KEYWORDS
Cancer, mortality, prehospital antibiotics, readmission, sepsis
INTRODUCTION
Sepsis is a syndrome which often leads to high morbidity and mortality.1-3 Although absolute mortality has decreased in recent years, incidence is still rising. Several factors are associated with increased mortality in septic patients, including age, gender, presence of organ dysfunction, and active cancer.
Retrospective studies in the last decade have found that early treatment with antibiotics is associated with better outcomes in sepsis patients,4,5 although a recent prospective study found no benefit of prehospital antibiotics on overall survival (PHANTASi). The Surviving Sepsis Campaign currently recommends antibiotic treatment within one hour after arrival at the hospital.6 However, whether early antibiotics administration lead to better outcomes in all sepsis patients is a matter of debate.7,8
Several studies have investigated the epidemiology of sepsis in patients with cancer.9-12 The diagnosis of infection in this cohort is difficult as its early signs and symptoms are mimicked by non-infective causes, including the cancer itself and responses to systemic anti-cancer treatment (SACT).13,14 Retrospective studies in this sub-group of patients have shown that this population may benefit from early treatment with antibiotics.15-17 Multiple studies have been conducted in septic cancer patients with neutropenia and shown that delay in administration of the first dose of antibiotics, as well as pneumonia and thrombocytopenia, were risk factors for severe complications.12 The aim of this study was to evaluate whether septic patients with cancer have a different survival rate compared to non-cancer patients, who have reached the emergency department (ED) by ambulance. In addition, we investigated the effect of early antibiotics administration in these two sub-groups on patient outcomes.
MATERIALS AND METHODS
Design and setting
A sub-analysis was conducted using the PHANTASi (PreHospital ANTibioitcs Against Sepsis) trial database.7,18, In this randomised controlled, open-labelled trial, we investigated whether improved recognition of sepsis and administration of antibiotics in the ambulance led to increased survival when compared to usual care (fluid resuscitation and supplementary oxygen). Patients under usual care received their first dose of antibiotics at the ED. Between June 2014 and June 2016, eligible patients who were transported to one of the 34 participating hospitals in the Netherlands were enrolled. Sepsis was defined as: a diagnosed or suspected infection, a temperature of > 38°C or < 36°C, and a minimum of one other Severe Inflammatory Response Syndrome (SIRS) criterion (heart rate > 90 beats per minute or a respiratory rate > 20 per minute). Due to the lack of prehospital leucocyte test, this was not used as an inclusion criterion. Sepsis severity was categorised into three groups according to the 2001 SSCM/ ESCIM/ ACCP/ ATS/ SIS International Sepsis definitions Conference guidelines:19 uncomplicated (non-severe) sepsis, severe sepsis, and septic shock. Data collection methods have been described elsewhere.7 In short, data were collected by emergency medical services (EMS) personnel and the PHANTASi trial investigators. Variables collected included patient demographics, comorbidities, sepsis severity, mortality, and length of stay, among others. Infection site and microbiological data was also retrieved. The case record form has been published elsewhere.7
Methodology
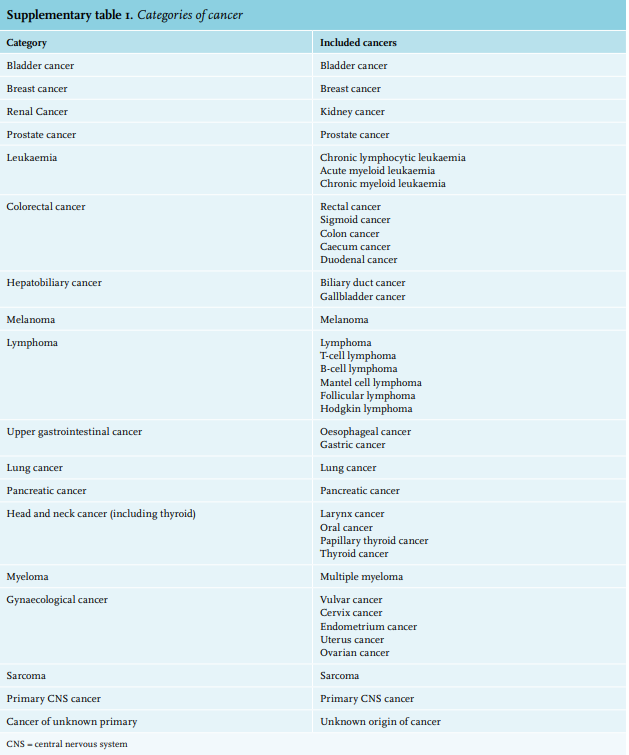
A total of 2,658 patients were included in the PHANTASi trial. In this post-hoc review, we compared patients who had any type of cancer in the past five years to those who were cancer free. Patients who had benign neoplasms in the past five years were categorised into the latter group. Cancers in our study were categorised into 18 categories: (1) bladder cancer, (2) breast cancer, (3) renal cancer, (4) prostate cancer, (5) leukaemia, (6) colorectal cancer, (7) hepatobiliary cancer, (8) melanoma, (9) lymphoma, (10) upper gastrointestinal cancer, (11) lung cancer, (12) pancreatic cancer, (13) head and neck cancer, including thyroid cancer, (14) myeloma, (15) gynaecological cancer, (16) sarcoma, (17) primary central nervous system (CNS) cancer, and (18) cancer of unknown primary origin. An overview of cancer types that were included in each category can be found in the appendix in PDF (supplementary table 1)*
Statistical analysis
The primary outcome of this study was 28-day mortality. Secondary outcomes included in-hospital mortality, 90-day mortality, focus of infection, time to antibiotics before arrival at the ED, time to antibiotics after arrival at the ED, 30-day readmission, intensive care unit (ICU) admission, length of hospital stay (LOS), temperature in the ambulance and at the ED, systolic blood pressure in the ambulance and at the ED, thrombocyte count at the ED, positive blood cultures, and ceftriaxone resistance. These clinical parameters were chosen as they have been described in the literature as being associated with mortality in septic patients with and without cancer.1,12,15,20-28 Descriptive statistics were used to describe patient characteristics, presented as frequency (proportion), mean ± standard deviation (SD), or as median (interquartile range (IQR)). Comparisons between the groups of patients with and without cancer were performed using the Pearson Chi-square. Confounders were identified and corrected for through logistic regression analyses. Power calculation showed that we were able to detect at least a 3.9% difference in 28-day mortality by using our sample size of 2,658 patients with a power of 80% (two-sided testing). All analyses were performed in IBM SPSS Statistics 22.0 (Chicago, USA), with p < 0.05 considered significant.
Ethics
The study protocol of the PHANTASi trial was approved by the medical ethical committee of the Amsterdam University Medical Centre, Location VU University Medical Centre, the coordinating centre, and all ethical committees of each participating hospital. Due to the complexity of the PHANTASi trial, the ethics committees granted approval to obtain deferred consent when necessary. Informed consent before study enrolment or deferred consent was obtained from all patients or their legal representatives or surrogates. All efforts were made by EMS personnel to obtain informed consent before study inclusion.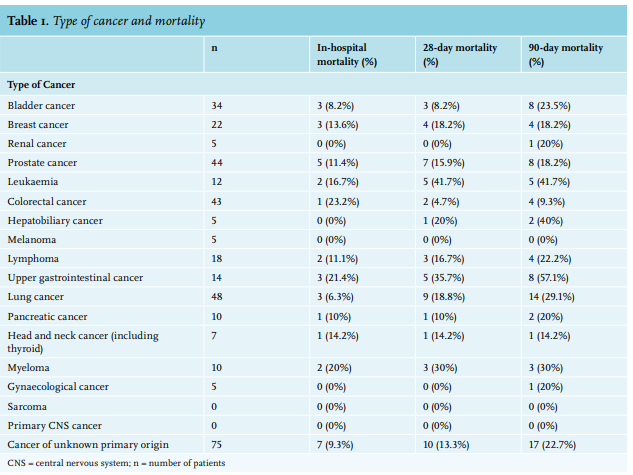
RESULTS
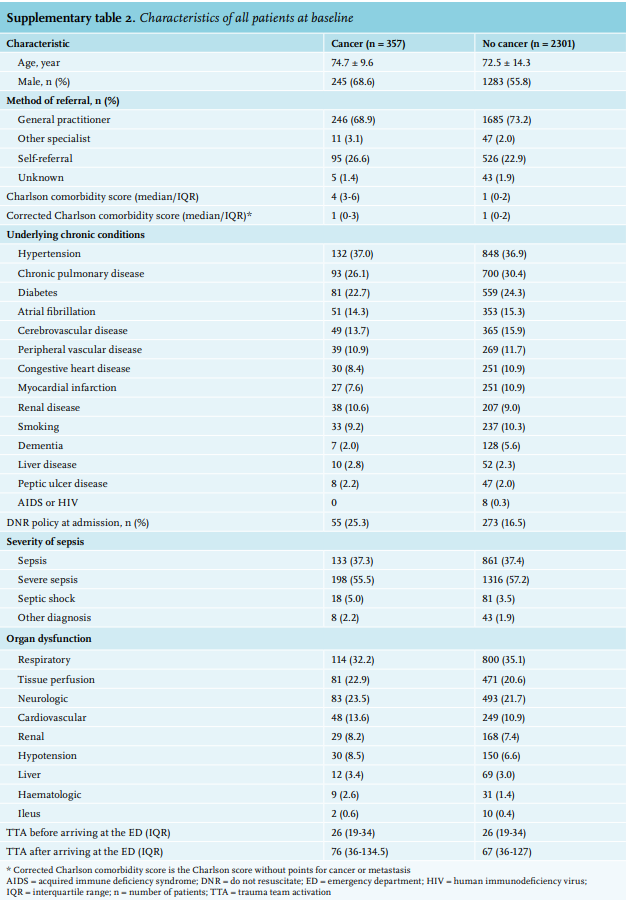
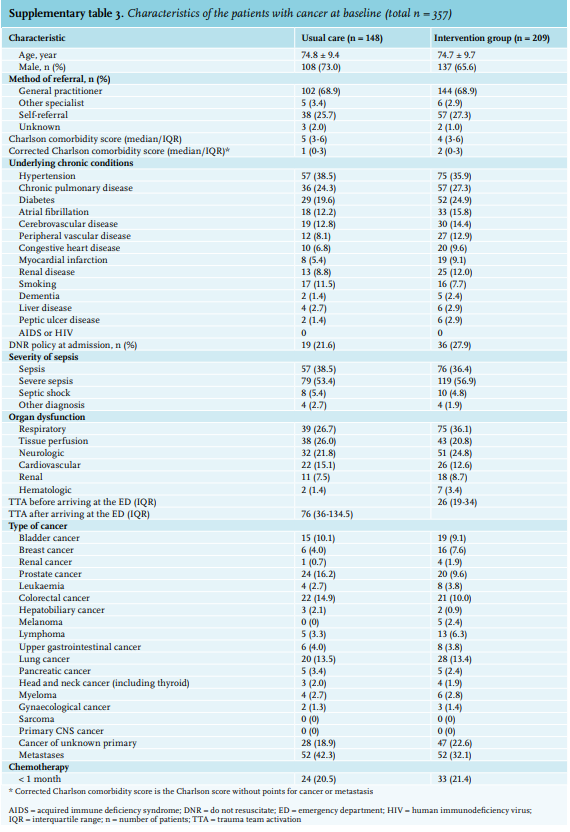
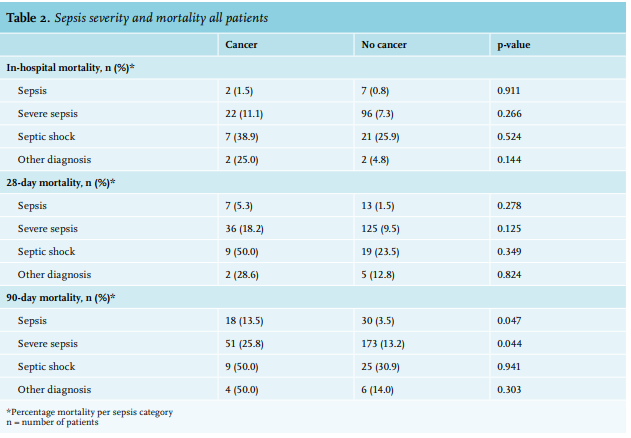
Among all included subjects in PHANTASi trial, 357 (13.4%) were diagnosed with cancer within five years prior to their inclusion in the study, while the remaining 2,301 (86.6%) patients did not. The most common types of cancer were colorectal, prostate, and lung cancer. Table 1 provides an overview of the mortality rates per cancer type. In the group of patients with cancer, 148 patients (41.5%) were in the usual care group and 209 patients (58.5%) were in the intervention group with a mean age of 74.8 ± 9.4 years and 74.7 ± 9.7 years, respectively. See table 2 and 3 for more details on sepsis severity and mortality.
Mortality
Difference between patients with and without cancer in the total population
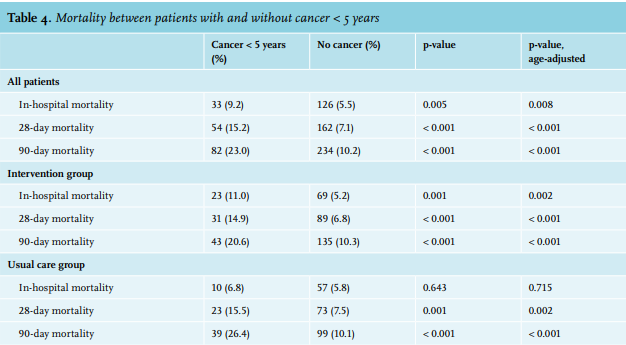
Overall, in patients with and without cancer there was a significantly higher age-adjusted in-hospital mortality (9.2% vs. 5.5%, respectively; p = 0.008), 28-day mortality (15.2% vs. 7.1%, respectively; p < 0.001) and 90-day mortality (23.0% vs. 10.2%, respectively; p < 0.001) (table 4).
Usual care group
Among patients in the usual care group, the age-adjusted in-hospital mortality between patients with and without cancer did not differ significantly (6.8% vs. 5.8%, respectively; p = 0.715). However, those with cancer had a significantly higher age-adjusted 28-day mortality (15.5% vs. 7.5%, respectively; p = 0.002) and 90-day mortality (26.4% vs. 10.1%, respectively; p < 0.001) than those without cancer (table 4).
Intervention group
Among subjects in the intervention group, patients with cancer had a significantly higher age-adjusted mortality than patients without cancer in all outcomes: in-hospital mortality (11.0% vs 5.2%, respectively; p = 0.002), 28-mortality (14.9% vs 6.8%, respectively; p < 0.001) and 90-day mortality (20.6% vs 10.3%, respectively; p < 0.001) (table 4).
Patients with cancer < 5 years
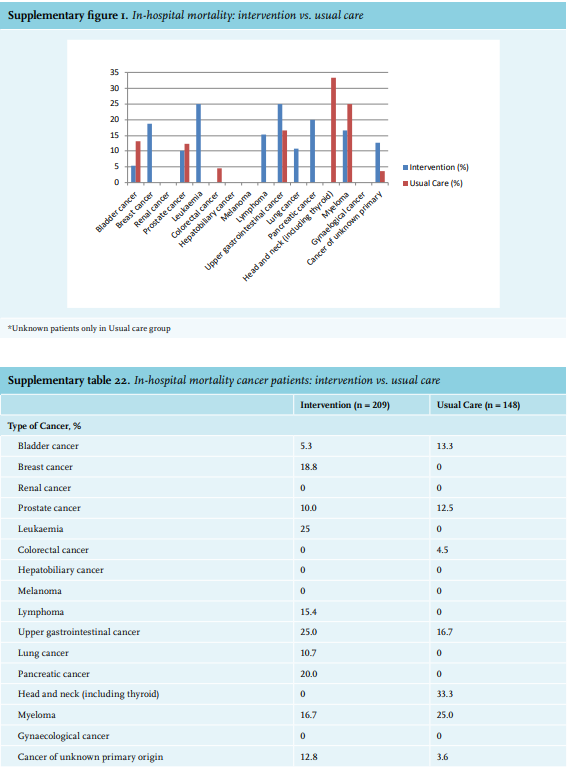
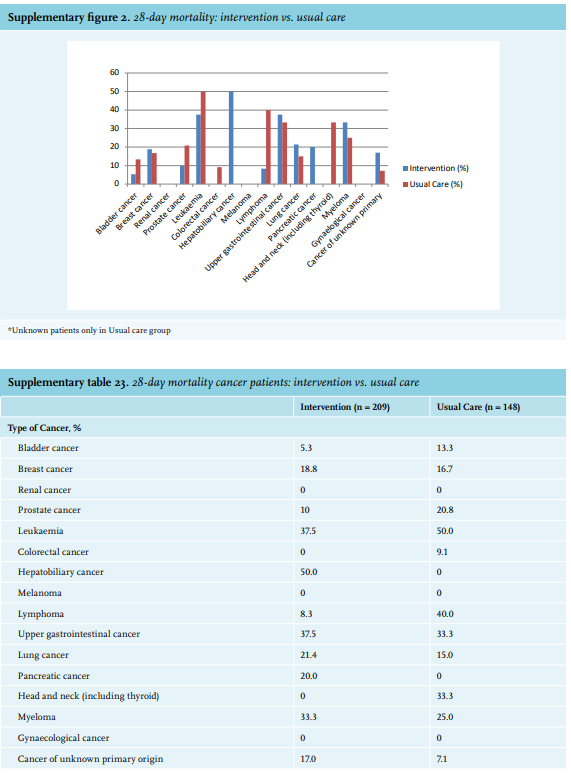
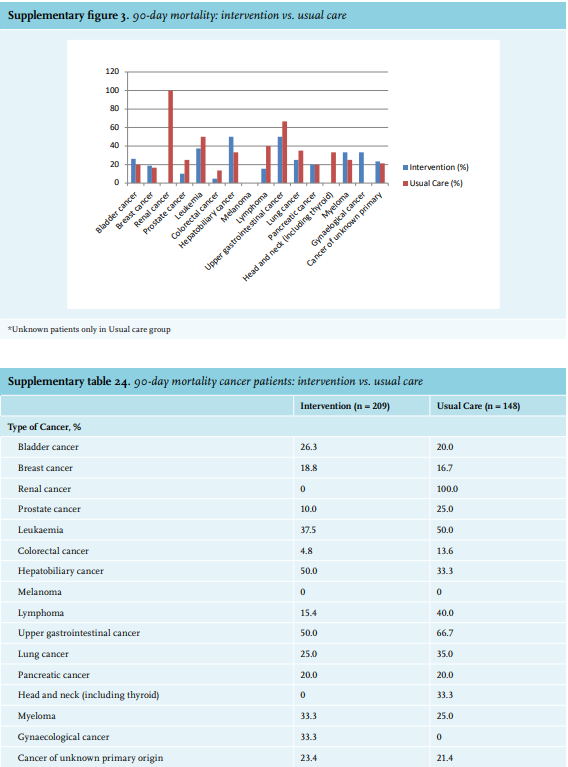
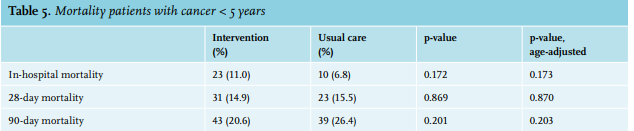
In the group of patients with cancer, there were no significant differences between the usual care compared to the intervention group for age-adjusted in-hospital (6.8% vs 11.0%, respectively; p = 0.173), 28-day (15.5% vs 14.9%, respectively; p = 0.203) and 90-day (26.4% vs 20.6%, respectively; p = 0.870) mortality (table 5). See supplementary figures 1-3 and supplementary tables 21-24 for more details on mortality.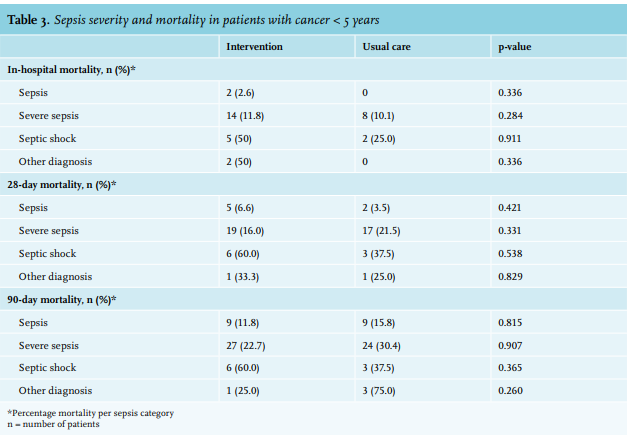
Secondary outcomes
Difference between patients with and without cancer
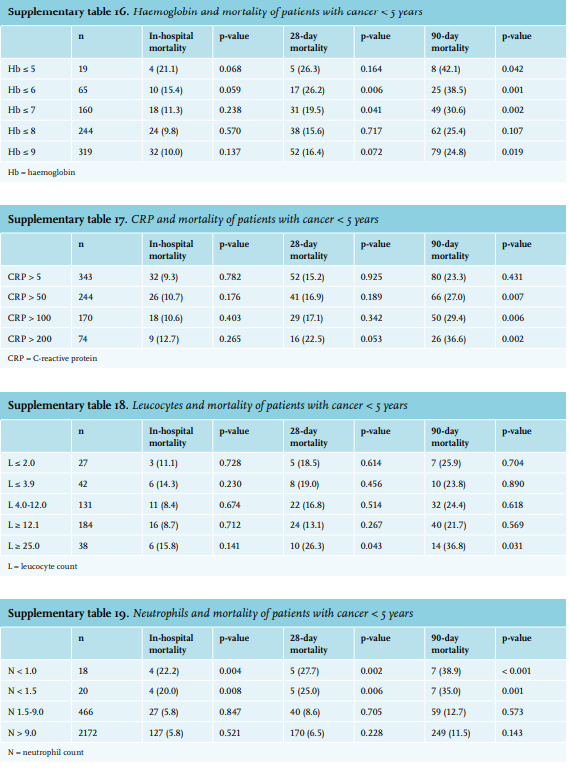
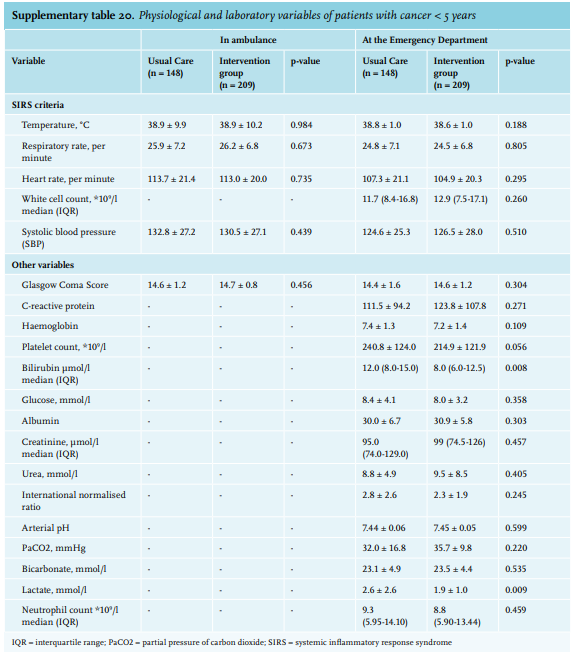
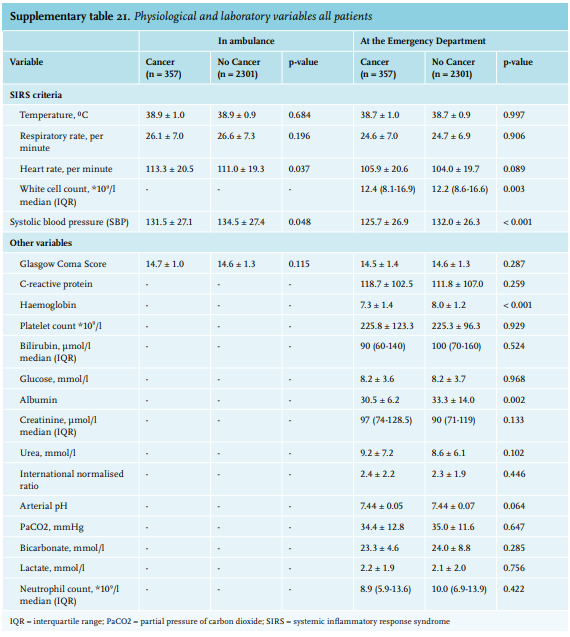
No significant difference was observed for LOS between subjects with and without cancer (8.1 vs. 8.0 days, p = 0.867). An overview of vital parameters and laboratory findings of both groups can be found in the supplementary tables 2 and supplementary tables 11-21.
Usual care group
In the usual care group, no significant difference was observed between patients with and without cancer in terms of the frequency of ICU admissions (p = 0.589) and 30-day readmissions (p = 0.076). The average LOS in patients with vs. without cancer were 9 days (IQR 3.25-9.0) and 7.8 days (IQR 3.0-9.0), respectively (p = 0.922).
Intervention group
In the intervention group, there was no significant difference in frequency of ICU admissions or 30-day readmissions between patients with and without cancer (p = 0.155 vs. p = 0.290, respectively). Mean LOS in patients with vs. without cancer were 8.3 days (IQR 3.25-9.0) and 8.2 days (IQR 3.0-9.0), respectively (p = 0.898).
Patients with cancer < 5 years: usual care group vs. intervention group
Patients with cancer had a median time to antibiotics of 26 minutes (IQR 19-34) prior to arrival at the ED in the intervention group; in the usual care group, patients had a median time to antibiotics of 76 minutes (IQR 36-134.5) after arriving at the ED, leading to a mean time advantage of 102 minutes for the intervention group.
In patients with cancer, there was no significant difference in ICU admissions (p = 0.947) between the intervention group and the usual care group. The average LOS in the intervention group and usual care group was 8.3 ± 8.1 days and 7.9 ± 10.7 days, respectively (p = 0.714). However, 30-day readmission was significantly lower in the intervention group (p < 0.031).
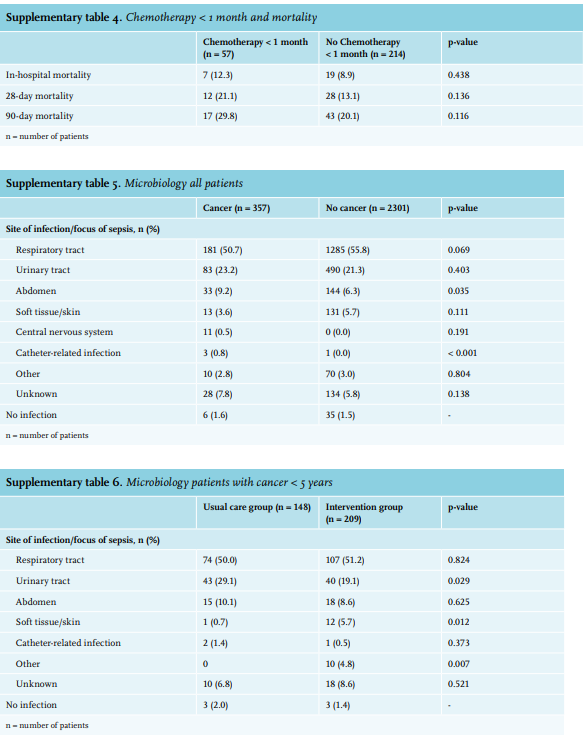
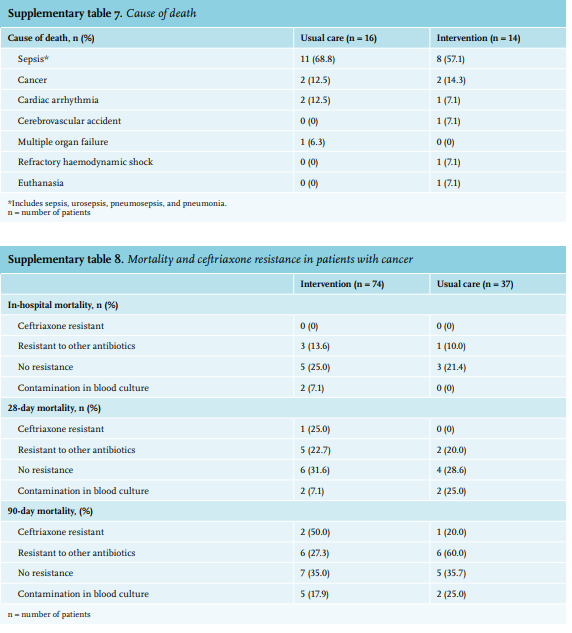
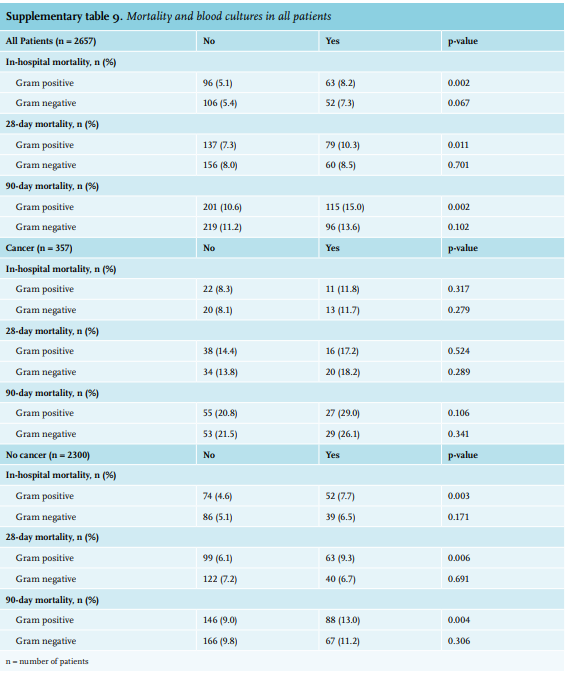
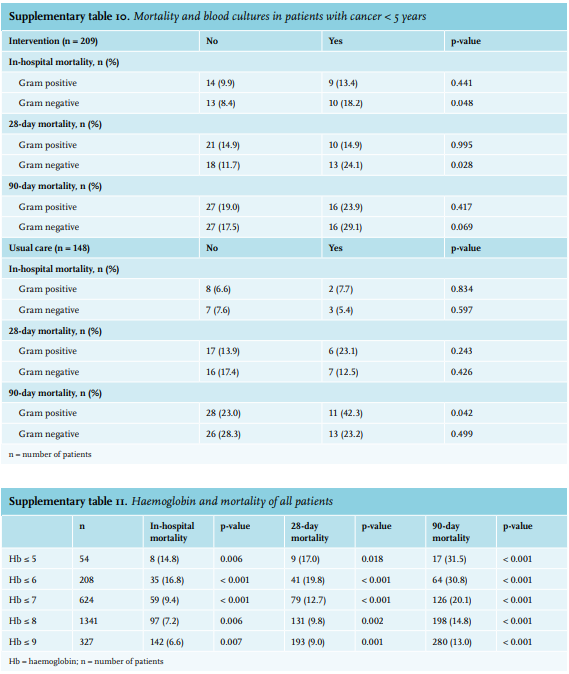
Chemotherapy one month prior to ED was not significantly correlated with increased in-hospital, 28-day, or 90-day mortality (supplementary tables 3 and 4). Information on micriobiological data can be found in supplementary tables 5-10.
DISCUSSION
To the best of our knowledge, this is the first study to compare the effect of prehospital antibiotics in septic patients with and without cancer. In the complete patient population included in the PHANTASi trial, when comparing patients with and without cancer, we found a significantly higher in-hospital (9.2% vs. 5.5%, respectively), 28-day (15.2% vs. 7.1%, respectively) and 90-day (23.0% vs. 10.2%, respectively) mortality rates. Despite receiving their first dose of intravenous antibiotics 102 minutes earlier, septic patients with cancer in the intervention group did not have significantly different mortality rates to those receiving usual care. However, septic patients with cancer in the intervention group did have a significantly lower readmission rate.
Previous studies compared clinical outcomes of patients with and without sepsis. However, these studies only included non-ED patients or patients without prehospital intravenous antibiotics.20 Nurse-led protocols for sepsis and cancer patients have been shown to be an effective, safe, and sustainable method for early antibiotic administration but have not demonstrated a significant decrease in mortality.29 Similarly, in the PHANTASi trial, EMS personnel were trained in the recognition of sepsis, which lead to an improvement in the recognition of sepsis as well as time to antibiotics.
Following SACT, cancer patients may produce vasoactive pro-inflammatory cytokines such as interleukin (IL)-2, IL-6, and tumor necrosis factor. This, together with the ability of the malignancy itself to mimic an infective driver of SIRS, can give a false impression that a cancer patient has sepsis.30 This alternative pathway is responsible for a proportion of sepsis presentations in patients with cancer and may partially explain the ineffective prehospital antibiotics on clinical outcomes in these patients.
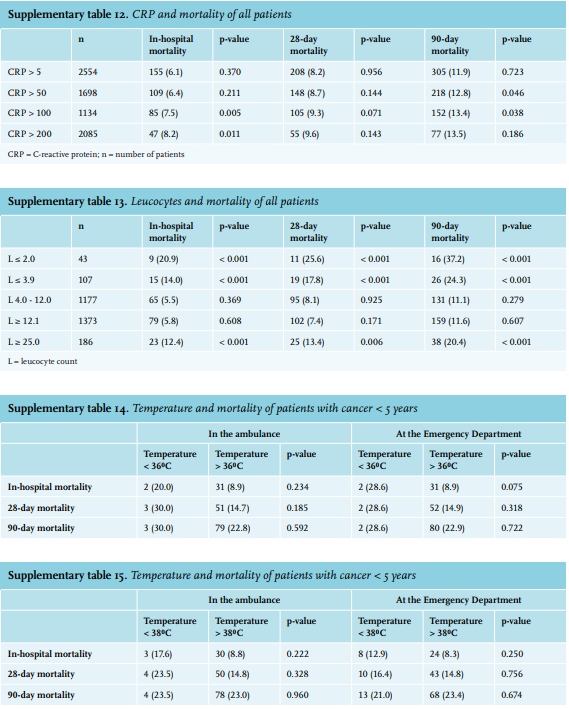
Our study has a number of strengths. First, this study had a large sample size of septic patients of whom 357 had cancer. Previous studies in similar populations had significantly smaller sample sizes.20,31 Second, this is the first study to compare the effect of prehospital intravenous antibiotics by EMS personnel in septic patients with and without cancer. Other studies have investigated either septic patients1-3,32 or cancer patients with febrile neutropenia.11,12 Third, a retrospective chart analysis was conducted on PHANTASi trial data by two acute physicians and an infectious diseases specialist, which allowed us to efficiently include patients with sepsis. In addition, in the PHANTASi trial, sepsis severity was classified by reviewing available information such as admission letters, vital parameters, lab results, and discharge papers available in electronic patient charts.7 These thorough reviews ensured high-quality samples and data. Fourth, this study investigated several factors associated with mortality in septic patients with and without cancer, described in literature, including time to antibiotics, systolic blood pressure, temperature, thrombocyte count, haemoglobin levels, C-reactive protein levels, leucocyte count, neutrophil count, gram-negative and gram-positive bacteraemia, type of cancer, and chemotherapy prior to ED admission.1,12,15,20
Septic patients have an increased risk of readmission and unplanned admissions after discharge. This risk is higher in septic patients with cancer.23 Interestingly, we found a lower 30-day readmission in cancer patients who received prehospital antibiotics compared to those who did not. This same trend was found in the PHANTASi trial.7 A possible explanation has been suggested for this effect that early antibiotics administration prevents the development of organ failure during the initial hospital admission which, in turn prevents readmission.33
Despite the smaller sample size of studies mentioned and minor differences in categorising cancer types, the main groups of cancer are similar in our study compared to others.15,20
Despite these strengths, our study also has a few limitations. First, our study was a sub-analysis of the PHANTASi trial, which inevitably leads to limitations. Although we did not apply stratified randomisation on the basis of cancer, we had a relatively large sample size compared to other studies on septic patients with cancer. Second, we had relatively limited amount of data on the cause of death as we did not have long-term follow-up. We could only retrieve data on in-hospital mortality and documented mortality by family members. Third, we included all patients with cancer in the past five years rather than only those with a currently an active form of malignancy due to absence of data. Despite these limitations, we did find a significantly higher mortality rate in septic patients with cancer (five years prior to the ED admission) compared to those who are cancer free.
Early antibiotic administration remains a paradigm of care for cancer patients presenting with sepsis and many studies have demonstrated the challenges of achieving this through routine care. This study shows that paramedic administration of intravenous antibiotics is a safe and effective strategy for decreasing the time to intravenous antibiotics in septic patients. However, in this unselected group of cancer patients with sepsis, this did not improve mortality and further studies are required to determine markers of high-risk patients who will benefit from this intervention.
CONCLUSION
Septic patients with cancer had higher in-hospital, 28-day, and 90-day mortalities compared to those without. Prehospital antibiotics did not lead to a decrease in mortality in patients with cancer, but did reduce 30-day readmission rate. Future studies should focus on optimisation of the treatment of septic patients with active malignancy.
* For supplementary tables and figures, see appendix
DISCLOSURES
All authors declare no conflict of interest.
REFERENCES
APPENDIX