KEYWORDS
Blood culture, quality improvement, risk assessment
INTRODUCTION
Approximately 23% of all hospitalised patients in the Netherlands receive antibiotics due to a suspected bacterial infection.1 Blood cultures are essential diagnostic tools to identify pathogens in systemic infections.2-4 This identification is crucial for tailoring antibiotic treatment to pathogen-directed therapy, often resulting in a switch from intravenous to oral therapy. Both steps are essential for adequate antibiotic treatment, better patient outcomes, lower hospital costs, and, in the long run, a decrease in antimicrobial resistance.5-8
Based on previous studies, the current recommendations for adequate blood culture performance in most Dutch hospitals, including ours, requires collection of at least two sets of blood cultures from independent punctures with 8-10 ml blood per bottle prior to start of antibiotic treatment.2,3,9-11 Previously, we have shown that blood culture results from two sets are available in only 48.8% of the patients who have an indication for blood cultures.12 In our academic hospital, this percentage was even lower at 33%. This result, combined with a worldwide call for awareness on the appropriate use of antibiotics,13,14 justified the initiation of a risk assessment into the root causes of suboptimal logistics of blood culture performance in 67% of our patients. The quality of a blood culture result relies largely on the quality of the pre-analytical phase and therefore we evaluated the whole process of blood culture performance starting from the ordering of blood cultures until the moment results are made available to the treating physician.
The quality system of our JCI-accredited hospital recommends proactive risk assessments as a method to improve systems of care.15 Motivated staff members, including nurses, medical specialists, and quality healthcare workers, are trained in two methods: the Bow-Tie method and the healthcare failure mode and effect analysis (HFMEA), to enable hospital-wide awareness and knowledge of risk assessment.
In the current study, we illustrated the utility of both methods in evaluating the process of blood culture performance.
METHODS
Hospital setting
Approximately 100 healthcare workers – both physicians and nurses – work in the emergency department (ED) and about 30,000 patients visit the ED every year. Seventeen technicians work in the laboratory for medical microbiology. Nearly 12,500 blood culture sets are processed in the laboratory each year. On average, 77% of the blood culture samples are in the incubator within two hours of being drawn. No decentralised incubators are present in the hospital. Blood cultures are transported 24 hours per day, seven days per week by nurses, doctors, residents, and couriers. They place the blood cultures in the blood culture device. If a culture becomes positive, the blood is poured over an agar plate and incubated for approximately four hours. Thereafter, the colonies are tested by MALDI-TOF. in addition to this technique, we also prepare a Gram stain. When positive culture bottles are flagged, the initial result is reported to the clinic within two hours. The contamination rate of blood cultures was 3.2% of all sampled blood cultures, and 22.7% of the positive blood cultures in 2015. Our laboratory is accredited according to the international standard (ISO) 15189 standards.
The Bow-Tie chart
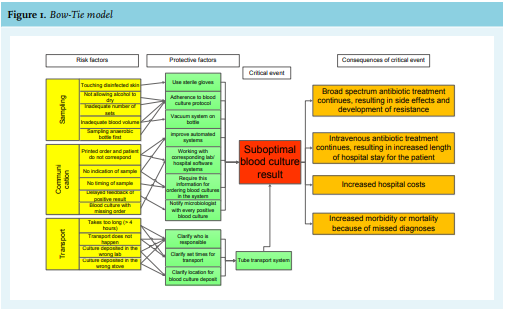
To identify root causes of a suboptimal process of blood culture performance, we first gathered data through direct observations in the ED and the microbiology laboratory. One researcher (MB) observed the process from the moment that a physician ordered blood cultures in the ED until the culture results appeared in the patient’s electronic medical record. All acts and difficulties were reported using a standardised format, which included reporting of human errors, equipment problems, communication difficulties, or any other factor that disrupted the flow of blood culture processing. Additionally, the researcher asked healthcare workers involved in the process about their perception on possible risk factors for a suboptimal process of blood culture performance. Then we modelled our findings using a hospital Bow-Tie chart format. The Bow-Tie model combines the risk and protective factors of a so-called ‘critical event’ with its consequences in one figure.16 Bow-Tie models have been used to evaluate risks in the petrochemical industry and aviation;16-17 they have also been applied more recently to the medical field.18,19 The ‘critical event’ refers to the final result that should be prevented, such as ‘gas leakage’.17 Therefore, we defined the ‘critical event’ as ‘a suboptimal blood culture result’ meaning that the pathogen is not identified.
The healthcare failure mode and effect analysis (HFMEA)
HFMEA originates from the failure mode and effect analysis that has been used successfully by other industries, including aviation.20 The methodology of the HFMEA has been comprehensively described,21,22 and it has also been applied in daily practice.23-26 Briefly, a HFMEA involves the close examination of an error-prone process by a multidisciplinary panel. In this analysis, the process is divided into small steps. Potential failure modes and their consequences are identified per step. Although each potential failure mode has some effect on the efficiency of the process, each failure mode cannot be addressed at once. Priority is given to failure modes in which improvements are needed most. Therefore, risk scores are assigned to all identified potential failure modes. This risk score is based on likelihood of occurrence, severity, and detection. A high-risk score indicates priority for action.20,21
The information gathered in the Bow-Tie model was used as input for HFMEA. As with the Bow-Tie model, we used a chart that was designed by the quality and safety department of our hospital. Again, we evaluated the process from the moment that the physician ordered blood cultures in the ED until the culture results appeared in the patient’s electronic medical record.
HFMEA started by establishing a multidisciplinary panel of key stakeholders and experts. The panel performed three brainstorm sessions resulting in identification of improvement actions. In a first brainstorm session, panel members were asked to suggest potential failure modes and their consequences in the process of blood culture performance. In a second session, they estimated which failure modes in the HFMEA had a high-risk score and thus, a high priority for action. These risk scores were based on the panel members’ experiences. Possible categories for actions per failure mode were ‘acceptation’, ‘control’, ‘elimination’, or ‘study’ (in case more information was needed on the risk score of this failure mode). The multidisciplinary panel was also asked to identify potential risk-reducing interventions for the most urgent failure modes. In a third session, accomplishable interventions were planned. The facilitator updated the HFMEA chart after each session.
Institutional Review Board
Approval Since the study involved a quality improvement project at the hospital level with negligible risk of harming patients, individual informed consent was waived. The Board of Directors of our institution approved the study.
RESULTS
The observations and short interviews were held in January 2015. Figure 1 presents our findings in the Bow-Tie chart. HFMEA was performed between January and September 2016. The panel consisted of one infectious diseases specialist, one acute care specialist, one medical microbiologist, two emergency department nurses, one quality officer, and one ‘lean coach’ from the microbiology department, who is specialised in the continuous optimalisation of working processes, with a focus on value and quality, and elimination of misconceptions. The facilitator was a researcher in the field of infectious diseases. Both the infectious disease specialist and the facilitator were trained in the Bow-Tie method and HFMEA by the Department of Quality and Safety. Table 1 presents the final chart.
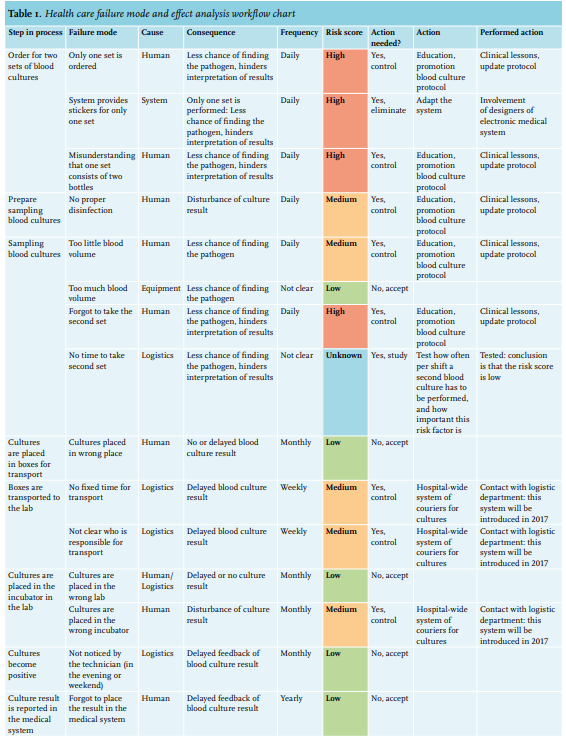
The multidisciplinary panel determined that the lack of a second set of blood cultures was the problem with the highest priority for action. The absence of a second set of blood cultures was the consequence of several potential failure modes, including three human factors (‘only one set ordered’, ‘misunderstanding that one set consists of two bottles’, and ‘forgot to take the second set’), one system error (‘system provides stickers for only one set’), and one potential logistic factor (‘no time to take the second set’) (table 1). To address the human factors, we gave clinical lessons to nurses in the ED in July 2016. In these clinical lessons, we reminded nurses that blood culture sets consist of two bottles and that two sets are four bottles. Furthermore, we stressed the importance of a second culture set for the interpretation of the result (contamination or pathogen) and for increasing the chance of detecting the pathogen. In total, five lessons were given and approximately 90% of all nurses working in the ED joined at least one lesson. 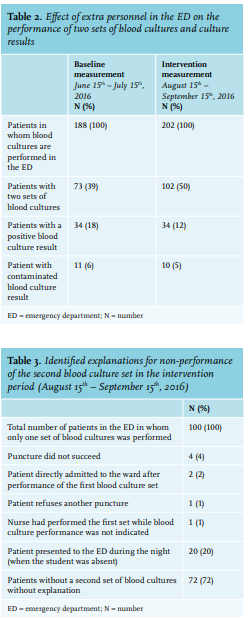
We reasoned that use of the blood culture protocol could also guide appropriate blood culture sampling. Although our hospital did have a protocol for blood culture performance, it was not easy to find. Therefore, we updated the search engine of the protocol database in such way that, when searching for “blood cultures”, “blood culture,” or “blood culture performance” the correct protocol appeared directly. Search terms for the protocol were updated in June 2016. We promoted use of the protocol during the clinical lessons in July 2016. In October 2016, unit nursing officers sent an email to remind nurses to use the protocol.
To address the system error involved in obtaining a second blood culture (‘system provides stickers for only one set’), we contacted the electronic medical system designers. They developed a module in the electronic medical system in which the healthcare worker can choose to order one, two, or three sets of blood cultures and the number of required stickers are printed automatically. This module was finished in March 2018. In April 2020, a post-intervention sample analysis showed that two sets of blood cultures were performed in 85% of the patients.The panel members disagreed on which risk score needed to be assigned to the logistic failure mode ‘no time to take the second set’. Therefore, the action ‘study’ was chosen to identify the urgency of this failure mode and to determine the effect of extra personnel on the number of blood cultures obtained per patient. Medical students were posted in the ED, seven days a week, 16 hours a day (between 7:00 AM and 11:00 PM), between the August 15th and September 15th, 2016. These students obtained the second blood culture set after the nurse sampled the first set. All students were trained in blood culture sampling. Nurses notified the students when an eligible patient was present and the students kept an eye on the registration board in the ED to make sure as few as possible eligible patients were missed. All nurses were informed about this test project in the clinical lessons by email and in a monthly newsletter. The number of blood cultures obtained per shift was determined using data that was extracted from the electronic medical system. The students reported observed explanations for not taking the second set of blood cultures on standardised forms. We extracted the number of patients admitted while the students were absent (between 11:00 PM and 7:00 AM) from the electronic medical system.
During this intervention period, 202 patients presented to the ED who required blood cultures, with an average of seven or eight patients per day, two or three patients per shift. Since several nurses work during one shift, a maximum of one patient per shift and per nurse needed blood cultures. Table 2 shows that the number of patients in whom two sets of blood cultures were taken increased by 11% in the intervention period (from August 15th until September 15th, 2016) compared to a baseline period (from June 15th until July 15th, 2016). Table 3 presents the explanations for not taking the second set during the intervention period. In the majority of the patients, no explanation was found.
We also started improvement actions on failure modes with an estimated medium risk score. ‘No proper disinfection’ and ‘too little blood volume’ during sampling were discussed using clinical lessons. To improve the transport of blood cultures from the emergency room to the microbiology laboratory, we approached the logistic distribution centre of our hospital. We enquired whether it was possible to hire a courier for the transport of cultures from the ED to the microbiology laboratory at fixed times. Personnel in the logistic distribution centre informed us that a hospital-wide distribution system would be implemented in 2020. Therefore, we optimised the current system (transport by ED assistants) for the remaining period, by scheduling one person who was responsible for the transport every two hours.
DISCUSSION
Method of risk assessment
The Bow-Tie model enabled us to gain in-depth knowledge of the root causes of a suboptimal process of blood culture performance. An important limitation of the Bow-Tie chart is that it does not allow identification of which risk factors are the most urgent. The Bow-Tie chart also did not allow prioritisation of interventions, which was an important limitation in determining which of the numerous departments involved in the process of blood culture performance should be targeted first. As a result, we struggled with translating the identified causes into actions to modify the process effectively for our purpose.
HFMEA provided useful insights in the different steps in the process of blood culture performance. The advantages of using a multidisciplinary panel are – amongst others – that it gives insight into the weaknesses of all steps of the process from different perspectives and that it provides mutual understanding. This approach helped to identify and prioritise failure modes of different steps in the process. These insights facilitated starting actions focused on the most urgent problems. The value of HFMEA in addition to the Bow-Tie model is demonstrated in identification of initial identified risk factors as described in in figure 1. Two risk factors in the Bow-Tie chart concern problems with the deposition of the cultures in the lab, while those were not classified as urgent in HFMEA. Also, some protective factors suggested in the Bow-Tie analysis – such as use of sterile gloves during blood collection – were not feasible in daily practice according to the multidisciplinary panel.
Furthermore, HFMEA demonstrated the importance of multidisciplinary communication. For example, without the involvement of the logistic distribution centre, we would currently be planning an improvement project for the transport from the ED to the microbiology laboratory concurrent to the upcoming hospital-wide distribution system.
Finally, HFMEA is usable in different situations. For example, while our analysis concerned an existing process, HFMEA has also been used to guide the implementation of a new technology.25 A disadvantage of this broad utility is that it complicates direct comparison of HFMEA’s performance due to the heterogeneity of processes.23-26
The most important disadvantage of performing HFMEA is that it can be very time consuming.26 Failure modes can be identified using direct observations, surveys among physicians, or expert panels. Systematically, it would be preferable to use all three techniques. Logistically, however, it can be preferable to choose one technique. Since we executed direct observations for the Bow-Tie model and we performed a survey among physicians to identify barriers of – amongst others – blood culture performance earlier,27 we only used the panel. During the panel meetings, we shared the knowledge from these earlier experiences. Also, we chose to estimate the risk scores based on expert opinion (the panel members). When consensus was lacking in the multidisciplinary panel - such as on the risk score of the failure mode ‘no time to take the second set’ – we collected data. This approach simplified the execution of HFMEA.
Blood culture process
The lack of a second set of blood cultures appeared to be the most important problem with the highest priority for action to improve the process of blood culture performance. Most failure modes were caused by human factors. Interventions focused on the human failure modes were relatively easy to accomplish. The effect differed per intervention, as illustrated by figure 2. Education and reminders should be incorporated into daily practice, since changing human behaviour is challenging and requires repetition.28 An alternative intervention that could actually eliminate the problem of the lack of a second set is the introduction of the so-called ‘single-sample strategy’. With this technique, the total volume of blood is collected from a single puncture, resulting in one ‘blood culture set’ existing of four to six bottles.2,29,30 Although discrimination between contaminants and pathogens is no longer possible with this technique, it does guarantee the collection of an adequate volume of blood, which is the most important parameter for the detection of pathogens.2,30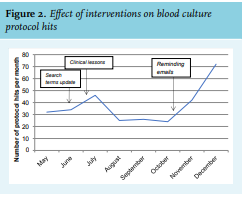
It took nearly two years to address the systemic failure mode, but after implementation of the module in the electronic medical system, we saw an impressive increase in the performance of two sets of blood cultures, with two sets of blood cultures performed in 85% of the patients.
We studied how urgent the suggested logistic failure mode ‘no time to take the second set’ is. We saw that the number of patients, in whom two sets of blood cultures were taken, increased by only 11% in the intervention period compared to a baseline period, meaning that during the intervention period, 50% of patients still only had one set of blood cultures taken. In the majority of the patients without a second set of blood cultures, no explanation was found. These results showed that the failure mode ‘no time to take the second set’ does not have a high-risk score with priority for action. Taking two sets of blood cultures in one patient per shift should be feasible. Interestingly, increasing the personnel in the ED did not result in an enormous increase of two sets of blood cultures, suggesting that hiring more personnel is not the solution for the lack of a second set.
Although we have distinguished many steps in the process of blood culture performance, we did not include all details. For example, the quality of the materials used for blood culture sampling has not been evaluated.
The most important limitation of our risk assessment is that we did not measure the effect of the improvement actions separately. To be able to determine which intervention is the most effective, each improvement action should be tested separately and preferably compared to a control hospital without the improvement action. Nevertheless, it should be stressed that the aim of this risk assessment was to illustrate the effectiveness of the Bow-Tie model and HFMEA, to identify weaknesses in the process of blood culture performance and to optimise this process, not to develop an effective improvement action.
CONCLUSIONS
The Bow-Tie model helped to gain insight into the root causes of a suboptimal procedure, while the healthcare failure mode and effect analysis helped to identify the most urgent barriers in a process and to translate these findings into improvement actions. In the evaluation of the process of blood culture performance, the lack of a second set of blood cultures was identified as the problem with the highest priority for improvement. Several failure modes, including human and system factors, were identified. At first sight, failure modes caused by human factors seemed easy to address, however changing human behaviour appeared challenging. The implementation of a module in the electronic medical system to order two sets of blood cultures, resulted in the most improvement in the performance of two sets of blood cultures.
ACKNOWLEDGEMENTS
We want to thank Vanessa Harris as a native English speaker for her corrections.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES