CASE REPORT 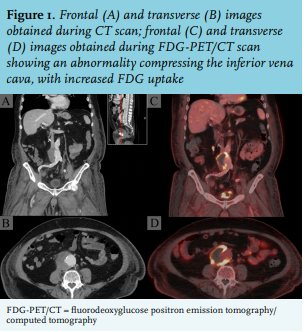
A 75-year-old male was referred to our emergency room because of dyspnoea, hypotension, and a swollen leg. His medical history included type 2 diabetes mellitus, stroke, hypertension, and colon cancer two years prior, treated with laparoscopic resection and adjuvant chemotherapy. The patient complained of progressive fatigue over the last few weeks followed by swelling of the left leg, which occurred one day prior to his visit, with progressive dyspnoea afterwards. His blood pressure was 70/50 mmHg, heart rate 115 bpm, temperature 36.2°C, respiratory rate 32 breaths per minute, and peripheral oxygen saturation 95%. Palpation of the abdomen was painful, but there was no abdominal rigidity. The left lower leg was swollen and erythematous but not noticeably warmer than the right leg. Laboratory testing showed high inflammatory markers (C-reactive protein 193 mg/l, leucocyte count 24.4 × 109/l). Ultrasound of the left leg revealed deep vein thrombosis. Therefore, a pulmonary embolism was suspected, which was confirmed on computed tomography (CT) imaging.
Low molecular weight heparin therapy was initiated in conjunction with ceftriaxone because concomitant sepsis was presumed. Blood pressure improved with intravenous fluid administration; therefore, we concluded that hypotension was mainly caused by sepsis and not obstructive shock secondary to the pulmonary embolism. Hence, no thrombolysis was initiated. Within several days the dyspnoea abated, blood pressure normalised, and heart and respiratory rates improved. Surprisingly, blood cultures (which were taken at admission because of the high inflammatory markers) became positive for Salmonella enterica subsp. enterica serotype Enteritidis, sensitive for ceftriaxone and ciprofloxacin. When asked, the patient mentioned that he had severe, self-limiting diarrhoea six weeks prior to current admission. A few days later, the contralateral right leg also became swollen, raising the suspicion of compression of the inferior vena cava. Indeed, further imaging demonstrated compression of the inferior vena cava by a fluorodeoxyglucose (FDG)-positron emission tomography (PET)-positive abnormality (figure 1).
WHAT IS YOUR DIAGNOSIS?
See page 345 for the answer to this photo quiz.