|
|
CASE REPORT
A 25-year-old patient was seen at the outpatient clinic of internal medicine three months after a two-month stay in South America because of a progressive (over two weeks) skin lesion (papule with evolution to an ulcer) on the left lower leg. He had participated to a survival training in the jungle of French Guiana. This training often impeded personal protective measures (use of long-sleeved clothing, insect repellents and impregnated bed netting). Prophylactic treatment with mefloquine was taken correctly. The clinical examination revealed an ulcer with a diameter of 3 cm on the left lower leg (figure 1). The patient was afebrile and the rest of the physical examination was unremarkable. A biopsy of the edge of the lesion was performed.
DIAGNOSIS
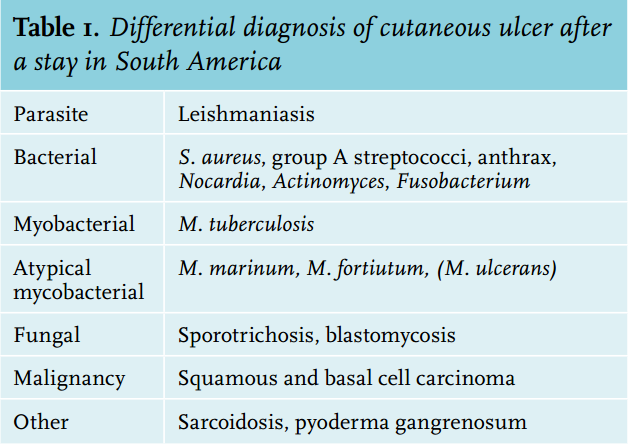
By means of direct microscopy, which determined Leishmania parasites, the diagnosis of cutaneous leishmaniasis was established. Species-specific diagnosis (L. guyanensis) was made by polymerase chain reaction (PCR). Treatment with intravenous pentamidine was administered with favourable evolution after three infusions: residual depressed and retracted scar (figure 2). The spectrum of dermatological diagnoses in travellers is broad.1 Because of his stay in South America, cutaneous leishmaniasis needed to be included in the differential diagnosis (table 1). However, a delay in diagnosis often occurs: the diagnosis was missed by the general practitioner in 38% of cases in a French study.2
Leishmaniasis is caused by various Leishmania parasite species and is transmitted through sandfly bites (Phlebotomus (Old World) and Lutzomyia (New World)). Depending on the causative Leishmania species and the host immune response, the clinical presentation is cutaneous, mucosal or visceral disease. Although all types of skin lesions (papules, nodules) might be seen in cutaneous leishmaniasis, ulcers are the most frequent. Incubation time varies (weeks to months). Occasionally, according to the species (and sometimes months after the appearance of the cutaneous leishmaniasis lesions) mucosal disease (nose and pharynx) can develop.3 Central and South America (New World cutaneous leishmaniasis) and Africa and the Middle East (Old World cutaneous leishmaniasis) are leishmaniasis-endemic regions. Diagnosis can be made by microscopy (sensitivity 19-77%) and culture (sensitivity 58-62%). PCR, however, is the method of choice because it allows species determination and it has high sensitivity (89-100%).3 Treatment modality (local vs. systemic) depends on the causative Leishmania species (PCR genotyping) and number, size and location of the lesion(s).4
REFERENCES