KEYWORDS
Blood pressure, diet, exercise, hypertension, smoking, treatment
INTRODUCTION
Hypertension (HT) is one of the most common chronic diseases in the world with a great burden on communities. It has significant complications which could result in advanced morbidity or mortality. Hypertension is among risk factors of coronary artery disease, stroke, heart failure, chronic kidney disease, peripheral vascular disease, and vascular dementia.1,2 Thus, achieving regulation of blood pressure is crucial in hypertensive subjects. There are numerous factors associated with better hypertension control in patients with HT. In addition to the reduction of waist circumference and body mass index, education of patients in acknowledging their blood pressure, compliance to the treatment, adherence to the schedule of exercise, diet modification, and reducing the number of pills for hypertension treatment are among factors that modify the regulation of blood pressure.3-5 In present prospective cross-sectional study, we aimed to observe the anthropometric measures, dietary and exercise compliance, treatment options and compliance, and awareness of the disease of the subjects with hypertension.
METHODS
The study was conducted in the Internal Medicine Department of Abant Izzet Baysal University Hospital between January 2019 and December 2019. The study protocol was approved by the local ethics committee (approval number: 2018/288). Subjects with hypertension (HT) who were admitted to outpatient internal medicine clinics of the institution were enrolled into the study. According to the Joint National Committee (JNC) VIII criteria,6 subjects with a mean blood pressure above target levels were defined as poorly-controlled hypertensive patients and others were grouped as well-controlled hypertensive patients. Blood pressure measurements were obtained in two consecutive clinic visits and the mean of these measurements were used in defining poorly- and well-controlled hypertension groups. Exclusion criteria were as follows: recently diagnosed hypertension (less than one year), modification of anti-hypertensive treatment within three months, lack of two consecutive visits for blood pressure measurements.
Age, gender, body weight, height, waist circumference, duration of HT, accompanying morbidities, diet and exercise status, smoking habit, awareness of blood pressure, anti-hypertensive medications (mono-therapy or combination), number of pills for hypertension treatment, additional medications for other conditions, systolic and diastolic blood pressures, laboratory parameters including levels of serum creatinine, blood urea, and triglycerides, as well as LDL-cholesterol and HDL-cholesterol levels were noted. Body mass index (BMI) was calculated by division of weight by the square of height. All study parameters were compared between poorly- and well-controlled hypertensive subjects.
Statistical analyses were held with SPSS software (SPSS 15.0 for Windows, IBM Co, Chicago, IL, USA). The Kolmogorov-Smirnov test was used for whether study parameters have normal distribution within study groups. Variables with normal distribution were compared with an independent samples t-test and expressed as mean ± standard deviation. Variables without normal distribution were compared with Mann-Whitney U test and expressed as median (min-max). Comparison of categorical variables was conducted with chi-square test. Statistical significance was defined as a p-value lower than 0.05. 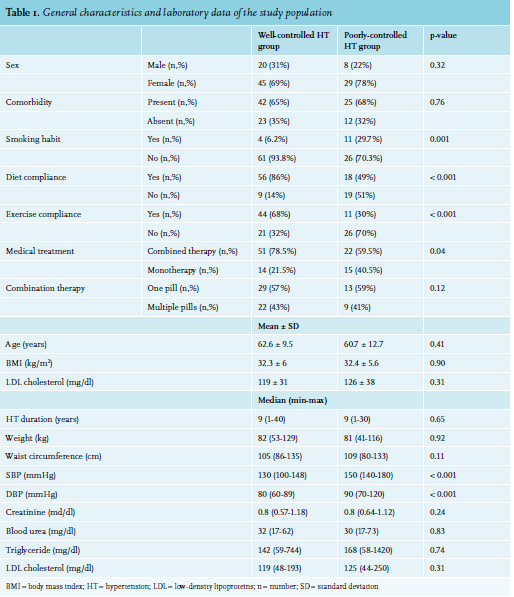
RESULTS
One hundred and forty-five subjects enrolled to the study; 43 patients were excluded according to the exclusion criteria. The study population was consisted of the remaining 102 hypertensive patients; 65 in well-controlled HT and 37 in poorly-controlled HT groups. Mean ages of the well- and poorly-controlled hypertensive subjects were 62.6 ± 9.5 years and 60.7 ± 12.7 years, respectively. The age of the patients in the well- and poorly-controlled HT groups were not statistically different (p = 0.41). In well-controlled HT group, 45 (69%) patients were women and 20 (31%) patients were men, while 29 (78%) were women and 8 (22%) were men in the poorly-controlled HT group.
Gender was not statistically different between study groups (p = 0.32). Forty-two (65%) of 65 patients in the well-controlled HT group and 25 (68%) of 37 patients in poorly-controlled HT group had comorbid conditions (p = 0.76). 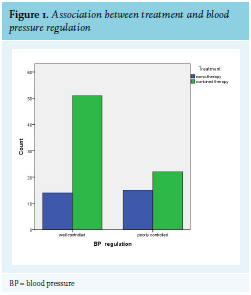
Duration of HT (p = 0.65), weight (p = 0.92), BMI (p = 0.90), waist circumference (p = 0.11), serum creatinine (p = 0.24), blood urea (p = 0.83), triglyceride levels (p = 0.74), LDL cholesterol levels (p = 0.31), and HDL cholesterol levels (p = 0.68) of well- and poorly-controlled HT groups were not significantly different. Table 1 shows the general characteristics and laboratory data of the study population. The differences of systolic and diastolic blood pressures between study groups were statistically significant (p < 0.001 for both systolic and diastolic blood pressures).
