usually presented with merely a small amount of subcutaneous emphysema, which did not require any special intervention. In severe cases, however, vast gas accumulation may occur in the chest, abdominal cavity, mediastinum or under the skin. Sometimes acute respiratory and circulatory failure and even death may occur. In such a setting, emergency invasive interventions of deflation via subcutaneous puncture and closed thoracic drainage should be taken for symptom relief.8 In addition, severe emphysema in the patients may cause great suffering, increase the operative time and hospitalisation duration and increase the economic burden as well. Thus it is of vital importance to know how to prevent the occurrence of complications. As revealed by the results of multivariate analyses, simple longitudinal mucosal incision, tunnel width and sigmoid-type oesophagus are independent risk factors of gas-related complications during POEM. In the cases of simple longitudinal mucosal incision or tunnel width ≤ 3 cm, sigmoid-type oesophagus, the occurrence of gas-related complications increases dramatically. Two methods, transverse and longitudinal incisions, are available for creating tunnel entry in POEM. Transverse incisions will not result in close contact between tunnel entry and the endoscope, facilitating gas discharge from the tunnel and lowering the occurrence of gas-related complications.13 However, endoscopic closure of a transverse incision in the oesophagus is technically difficult or loose, which likely results in intra-tunnel infections and gastrointestinal tract fistula. In contrast, it is easy to close the entry site to the tunnel using longitudinal incisions. Nevertheless, close contact between endoscope and tunnel entry may ensue, which forms a high-tension status within the tunnel so that there were increased risks of gas-related complications. To effectively solve the above dilemma, we performed the subsequent submucosal dissection of at least 0.5 cm along both sides of the longitudinal incision. Our cohort study has shown that, when a simple longitudinal incision was used, the occurrence of gas-related complications was 23. 3% (20/86). However, the occurrence of gas-related complications was significantly reduced to 1.54% (2/130) when submucosal dissections for at least 0.5 cm were performed along both sides of the longitudinal incision. Therefore, we believe that subsequent submucosal dissection along both sides of the longitudinal incision while creating tunnel entry in POEM could effectively lower the occurrence of gas-related complications.
In addition, we found that tunnel width was an independent risk factor for gas-related complications. The occurrence was 18.1% (21/116) in the cases with a tunnel width ≤ 3 cm, but it decreased to 1% (1/100) in the cases with a tunnel width > 3 cm. These findings suggest that sufficient tunnel width might markedly reduce the risk of gas-related complications. Since the endoscope itself occupies a certain amount of space, the tunnel should be wide enough to ensure the presence of ample space between the instrument and tunnel during the procedure. In this way, sufficient space could not only reduce the difficulty in handling the endoscope within the tunnel, but also lessen the procedure-related injuries of tunnel mucosa, blood vessel, peri-oesophageal or gastric serous membrane. Moreover, this facilitates gas diffusion and prevents the formation of high pressure within the tunnel, particularly in an extremely twisting oesophagus. Inoue et al. recommended that tunnel width should be greater than or equal to one-third of the oesophageal circumference during POEM.14 In our experience, to effectively lower the occurrence of gas-related complications during POEM, tunnel width should be > 3 cm for those patients without obvious oesophageal twisting.
Sigmoid-type oesophagus was another independent risk factor for the occurrence of gas-related complications. In the present cohort, the occurrence of gas-related complications for patients with sigmoid-type and non-sigmoid-type oesophagus was 63.6% (7/11) and 7.3% (15/205) respectively. Sigmoid-type oesophagus, especially type S2, was previously considered to be a relative contraindication of POEM.15 Due to oesophageal twisting, it is difficult to create a submucosal tunnel in patients with sigmoid-type oesophagus. And the curvature interferes with gas discharging out of the tunnel, which might form a state of high pressure within the tunnel so as to cause such complications as subcutaneous emphysema, pneumothorax and pneumoperitoneum. In the present study, all the six patients with sigmoid-type oesophagus before March 2012 had an onset of gas-related complications with an occurrence of 100%. However, the occurrence of gas-related complications significantly dropped to 20% (1/5) in patients with sigmoid-type oesophagus thereafter. In our opinion, to reduce the occurrence of gas-related complications, more attention should be paid to the following points of caution:
In addition, we also found that myotomy depth was not a risk factor for gas-related complications. During POEM, most researchers preferred to adopt a simple circular myotomy and preserve the longitudinal muscular layer in order to reduce the chance of gas entry into the thoracic and abdominal cavity. However, some studies have demonstrated that the application of full-thickness myotomy did not increase the occurrence of complications. Moreover, full-thickness myotomy helps accelerate the functional recovery of oesophageal peristalsis and shorten operative duration.7,16 Notably, the longitudinal oesophageal muscle layer is relatively thinner, and is closely connected with the circular muscle, but not with the peri-oesophageal membrane. Unintentional splitting of longitudinal muscle is likely to occur during simple circular myotomy, either due to intra-operative mechanical trauma or electrocautery damage. In our experience, to prevent tunnel perforation and gas-related complications during POEM, one of the most important steps is to maintain the integrity of peri-oesophageal or serous membrane. Yet the integrity of longitudinal muscle should not be overemphasized. In conclusion, simple longitudinal mucosal incision, tunnel width and sigmoid-type oesophagus are independent risk factors for gas-related complications for achalasia during POEM, but not myotomy depth and operative time.
ACKNOWLEDGEMENTS
Professor Yan Yan, Department of Statistics, School of Public Health, Central South University provided great assistance in the statistical analyses.
DISCLOSURES
The authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES