KEYWORDS
Haemophagocytic lymphohistiocytosis, immune-mediated diseases, sarcoidosis, soluble IL-2 receptor, T-cell activation
INTRODUCTION
Interleukin 2 (IL-2) represents one of most significant cytokines in the immune system as it is involved in the regulation of protective immunity, as well as maintaining immune tolerance mediated by CD4+ regulatory T lymphocytes (Treg).1-3 IL-2 acts on cells that express either the trimeric high-affinity IL-2 receptor (IL-2R) or dimeric low-affinity IL-2R (figure 1). 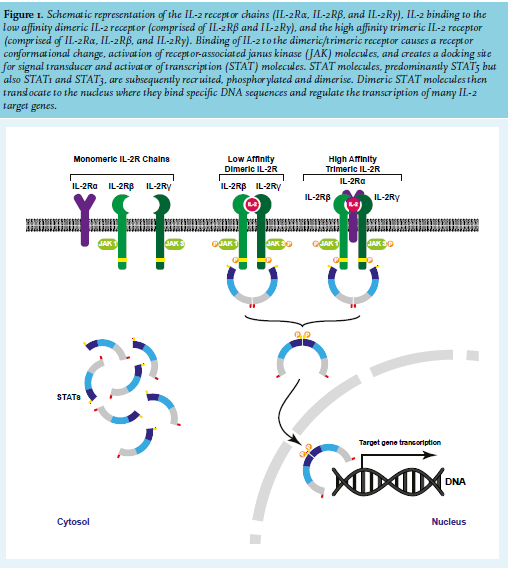
The dimeric low-affinity IL-2R consists of the IL-2Rβ chain (also known as CD122) and the cytokine receptor common γ-chain (γc, also known as CD132). The low-affinity dimeric IL-2R is hardly expressed by naive CD4+ T lymphocytes, expressed at low levels by naive CD8+ T lymphocytes and memory CD4+ T lymphocytes, and at high levels on memory CD8+ T lymphocytes and NK cells. Cells that express high levels of low-affinity IL-2R are susceptible to activation by IL-2 in vitro, yet this requires stimulation with (non)-physiological IL-2 concentrations.1,4 The third chain of the trimeric high-affinity IL-2R is IL-2Rα (also known as CD25 or TAC antigen). IL-2Rα does not actively participate in receptor signalling but rather, enhances the receptors affinity for IL-2. Tregs are characterised by strong constitutive expression of IL-2Rα which enables these cells to constantly express the high-affinity trimeric IL-2R (IL-2Rαβγ) and thereby use the low physiological level of IL-2 as is present in vivo.1 The high-affinity IL-2R is transiently expressed at high levels by activated CD4+ and CD8+ T lymphocytes. First, following signalling induced by T-cell receptor (TCR) activation and co-stimulatory molecules, IL-2Rα is induced to moderate expression levels which is subsequently further enhanced in a positive feedback loop through IL-2/IL-2R signaling.1,3,5 Rubin and colleagues were the first to demonstrate that after in vitro activation, T lymphocytes not only enhanced cellular IL-2R expression but also released soluble IL-2R(α),6 and similar to cellular IL-2R expression, the release of soluble IL-2R required de novo protein synthesis rather than cellular proliferation.6 Other studies demonstrated a significant correlation between surface membrane IL-2R expression on activated CD4+ and CD8+ T lymphocytes and the amount of secreted sIL-2R following in vitro activation.7 In addition, CD4+CD25+ Tregs were found to secrete sIL-2R upon in vitro activation with certain stimuli.8 Soluble IL-2R most likely originates from enzymatic cleavage and release from the cell surface membrane. Several enzymes, including neutrophil-derived elastase, matrix metalloproteinases-9, and the house dust mite protease Der p 1, have been proposed for cleavage of membrane IL-2Rα. 9-11 However, although the exact nature of the involved proteolytic factor(s) remains largely unknown, it is most likely endogenous to the sIL-2R-producing cell as suggested by occurrence of sIL-2R production under serum-free cell culture conditions.6,12 Since its initial in vitro description in 1985, elevated sIL-2R blood levels have been found in different pathological conditions, including autoimmune diseases, infectious diseases, transplant rejection, and malignancies.13-16 Associations between genetic variants in IL2RA (the gene encoding IL-2Rα) and autoimmune diseases have been described. However, correlating this directly to serum sIL-2R levels may be difficult given that sIL-2R is produced through membrane cleavage which, in turn, depends on several different processes which may be influenced by disease activity.17-22 Currently, sIL-2R is generally regarded as a marker of T-lymphocyte activation; however, the cellular source of sIL-2R may not be restricted to T lymphocytes as other types of activated immune cells, including monocytes, dendritic cells, and B lymphocytes may release sIL-2R as well.6,16,23-27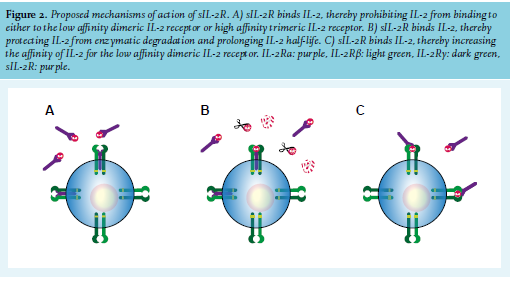
Despite the recognised association between immune activation and increased sIL-2R release under pathological conditions, the biological actions of sIL-2R are still far from understood. Several mechanisms of action, ranging from immune-inhibitory to immuno-stimulatory effects, have been proposed (figure 2). Soluble IL-2R binds IL-2 efficiently, and based on in vitro experiments, it has been proposed that sIL-2R may limit activation and proliferation of T lymphocytes by sequestration of available IL-2.1,27-30 However, conflicting data have been reported.8 Alternatively, sIL-2R complexed with IL-2 prolongs IL-2 half-life which may enhance the immune-stimulatory properties of IL-2, even by activation of low-affinity dimeric IL-2R.31,32 It has been proposed that IL-2 can be presented to CD4+ T lymphocytes through sIL-2R, which then induces differentiation into Tregs (rather than differentiation into T-helper (Th)1 or Th17 lymphocytes) that subsequently can suppress immune activity.33 On the other hand, there are reports to support observations that sIL-2R may promote (auto)immune processes in association with enhanced Th17 generation, which involves sequestration of the IL-2 that normally inhibits early Th17 differentiation.21,34 Although the exact mechanism(s) of action of sIL-2R, as well as their in vivo occurrence and final biological effects, remains to be determined, the data available so far do support a role for sIL-2R in regulating IL-2-dependent cell function.
SOLUBLE IL-2 RECEPTOR IN DISEASE AND CLINICAL PRACTICE
Elevated blood sIL-2R levels have been reported in a variety of human diseases, including autoimmune and inflammatory diseases, solid cancers, haematological malignancies, and infections.13-16 This clearly indicates the disease aspecificity of elevated sIL-2R. Nevertheless, serum sIL-2R measurement has increased substantially in routine clinical practice over the last decade. Below we discuss laboratory tests for sIL-2R and several conditions where serum sIL-2R measurement can be of clinical use.
Laboratory tests for soluble IL-2 receptor
To date, no gold standard technique and standard reference sera are available for sIL-2R measurement. Current available laboratory tests for sIL-2R comprise enzyme linked immunosorbent assays (ELISA) from different suppliers, but an automated immune assay based on chemoluminiscence (CLIA) is also available. A comparison between an ELISA (Diaclone, Besancon Cedex, France) and the automated Immulite chemiluminescent method (Siemens Healthcare, Germany), both commonly used by clinical laboratories in the Netherlands, is shown in figure 3. Although both detection systems report different absolute values in different units (pg/ml vs U/ ml) there is perfect correlation between both methods, with results differing by a factor of 6-7 in magnitude. Yet, comparison of the Immulite chemiluminescent method with ELISA from another supplier that uses different capture and detection antibodies could result in a different conversion factor. External quality control rounds revealed reproducible results comparing data of the same method.
From a practical point of view, it is important to note that sIL-2R measurements in serum and plasma yield comparable results and that sIL-2R levels remain stable at room temperature over a period of at least three days after sample collection (internal validation, Laboratory Medical Immunology, Department of Immunology, Erasmus MC, University Medical Center Rotterdam, the Netherlands). Also, up to three freeze-thaw cycles do not seem to affect sIL-2R concentration (personal experience). In healthy individuals, serum sIL-2R levels vary with age, with children and elderly (≥ 65 years) having higher levels than (young) adults.35-38 This illustrates that age-related references values are preferable when considering usefulness of serum sIL-2R levels for clinical assessment.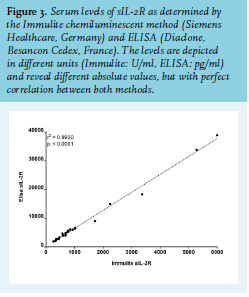
Haemophagocytic lymphohistiocytosis
Haemophagocytic lymphohistiocytosis (HLH) is a complex inflammatory and often very serious disease. Two different HLH forms exist. Primary HLH, also referred to as genetic HLH, has a typical disease onset during infancy or early childhood in individuals with gene mutations that hamper the cytotoxic function of NK cells and T lymphocytes. Secondary HLH tends to occur in older patients in association with another condition, most commonly malignancy, infection, autoimmune disease, and without an identifiable genetic abnormality.39-42 Despite the genetic difference between primary HLH and secondary HLH, the clinical manifestations (e.g., fever, hepatosplenomegaly, generalised lymphadenopathy, pancytopenia), and most likely the pathophysiological mechanisms involved, are highly comparable. Although the exact mechanisms are not always clear, it is currently thought that all forms of HLH result from impaired cytotoxic T-lymphocyte and NK-cell functioning. This cellular dysfunction prevents efficient antigen removal with subsequent uncontrolled immune activation with a cytokine storm (including IL-6, IL-18, IFN-γ, TNF-α), uncontrolled macrophage activation, and haemophagocytosis.39,43-45
Serum sIL-2R level is strongly elevated in both primary and secondary HLH and is considered to originate from excessively activated T cells.40,45-47 The updated criteria HLH-2004 from the Histiocyte Society included an elevated serum sIL-2R receptor (≥ 2400 U/ml, with a sensitivity of 93% and specificity of 100%) as an additional laboratory diagnostic criterium for paediatric HLH.48,49 However, relevant disease controls that most likely would have lowered specificity were lacking in the HLH-2004 study cohort.49 A slightly lower sensitivity (89%) for HLH was reported in another paediatric cohort when applying the HLH-2004 serum sIL-2R cut-off value.50 Currently the HLH-2004 guidelines contain the standard diagnostic criteria for paediatric HLH. Although developed for paediatric HLH, the HLH-2004 criteria are widely applied to patients with secondary HLH, including adults, as well. There is data to support that the HLH-2004 criteria may be inadequate to accurately diagnose HLH in adults.51,52 However, extending HLH-2004 with additional criteria may improve HLH diagnosis in adults, as was for instance, shown for malignancy-associated HLH.52 Nevertheless, serum sIL-2R has also been found to display a good to excellent diagnostic performance in diagnosing HLH in adults, with optimal sensitivity (100%) and specificity (72,5%) at a cut-off value of ≥ 2515 U/ml.53 Although this cut-off value is slightly higher than the 2400 U/ml described in the HLH-2004 criteria, the data do demonstrate that a serum sIL-2R level ≤ 2400 U/ml can be helpful in ruling out HLH in adults with high sensitivity (100%). Furthermore, a serum sIL-2R level > 10000 U/ml was found helpful for ruling in HLH in adults with high specificity (93%), but with limited sensitivity (45%).53 Currently, serum sIL-2R is considered a valuable tool in the diagnostic work-up of HLH, yet data on sensitivity and specificity are so far only available from a limited set of studies on paediatric and adult HLH. Establishing a cut-off value for most optimal diagnostic specificity requires further evaluation, especially when one considers the fact that elevated serum sIL-2R levels occur in many diseases, including different types of cancers, infectious conditions, and autoimmune diseases that can overlap, mimic, or trigger HLH.14-16,41,42,54 There are some reports that suggest that serum sIL-2R might be of use to distinguish the aetiology underlying HLH. For instance, higher levels of serum sIL-2R have been described in malignancy-associated HLH compared to HLH associated with infection or (auto)immune disease.53,55-57 However, comparable sIL-2R serum levels between malignancy-associated HLH and EBV-associated HLH have been reported.57 Moreover, a higher sIL-2R to ferritin ratio was described in lymphoma-associated HLH as compared to infection-associated HLH and autoimmune disease-associated HLH, but conflicting data exist.53,55,56 Likewise, it has been reported that HLH, in the context of (severe)combined immunodeficiency, presents with lower serum sIL-2R levels compared to primary HLH or infection-triggered secondary HLH in infants, which may clearly hamper diagnosing HLH in case of (severe) combined immunodeficiency. Yet, an elevated ratio of serum ferritin/sIL-2R was shown to distinguish HLH in patients with T-cell deficiencies from the other HLH types.58 Also, studies reported that primary HLH may present with higher serum sIL-2R levels compared to HLH of other aetiologies, and that the serum sIL-2R/ ferritin ratio can distinguish primary HLH from other types of HLH, although data on this is not consistent.50,58-60 Thus, although interesting, data to firmly support a role for serum sIL-2R in distinguishing between HLH types and aetiologies are limited and further studies on this are required.
In addition to its application in diagnosing HLH, serum sIL-2R measurement may also provide a tool to monitor disease activity as serum sIL-2R declines with clinical improvement.46,53,57,61-63 Alternatively, an increasing serum sIL-2R concentration has been associated with clinical deterioration.45,53,54 Moreover, higher initial sIL-2R serum levels (for instance ≥10000 U/ml or ≥ 20000 pg/ml) have been reported to be associated with decreased survival compared to HLH patients with lower serum sIL-2R, although data on this is inconclusive.53,57,64-66 Altogether these data indicate that serum sIL-2R represents a biomarker useful for at least HLH diagnosis as well as monitoring HLH disease activity and potentially prognosis.
Sarcoidosis
Sarcoidosis is a multisystem granulomatous disease of unknown aetiology presenting with a wide spectrum of clinical manifestations. The natural course of the disease is highly variable and the outcome difficult to predict. Symptom burden is high, and quality of life and social participation are negatively affected. In patients with pulmonary sarcoidosis, treatment is recommended in cases with significant symptoms and/or impaired or deteriorating lung function. The development and formation of noncaseating granulomas characterises the fundamental abnormality in sarcoidosis, with the lungs, lymph nodes, and skin being the most affected organs.67,68 Although granulomas may often resolve spontaneously, pulmonary fibrosis occurs in 10%-15% of patients with sarcoidosis. Granuloma formation is thought to be initiated by CD4+ T lymphocytes that interact with antigenpresenting cells, that become activated and differentiate into Th1 lymphocytes. CD4+ Th1 lymphocytes secrete predominantly IL-2 and IFN-γ and stimulate macrophage TNF-α production, ultimately leading to the characteristic fierce influx of CD4+ T lymphocytes into the involved organs.
A significant correlation was observed between serum soluble IL-2R values and the influx of T lymphocytes into the lungs by Grutters et al., who reported the absolute CD4+ T-lymphocyte numbers in bronchoalveolar lavage in 47 newly diagnosed sarcoidosis patients.69 Moreover, higher sIL-2R values were observed in sarcoidosis patients with more advanced and progressive disease, which may predict need for therapy, and high sIL-2R at therapy initiation could serve as a predictor of relapse after infliximab therapy.70-76 Furthermore, sequential measurements of serum sIL-2R could be useful to assess the evolution of disease activity in sarcoidosis. Vorselaars et al. found that decline in serum sIL-2R after six months of treatment with methotrexate correlated with improvement of pulmonary parameters.77
In patients with extrapulmonary sarcoidosis, serum sIL-2R was superior to the serum marker, angiotensin-converting enzyme (ACE) when used as screening tool for the detection of intra-ocular sarcoidosis in patients with uveitis.78,79 Moreover, Petereit et al. reported that sIL-2R measurements in the cerebrospinal fluid in patients with suspected neurosarcoidosis may help in the diagnostic work-up and may be used to monitor CNS disease activity.80 In contrast, in isolated cardiac sarcoidosis compared to non-isolated cardiac sarcoidosis, plasma sIL-2R levels were not elevated.81 The diagnostic value of sIL-2R for sarcoidosis was confirmed in a recent retrospective cohort study. In total, 189 patients suspected for sarcoidosis were analysed. The sensitivity and specificity of serum sIL-2R for detection of sarcoidosis was 88% and 85%, respectively, superior to ACE (62% and 88%).82 In 2015, the diagnostic criteria for sarcoidosis were updated in Japan by the Japanese Society of Sarcoidosis and Other Granulomatous Disorders (JSSOG), with elevated serum sIL-2R replacing negative tuberculin reaction.73 Although considered useful, serum sIL-2R measurement was not included in the recently revised International Workshop on Ocular Sarcoidosis (IWOS) criteria for diagnosing ocular sarcoidosis. The main reason being that it was considered that serum sIL-2R measurement is not (yet) used widely enough in uveitis clinics.83 Nevertheless, the data available so far do show that serum sIL-2R measurement represents a valuable biomarker in the diagnosis of sarcoidosis as well as for assessment of disease activity and for monitoring treatment efficacy.
Autoimmune disease and other immune-mediated diseases
Increased levels of serum sIL-2R have been described in a variety of autoimmune/immune-mediated diseases as well as other disease conditions associated with immune dysregulation (table 1).13-16,78,82,84-102 Of these, rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), juvenile idiopathic arthritis (JIA), adult-onset Still’s disease (AOSD), ANCA-associated vasculitis, and IgG4-related disease (IgG4-RD) will be discussed in more detail below. 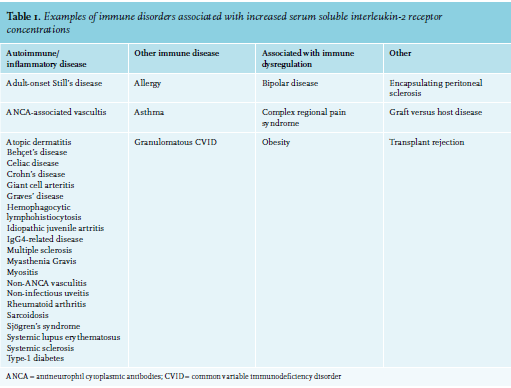
Rheumatoid arthritis (RA). RA is a chronic inflammatory joint disease that eventually results in destruction of cartilage and bone, severe disability and premature mortality. RA is considered an autoimmune disease associated with the production of autoantibodies, such as anti-cyclic citrullinated peptide (ACPA) and rheumatoid factor (RF).103,104 Classification as definite RA, using the ACR/EULAR classification criteria, is based upon the presence of synovitis in at least one joint and a total score of at least six points (of a possible 10) achieved in four domains. These domains are number and site of involved joints, serological abnormality (ACPA or RF), elevated acute phase response, and at least six weeks of symptom duration.105 Earlier reports in RA patients revealed conflicting results concerning the correlation between sIL-2R levels and disease activity scores or correlation with other laboratory markers of inflammation.16 More recently, Kuuliala et al. reported that low sIL-2R levels may be predictive of a rapid response to treatment with infliximab in patients with RA.106 However, in their cohort, the marker did not identify the patients in remission after 22 weeks. In addition, Steenbergen et al. reported that lower sIL-2R levels were associated with more disease-modifying antirheumatic drug-free sustained remission in RA.22
Systemic lupus erythematosus (SLE). SLE is a chronic, severely debilitating systemic autoimmune disease characterised by the production of autoantibodies and multi-organ inflammation. SLE is a multifactorial disease that results from complex interactions between susceptibility genes, epigenetic, environmental, hormonal, and immuno-regulatory factors and can present with a wide spectrum of clinical manifestations with unpredictable relapse-remitting course.107,108 SLE may involve almost all organs and tissues. Clinical manifestations may include fatigue, mucocutaneous lesions, renal involvement, arthritis, haematological abnormalities, serositis and fever. Newly developed 2019 EULAR/ACR classification criteria for SLE include positive antinuclear antibody (ANA) as entry criterion, followed by weighed criteria grouped in seven clinical domains (constitutional, haematological, neuropsychiatric, mucocutaneous, serosal, musculoskeletal, renal) and three immunological domains (antiphospholipid antibodies, complement proteins, and SLE-specific antibodies). Patients fulfil classification for SLE when accumulated ≥ 10 points.109
Elevated blood levels of sIL-2R occur in SLE and have been reported to precede major disease exacerbations.110-112 Also, significantly higher sIL-2R values are found in SLE patients with lupus nephritis compared to SLE patients without nephritis, and sIL-2R levels decline after treatment.113,114 Recently, Zhang et al. reported that SLE patients in the group with high sIL-2R values had significantly more lupus nephritis, arthritis, and vasculitis compared to SLE patients in the group with low sIL-2R values. Moreover, high sIL-2R values were significantly associated with laboratory parameters of renal impairment and Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K).115 Together, these data indicate that sIL-2R may be a useful biomarker for the assessment of SLE disease activity and might be used as early indicator of renal involvement. As T lymphocytes play a central role in most rheumatic diseases, it would be of interest to establish correlations between sIL-2R values and disease activity scores in other connective tissue diseases, e.g., systemic sclerosis and Sjögren’s disease.
Juvenile idiopathic arthritis (JIA). JIA is a heterogeneous group of diseases characterised by arthritis of unknown origin with onset before age of 16 years. The current International League of Associations for Rheumatology (ILAR) classification criteria for JIA were developed by consensus and not formally validated.116,117 The classification criteria recognise six mutually exclusive categories defined in clinical and laboratory measures: systemic arthritis, oligoarthritis (persistent or extended), polyarthritis rheumatoid factor (RF)-positive, polyarthritis RF-negative, enthesitis-related arthritis, psoriatic arthritis, and a seventh category, undifferentiated arthritis. Recently, an initiative was started to provide new evidence-based classification of JIA using a formal process to validate preliminary criteria.118
Elevated sIL-2R levels were found in patients with clinically active JIA compared to controls,119-121 and sIL-2R levels correlated significantly with pannus thickness and joint count.120,121 Furthermore, in addition to other disease characteristics, treatment-refractory disease course may be associated with a higher sIL-2R level.122 Finally, macrophage activation syndrome (MAS) has been increasingly recognised in association with rheumatic diseases, most commonly in systemic JIA. The clinical features of MAS in JIA are similar to HLH and include high, non-remitting fever, generalised lymphadenopathy, hepatosplenomegaly, central nervous system dysfunction, and haemorrhagic manifestations and can result in multi-organ failure.123 Recent reports suggest that (subclinical) MAS in systemic JIA may even occur in 30-40% of patients.124,125 The utility of serum sIL-2R for JIA will probably vary per clinical phenotype, but, serum sIL-2R may be a promising marker for disease activity in systemic JIA, especially when associated with MAS.124
Adult-onset Still’s disease (AOSD). AOSD is a rare systemic inflammatory disorder characterised by high fever that typically spikes once or twice daily, a transient salmon pink skin rash (mostly on the proximal limbs and trunk) that occurs along with the fever spikes, arthritis and arthralgia involving predominantly the wrists, knees and ankles, and frequently a sore throat; as well as less frequent symptoms including myalgias, lymphadenopathies, splenomegaly, hepatomegaly, pleurisy, pericarditis, weight loss, and abdominal pain.126,127 The pathophysiology of AOSD is mainly unknown, but involvement of a pro-inflammatory cascade that can be triggered by infectious agents, solid cancers, or lymphomas in genetically predisposed individuals has been proposed.126,127 AOSD shares several phenotypic characteristics with systemic JIA, including daily recurring fever, salmon-coloured skin rash and polyarthritis, and is considered to represent the adult counterpart of systemic JIA or even a continuum of a single disease entity.127,128
No definitive diagnostic tool for AOSD exists and its diagnosis is based on extensively excluding diseases with comparable clinical presentation (including, for example, viral and bacterial infections, SLE, RA, myositis, systemic vasculitis, autoinflammatory diseases, sarcoidosis, malignancies), for which several diagnostic criteria sets have been developed.127 Laboratory findings reflect the (non-specific) systemic inflammatory nature of the disease and increased erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels, neutrophilic leucocytosis (> 80% polymorphonuclear leucocytes), anaemia and thrombocytosis are common findings. Also, serum ferritin is highly elevated in AOSD, while glycosylated serum ferritin is typically low.126,127 Neutrophil and macrophage activation are at the centre of the immunopathogenesis of AOSD and macrophagederived pro-inflammatory cytokines such as the interleukin-1 family members IL-1β and IL-18, as well as IL-6, are centrally involved.126,127 AOSD is also strongly associated with secondary HLH and cytotoxic functions of NK cells are diminished in active AOSD.126,127,129,130
Also, increased IFN-γ-producing Th1 lymphocytes have been detected in peripheral blood and pathological tissues from patients with active untreated AOSD, which likely contributes to further macrophage activation and cell-mediated immunity.126,127,131 In addition, circulating Th17 lymphocytes were found elevated in patients with active untreated AOSD.132 Frequencies of circulating Th1 and Th17 lymphocytes correlated significantly with clinical activity, and serum IL-18 and ferritin levels in active untreated AOSD, and all these laboratory parameters declined with clinical remission upon treatment.131,132 Only limited data on serum sIL-2R in AOSD is available, yet increased levels are detected in active AOSD, thus further supporting T-lymphocyte involvement in this disease.131,133-137 Although AOSD may not display differences in serum sIL-2R levels compared to other diseases, serum sIL-2R level may represent a potential biomarker for monitoring AOSD disease activity and treatment response.136 Serum sIL-2R levels have been reported to correlate with AOSD disease activity.133,135,137 Moreover, Fuji et al. reported that serum sIL-2R levels were higher in the subgroup of AOSD patients with chronic articular disease, suggesting that serum sIL-2R levels may distinguish between different AOSD disease patterns.135 Also, several studies demonstrated that upon treatment, disease remission was associated with a strong decline in serum sIL-2R levels, along with decreases in other laboratory parameters such as ESR, CRP, ferritin, and IL-18 levels.131,134,135,137,138 In contrast, a rise in serum sIL-2R level can occur in case of disease recurrence.137 Altogether, the data available so far suggest that serum sIL-2R can be considered as an additional biomarker to monitor AOSD disease activity and therapeutic response.
ANCA-associated vasculitis (AAV). AAV is a necrotising vasculitis that predominantly affects small vessels and is associated with antineutrophil cytoplasmic antibodies (ANCA) specific for myeloperoxidase (MPO-ANCA) or proteinase 3 (PR3-ANCA). The major clinicopathological variants of AAV are microscopic polyangiitis (MPA), granulomatosis with polyangiitis (GPA), and eosinophilic granulomatosis with polyangiitis (EGPA). Besides necrotising vasculitis, GPA and EGPA show necrotising granulomatous inflammation often involving the respiratory tract. Moreover, EGPA is associated with asthma and eosinophilia.139 Clinical manifestations that suggest the diagnosis of AAV, when there is no other obvious cause, and indicate ANCA testing include: (rapid progressive) glomerulonephritis, pulmonary haemorrhage, cutaneous vasculitis with systemic features, multiple lung nodules, chronic destructive disease of the upper airways, long-standing sinusitis or otitis, subglottic tracheal stenosis, peripheral neuropathy, retro-orbital mass, and scleritis.140
Elevated levels of sIL-2R have been detected in the sera of patients with GPA and MPA. Moreover, sIL-2R levels correlated with disease activity at diagnosis and differed between limited and generalised and between active and inactive disease.141-144 In addition, positive ANCA serology during follow up was associated with sIL-2R levels. At 18 and at 24 months after diagnosis, higher levels of sIL-2R were found in ANCA-positive patients compared to patients negative for ANCA.142 Analogous to sIL-2R as marker for T-cell activation, soluble CD163 (sCD163) is considered a systemic marker of macrophage activation. CD163 is abundantly expressed by tissue macrophages and is shed from the macrophage surface under inflammatory conditions by ADAM17, the enzyme that also releases TNF into the circulation.145,146 It has been reported that urinary sCD163 levels may reflect active glomerular inflammation.147 Dekkema et al. found that measurement of serum sIL-2R, in addition to urinary sIL-2R, complements urinary sCD163 in the detection of active renal vasculitis in AAV patients and that serum and urinary sIL-2R are significantly higher during active renal disease and decline upon remission.148 Taken together, these data show that sIL-2R may be a valuable biomarker for assessment of disease activity and for monitoring treatment, and seems to reflect the central role of the T-lymphocyte-driven immune response in ANCA-associated vasculitis.
IgG4-related disease (IgG4-RD). IgG4-RD is a fibroinflammatory disease that can involve various organs, including the lungs, thyroid, lymph nodes, orbital tissue, kidneys, salivary and lacrimal glands, aorta, pancreas, and skin. IgG4-RD is characterised by accumulation of IgG4-producing plasma cells at affected sites, along with the formation of storiform fibrotic lesions.149 Serum IgG4 levels are elevated in the majority of patients with IgG4-RD, yet IgG4 elevation is not fully sensitive or specific for diagnosing IgG4-RD.149 Moreover, serum IgG4 levels may not always accurately reflect disease activity.150,151 Therefore, additional blood biomarkers for improved diagnosis and evaluation of IgG4-RD disease activity are still needed.152,153 To date, only a limited number of studies have explored serum sIL-2R in relation to IgG4-RD. These studies report elevated serum sIL-2R levels in IgG4-RD, a positive correlation between serum sIL-2R levels with the number of affected organs as well as disease activity.90,154,155 Moreover, these studies reported a decline of serum sIL-2R levels after treatment.90,154,155 In addition, serum sIL-2R levels have been reported to display high accuracy in predicting an individual glucocorticoid requirement.155 These data indicate that serum sIL-2R level may be a valuable biomarker for evaluating disease activity and treatment response in IgG4-RD. However, additional (prospective) studies are needed, especially with regard to treatment stratification, monitoring treatment response, as well as sensitivity and specificity of sIL-2R in the context of IgG4-RD diagnosis.
Cancer and treatment
Increased serum sIL-2R levels have been found in a variety of malignancies, mostly haematopoietic malignancies but also solid cancers.13-16 These elevated sIL-2R levels most likely derive from the malignant cells, although the host cellular immune response likely contributes to the generation of sIL-2R as well.13-15 Immune checkpoint inhibitor treatment is a rapidly expanding field within oncology. High serum sIL-2R in metastatic melanoma patients before initiation of ipilimumab (anti-CTLA-4) treatment has been associated with treatment resistance, most likely by IL-2 sequestration.156 Despite the anti-tumour efficacy of immune checkpoint inhibitor treatment, secondary development or worsening of autoimmune/inflammatory disorders is commonly observed in cancer patients upon such treatment.157 Measurement of serum sIL-2R prior and during therapy, potentially along with other cytokines such as IFN-γ, IL-17, and IL-10, may, in the future, prove a valuable tool for monitoring excessive/uncontrolled immune activation and to predict the development of immune-related adverse events in cancer patients treated with immune checkpoint inhibitors.157
CONCLUDING REMARKS
The clinical utility of sIL-2R, as reviewed above, lies particularly in evaluating disease activity in a variety of immune-mediated diseases and may add in the diagnostic work-up of especially HLH and sarcoidosis. As sIL-2R level reflects activation status of the T-lymphocyte compartment, its disease specific value is limited. However, in immune-mediated diseases where T-lymphocyte responses play a central role in the pathophysiology, sIL-2R might be a valuable biomarker for predicting or monitoring the efficacy of immune suppressive therapies.
DISCLOSURE
All authors declare no conflicts of interest. No funding or financial support was received
REFERENCES