Only 4 (6.2%) of 65 patients in the well-controlled HT group were smokers while 11 (29.7%) of 37 patients in the poorly-controlled HT group smoked cigarettes. The difference between groups was statistically significant (p = 0.001). Fifty-six (86%) of 65 patients in the well-controlled HT group and 18 (49%) of 37 patients in the poorly-controlled HT group followed the dietary advice for treatment of HT (p < 0.001); 44 (68%) of the patients in the well-controlled HT group and 11 (30%) of those in the poorly-controlled HT group were on regular physical exercise (p < 0.001).
Fourteen (21.5%) of 65 well-controlled patients received only one anti-hypertensive drug as monotherapy and 51 (78.5%) of 65 received combined antihypertensive agents; while 15 (40.5%) of 37 patients in the poorly-controlled HT group received only one anti-hypertensive drug as monotherapy and 22 (59.5%) received combined antihypertensive treatment. Combined treatment was significantly more common in the well-controlled HT group compared to the poorly-controlled HT group (p = 0.04). The association between treatment and blood pressure regulation is shown in figure 1.
Of 51 subjects who received combined treatment in the well-controlled HT group, 29 (57%) received a combined treatment in one pill and 22 (43%) received treatment in multiple pills; 13 (59%) of 22 patients in the poorly-controlled HT group received combined treatment in one pill and 9 (41%) received treatment in multiple pills. There was no significant difference between well- and poorly-controlled HT groups according to the number of pills of combined treatment (p = 0.12).
DISCUSSION
The main findings of the present study were: (i) non-compliance with dietary and physical exercise program, (ii) smoking cigarettes, and (iii) treatment with monotherapy antihypertensive regimen instead of combined treatment was associated with poor control of hypertension. Interestingly, combined therapy with one pill was not superior to combined therapy with more than one pill in achieving good control of hypertension.
The association between diet and hypertension has been studied for a long time. While a Mediterranean diet, which is rich in vegetables and fruits, relates to a reduced blood pressure, excessive salt in the diet was introduced as a cause of increased blood pressure.7 Recent studies showed that a Mediterranean diet and a healthy Nordic diet were associated with a reduced risk of stroke, a serious complication of HT.8,9 Similarly, the stop hypertension (DASH) diet, which recommends consumption of fruits, vegetables, whole grains, dairy products with low fat, and nuts, along with low intake of sodium, sweetened beverages, and red meat (especially processed red meat), has been shown to be associated with a reduction in blood pressure and a decrease in the incidence of HT.10,11 Moreover, the DASH diet was also suggested to be related to a lower incidence of coronary heart disease.12 In addition, a recent meta-analysis reported that adherence to the DASH diet was associated with lower risk of stroke in patients with HT.13 The results of this present study report better blood pressure control in subjects who were compliant with dietary advices compared to those who were not, and are in accordance with data in the literature. Regular physical exercise reduces blood pressure in hypertensive patients, especially in the period after recent physical activity. Blood pressure decreases to below to pre-activity levels after 20 to 30 minutes of physical exercise.14,15 In subjects adhering to regular exercise, blood pressure reduces considerably compared to those who do not adhere to regular exercise; therefore, physical exercise is often recommended to hypertensive patients in the treatment of HT.16 Exercise of moderate intensity has been reported to be related with a lower incidence of HT.17-21 Moreover, in a recent cohort study, significantly lower HT incidence was reported in subjects who participated in skiing compared to the subjects who did not.22 Larger artery diameter, positive autonomic balance, and improved endothelial function observed in athletes could be responsible for beneficial effects of exercise seen in hypertensive patients.23 In the present study, we showed that patients on regular exercise more commonly have well-controlled blood pressure levels, which is consistent with medical literature.
Studies in literature pointed out a relationship between smoking and cardiovascular risk factors. Smoking has a hypertensive effect as it promotes arterial stiffness and induces sympathetic system; therefore, smokers are more prone to elevated blood pressure levels.24 In the present report, there was an increased number of smoking patients in the poorly-controlled hypertension group compared to the patients with well-controlled HT.
Combined treatment with anti-hypertensive drugs is advised instead of monotherapy with an antihypertensive agent in recent literature. Mahmud et al. reported that combined treatment was more effective than monotherapy in treatment of HT.25 In another study, it was found that combination treatment of HT was superior to treatment with a single agent in achieving blood pressure control.26 Similar to the literature, blood pressure levels were significantly lower in our study in patients on combined treatment compared to patients treated with a single agent. In conclusion, we suggest that, in addition to dietary and exercise recommendations and smoking cessation, treatment with combination therapy could improve the goals of reaching blood pressure targets in patients with HT.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES