KEYWORDS
Atypical presentation, ICU, pneumococcal infection
INTRODUCTION
Streptococcus pneumoniae is a Gram-positive bacterium and a coloniser of the upper respiratory tract. Common clinical manifestations of pneumococcal infections are acute otitis media, pneumonia, and meningitis. However, uncommon manifestations like infections of bone and joint or manifestations affecting the cardiovascular, gastrointestinal, and (uro)genital tract have been described.1 Invasive pneumococcal disease (IPD) is defined as positive culture of material from a normally sterile body site (e.g. blood, cerebrospinal fluid, pleura, joint, pericardium).
Pneumococcal disease has a significant burden on mortality and healthcare budget,2-4 however since the beginning of the 21st century conjugate vaccines have been used to diminish this burden. A decreasing incidence of IPD predominantly in children, ensued the implementation of PCV10 (10-valent pneumococcal conjugate vaccine, directed against serotypes 1, 4, 5, 6B, 7F, 9V, 14, 18C, 19F, and 23F) in the paediatric immunisation program.5 Because children are a reservoir for circulating pneumococci, their immunisation also confers herd immunity in the adult population.6
However, existing conjugate vaccines target up to 13 out of more than 95 known pneumococcal serotypes. In most adult populations, the vaccine-mediated reduction in IPD has now been replaced by non-vaccine serotypes.7-12 Several studies suggest that this shift in causative serotypes also affects clinical manifestations of diseases.13-16
It is well known that pneumococcal disease has a seasonal distribution like other respiratory infections, with the highest prevalence in autumn and winter. Temporal associations with seasonal respiratory viruses are described in the literature and pneumococcal superinfections to influenza have been studied in vitro and in animal models.17-20
During the respiratory season of 2017-2018, an unusually high number of patients with notable pneumococcal infections was admitted to the intensive care unit (ICU) of our tertiary care centre. In this paper, we present a case series of severe pneumococcal infections and highlight five cases with either uncommon or fulminant manifestations of pneumococcal disease.
METHODS
Case identification and reporting
We searched the hospital digital patient data system and the clinical microbiology data system for adult patients admitted to mixed medical and surgical ICUs of our academic tertiary care centre with a confirmed or suggested invasive pneumococcal infection between September 1st, 2017 and April 30th, 2018. Patients were considered eligible if S. pneumoniae was identified in cultures, or by PCR on materials from normally sterile body sites, or by a pneumococcal antigen test (PAT) (Alere Binex Now, Abbott, USA) on urine at the hospital’s clinical microbiology laboratory. In addition, patients referred from other hospitals were identified by text mining of electronic patient records from patients who had been admitted to the ICU during the study period, on synonyms of S. pneumoniae infection (Software: CTcue, Amsterdam, the Netherlands). Synonyms included any phrase containing pneumokok, pneumococ, Streptococcus pneumoniae, S. pneumoniae, or S.pneumoniae, and all hits were verified manually. Only medical cases with evident pneumococcal aetiology as the main reason for ICU admission were included, excluding patients who were temporarily monitored in the ICU, e.g., for diagnostic procedures (such as bronchoscopy or pericardial drainage). We reviewed patient records and summarised characteristics of individual cases. Serotyping of cultured pneumococcal isolates was performed at the Netherlands Reference Laboratory for Bacterial Meningitis by Quellung reaction. Five cases with atypical or fulminant disease are described in detail.
There is a lack of literature reports on pneumococcal IPD manifestations in the ICU. As a best alternative to appraise our observed distribution of clinical manifestations and mortality, we compared our data to a cohort of all adult pneumococcal bacteraemia cases admitted to the ICU of the neighbouring and a major referring secondary care training hospital (Canisius-Wilhelmina Hospital, Nijmegen, the Netherlands) between 2001 and 2015. For this comparator cohort, details on inclusion criteria, data collection, and representativeness of cohort characteristics (including serotype distribution) for the Dutch population were previously described elsewhere.21
CASE SERIES
Case 1: Meningitis
Patient 1 was a 48-year-old man admitted to the ICU with septic shock and meningitis. His medical history listed hypertension and type 2 diabetes mellitus. Two days before admission, symptoms started with an earache. The day before admission, the patient was nauseous and later disoriented. There was no history of fever or meningeal irritation. On the day of admission, the patient was found unresponsive with urinary and faecal incontinence. A Glasgow Coma Scale (GCS) of 6 with uniformous and responsive pupils were reported on presentation and patient was promptly intubated and sedated by the mobile medical team at his home.
Computed tomography (CT) at the emergency room (ER) showed findings suggestive of left-sided mastoiditis with transverse sinus thrombosis. Relevant blood analysis showed signs of an infection with leucocytosis (31x109/l) and elevated C-reactive protein (192 mg/ml). Blood gas analysis showed a combined metabolic-respiratory acidosis with impaired oxygenation (pH 6.98; partial pressure of carbon monoxide (pCO2) 7.3 kPa; partial pressure of oxygen (pO2) 10.2 kPa; bicarbonate (HCO3-) 10.4 mmol/l; lactate > 15 mmol/l). Blood cultures were taken and empirical antimicrobial therapy was started for suspected meningitis with amoxicillin 2000 mg intravenous (IV) three times a day and ceftriaxone 2000 mg IV two times a day (BID), according to hospital guidelines. After admission to the ICU, a lumbar puncture was performed. Opening pressure was > 50 cmH2O. Cerebrospinal fluid (CSF) showed 1243 leucocytes/µl (98% neutrophils), protein 3508 mg/l, glucose 2.0 mmol/l (glucose ratio CSF/blood 0.11) and L-lactate 26,260 µmol/l. Gram stain showed Gram-positive cocci in pairs and pneumococcal antigen testing on liquor was positive, after which antibiotic treatment was de-escalated to ceftriaxone monotherapy (because of selective decontamination of the digestive tract, a third generation cephalosporine was given). Nonetheless respiratory status deteriorated and the patient was placed in a prone position. After several hours, both pupils became unresponsive and dilated; a second CT scan of the head showed diffuse swelling of the brain. On the second day of admission, sedation was stopped. GCS remained 3 on day three with the absence of brain stem reflexes. It was decided to withdraw treatment because of a very poor prognosis. Both blood and cerebrospinal fluid cultures yielded growth of S. pneumoniae.
Case 2: Peritonitis
Patient 2 was a 38-year-old woman with a medical history of epilepsy, autoimmune pancreatitis, and hepatitis with chronic liver failure. Two days before admission to the ICU, she underwent an endoscopic ultrasound procedure to perform a biopsy of the pancreas. The day after, she complained of severe abdominal pain and was admitted to the hospital. An ultrasound-guided puncture for ascites was performed and cultures were taken. A CT scan showed signs of hepatic ischaemia, an oedematous pancreas and signs of duodenitis, jejunitis, and colitis. Antibiotic treatment was initiated promptly with ceftriaxone 1000 mg IV every day (QD), metronidazole IV 500 mg QD, teicoplanin 12 mg/kg IV BID (to cover Enterococcus spp) and anidulafungin IV 100 mg QD (as empirical choice for potential invasive candidiasis). The patient was admitted to the ICU two days after the endoscopic procedure with sepsis and liver failure. An exploratory laparotomy was performed revealing a diffusely ischaemic jejunum and colon. Because of the extent of the ischaemic lesions, no resection was performed; the abdomen was left open because of high intra-abdominal pressure. The patient developed multiple organ failure (MOF). Culture from the abdominal fluid (ascites) showed S. pneumoniae and antibiotic treatment was de-escalated to penicillin 6,000,000 U/day. At ICU day 15, severe rectal blood loss occurred from a rectal ulcer. Because of a lack of treatment options and progression of multiple organ failure, palliative therapy was started. The patient died on day 17.
Case 3: Pneumonia, pleural empyema, pericarditis
Patient 3 was a 68-year-old man with a medical history of a chronic pancreatic insufficiency and a transient ischemic attack (TIA) eight years before admission. The patient was transferred to our ICU after he had been treated for severe pneumonia in another hospital for seven days. He was mechanically ventilated from admission and his stay was complicated by recurrent atrial fibrillation/flutter and cardiogenic shock because of cardiac tamponade. Percutaneous pericardial drainage was performed in the referring hospital without apparent effect. Loculated pleural fluid was present bilaterally and a pleural drain had been placed in the left pleural cavity. Blood cultures were positive for S. pneumoniae.
On admission to our hospital, the patient was treated with cefotaxime 1000 mg IV QID. The same evening, a surgical subxiphoidal pericardial drainage was performed. Antibiotic treatment was de-escalated to penicillin 12,000,000 U/day. A sternotomy was performed two days after primary drainage during which, pericardial adhesions were dissected and a partial pericardiectomy was performed, and pleural spaces were opened with debridement of pleural adhesions. Soon thereafter however, the patient developed progressive MOF and it was decided to withdraw active treatment. Patient died on day 11 after primary admission. While pleural and pericardial fluids remained culture-negative, the presence of S. pneumoniae in these specimens was later confirmed by PCR.
Case 4: Meningitis, endocarditis
Patient 4 was a 67-year-old woman with a medical history of hypertension, hypercholesterolaemia, type 2 diabetes mellitus, and irritable bowel syndrome (IBS). The patient was admitted to the ICU of the referring hospital with a GCS of 9, a fever of 40 °C, and hypotension. She had reported pain in her left shoulder. The day before admission, she had become acutely ill with pain spreading to her left leg; she also had pollakisuria and mild diarrhoea. A lumbar CSF puncture showed an increased pressure (> 50 cm H2O), high glucose, high protein, high leucocyte count, all compatible with bacterial meningitis. Blood and CSF cultures revealed S. pneumoniae. Antibiotic treatment with penicillin 12,000,000 U/day was started. The next day, her neurological status improved. However, there were signs of a recent myocardial infarction on electrocardiography. A screening echocardiogram showed a moderate left ventricular function. Patient had two episodes of acute congestive heart failure and she developed atrial fibrillation. A follow-up echocardiogram showed vegetations on the mitral valve. The patient was intubated and a transoesophageal echocardiogram showed vegetations on both the mitral and aortic valves. Antibiotic treatment with benzylpenicillin 12,000,000 U/day was continued based on the pneumococcal isolate minimum inhibitory concentration of benzylpenicillin of 0.016 mg/l. Because of the poor clinical condition, acute surgical treatment was decided against and conservative treatment with antibiotics was continued. The third day after referral, the patient was extubated and transferred to the ward. A magnetic resonance imaging of the cerebrum showed multiple lesions consistent with infarctions, compatible with septic embolism. Because her condition improved, a mitral valve replacement and coronary artery bypass graft were performed almost one month after first hospitalisation. Culture of the native mitral valve showed no bacterial growth. During hospitalisation, hypogammaglobulinaemia was found, which may have increased the patient’s susceptibility for the invasive pneumococcal infection. Gamma globulin treatment was started and continued at home. The antibiotic regime was continued for six weeks.
Case 5: Pneumonia
A 26-year-old woman was transferred to our ICU for venovenous extracorporeal membrane oxygenation (VV-ECMO). She had a medical history of exercise-induced asthma, allergic rhinitis, and migraines. One day earlier, she was admitted to the referring ICU with bilateral pneumonia after she had been ill for a week. The general practitioner had prescribed steroids for asthma exacerbated by a (suspected) viral infection. She was intubated for acute respiratory failure. The following day, she was transferred to our hospital with persistently high respiratory support. Empirical antimicrobial treatment included ciprofloxacin, ceftriaxone, and oseltamivir. After starting prone positioning, respiratory support could gradually be reduced and ECMO support was not required after all. Pneumococcal urinary antigen test was positive, as well as blood cultures showing S. pneumoniae. A PCR for influenza A was also positive. Treatment was de-escalated to benzylpenicillin 6,000,000 U/day. During admission, a chest CT scan showed a cavitation in the middle lobe without signs of abscess or of an empyema. Aspergillus fumigatus was cultured in a respiratory surveillance specimen; anidulafungin 100 mg QD and voriconazole 160 mg BID were started for suspected influenzaassociated invasive aspergillosis. Her respiratory status improved and just over two weeks after admission to our ICU, she was transferred back to the referring ICU. At that point, she was still intubated and on pressure support ventilation, receiving anidulafungin and voriconazole as antimicrobial therapy.
RESULTS
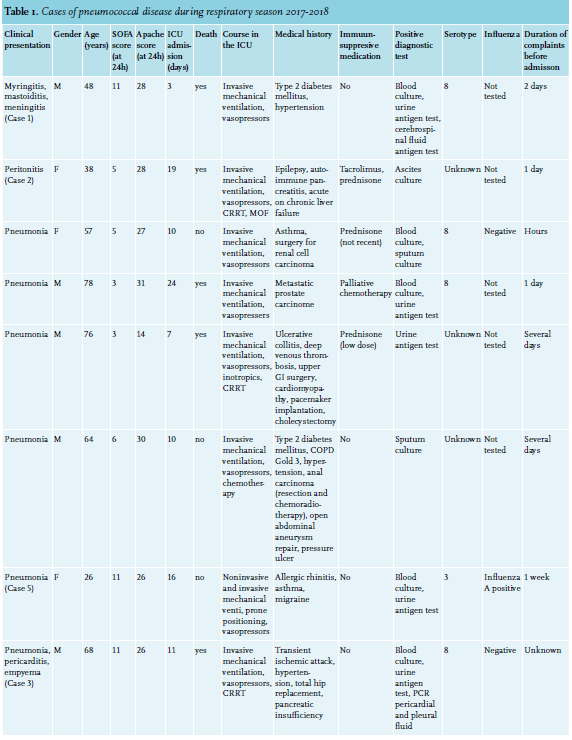
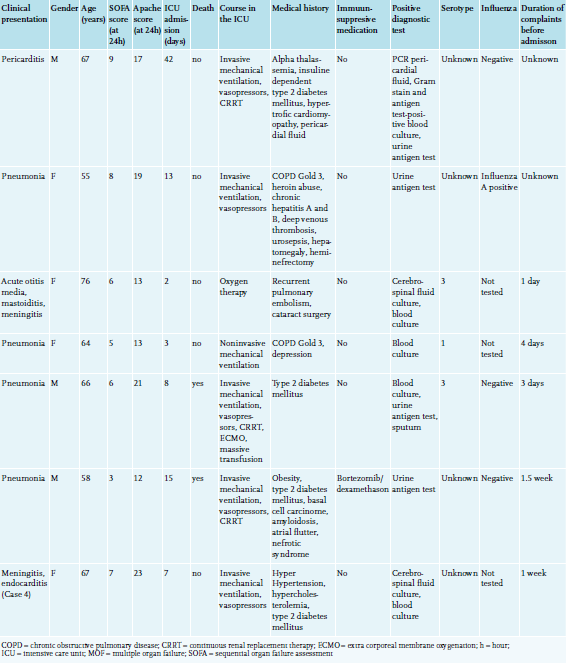
Fifteen cases met our inclusion criteria; 10 from in-house microbiology results and five solely by text mining (table 1). Their age ranged from 26 to 78; eight patients were younger than 65 years old. Eight patients were male and seven patients were female. The mortality in our cohort was 47%.
In three cases, only a pneumococcal urinary antigen test was positive; in one case, only sputum culture. In one case of pericarditis, pneumococcal aetiology was established by PCR on pericardial fluid in combination with a positive pneumococcal antigen test on both urine and a non-determined positive blood culture. In all other cases, S. pneumoniae was cultured from blood, cerebrospinal fluid, or ascites. All cultured pneumococci were susceptible for penicillin. In five patients, PCR on influenza was performed; two patients tested positive for type A influenza. Interestingly, the 2017-2018 influenza season was dominated by type B influenza.
In our population, 11 out of 15 patients had one or more known risk factors such as chronic lung disease (COPD more than asthma), smoking, diabetes mellitus, or chronic heart disease, predisposing them to invasive pneumococcal disease. Two patients had two risk factors. However, three out of seven patients who died had none of these risk factors. Five patients had been treated with some form of immunosuppressant medication. In one patient, severe hypogammaglobulinaemia was identified, making the patient more susceptible to pneumococcal infections. Vaccination status could not be retrieved in any of the patient records. In our cohort, seven out of eight serotyped isolates were non-PCV10 serotypes (table 1).
In our study period of 2017-2018, we observed relatively many uncommon clinical manifestations in our own ICU, in comparison to 138 adult bacteraemic IPD cases admitted to the ICU of a neighbouring secondary care hospital during 15 preceding years (figure 1). None of the seven external patients referred to our academic ICU during the current study period came from the comparator hospital. Mortality was 47% (7 out of 15) in our cohort, compared to 28% (38 out of 135) in the preceding cohort. In the preceding cohort, deaths were significantly older than survivors (mean of 69 versus 62 years old, respectively), and were mainly attributable to pneumonia, meningitis, and patients with an unknown focus of infection (23, 6, and 9 cases, respectively). Although in the current study cohort both deaths and survivors were relatively young (62 and 60 years old, respectively), mortality was particularly high among pneumonia cases (4 out of 9, compared to 23 out of 96 in the preceding cohort).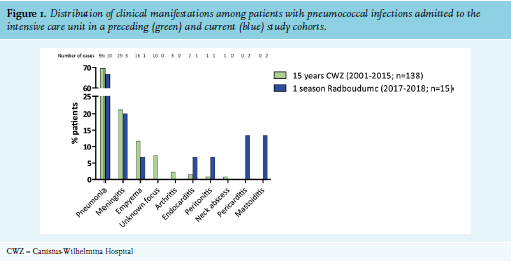
DISCUSSION
Our case study describes an unusual number of atypical manifestations and/or fulminant character of pneumococcal infections during the 2017-2018 autumn and winter months in a tertiary care ICU. In our cohort, almost all serotyped isolates were non-PCV10 serotypes, which corresponds with replacement of infections by non-vaccine serotype pneumococci and matches IPD surveillance in Europe and the Netherlands, reporting 86% to 90% non-PCV10 serotype IPD, with major serotypes 8 and 3.4,19 With serotypes, clinical presentation may change over time. We admitted a notable and unusually high number of severe pneumococcal infections, and comparison of our data with a neighbouring ICU suggests an increase in severe and atypical presentations over time. We report a relatively high mortality rate of 47% in 2017-2018 compared to preceding Dutch IPD cohorts; 28% in the secondary care ICU population in 2001-2016, and 13% in the general adult population 2008-2012.14,22 IPD mortality rates in an ICU setting were 14 to 29% for pneumonia cases, and 25% for meningitis cases.23-25 The sole study reporting on a comparable IPD case mix in ICU stems from 1983, where mortality was 76%.26 In our cohort, three serotyped deadly infections concerned non-vaccine serotype 8, which, since 2013,27 is the most common serotype in the Netherlands and more recently throughout Europe.28
Two previous studies reported that the rise in non-vaccine serotypes predominantly affected immunocompromised hosts, in addition to the elderly.13,29 Most patients were over 65 years old in our cohort, but several patients were younger. Also, patients with few risk factors contracted severe pneumococcal disease. As it is sometimes a previously unknown risk factor, it may be worthwhile to screen for immunodeficiency in these cases.
In the group of typical presentations, most patients presented with pneumonia; mortality (4/9) seemed somewhat higher than the 24% in the preceding neighbouring ICU cohort or the 14-29% reported elsewhere previously.23-25 We had two patients with pneumococcal meningitis, of whom, one patient died after a short course of disease.
Pneumococcal pericarditis is an unusual but severe complication of pneumococcal infection with high mortality rates.30-32 In one multinational prospective study, cardiac complications were reported in 1% of 844 patients with S. pneumoniae bacteraemia carrying a mortality rate of 25%. In our cohort, 20% of patients developed cardiac complications with a mortality rate of 33%. Interestingly, recent reports found evidence of invasion of S. pneumoniae into the myocardium in animal models, which disrupts cardiac muscle function leading to arrhythmias and heart failure.33,34
Pneumococcal peritonitis is also a rare manifestation of pneumococcal infection. Spontaneous (primary) pneumococcal peritonitis occurs in patients with underlying liver cirrhosis and is reported in association with respiratory tract infections.35-36 Secondary peritonitis is described with appendicitis or with genitourinary tract infection related to, for example, intrauterine tract devices.35 In our cohort, one patient had pneumococcal peritonitis after an endoscopic procedure. Her medical file did not mention any respiratory symptoms. In immunodeficient patients, secondary pneumococcal infection has been described after endoscopy or variceal bleeding.
Regarding the diagnosis of pneumococcal disease, 11 of our cases cultures (blood, ascites, CSF, sputum) were positive for pneumococci. In seven cases, non-culture-based tests were found positive (PAT, PCR). Moreover, in four cases, these tests were not supported by a concomitant positive culture. This emphasises the increasingly important role of PAT and PCR testing in diagnosing pneumococcal disease. A major limitation to our study is the retrospective single-centre design. For data collection, we depended on the accuracy of the electronic patient file.
As our results hint at a change in the severity of presentation of pneumococcal infections, a prospective systematic clinical registry for severe (invasive) pneumococcal infections might help to clarify trends in disease manifestations, serotype distributions, risk factors, and outcomes.
CONCLUSION
We report a case series of pneumococcal infections in adults with extreme disease manifestations. While our data are not representative enough to suggest a trend in increasing disease severity, interesting differences are seen when compared to a historical cohort from a neighbouring hospital. Given ongoing changes in infecting serotypes, a systematic clinical registry of pneumococcal infections in the ICU may be a valuable addition to pneumococcal disease surveillance.
ACKNOWLEGDEMENTS
We would like to thank Marien de Jonge and Tim Frenzel for their participation.
DISCLOSURE
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES